Page 25 of 32
OP10.7 | Blindness, Vision Impairment, NPCB and Vision 2020 — SDL Guide (Part 2)
Investigation and Assessment of the Visually Impaired Patient
Assessing a patient with visual impairment requires both a clinical and a functional evaluation. The clinical evaluation establishes the cause and potential reversibility; the functional evaluation determines the impact on daily activities and the need for rehabilitation. The distinction between these two dimensions of assessment is not merely academic — it has direct management consequences. A patient with VA 6/60 due to a dense cataract (clinical evaluation: treatable cause, highly reversible) needs a completely different management pathway from a patient with VA 6/60 due to end-stage glaucomatous optic atrophy (clinical evaluation: irreversible cause, no treatment restores lost field) — yet both patients may have identical functional limitations in daily life, and both need the functional evaluation to determine what rehabilitation support they require. The pinhole test is the single most important bedside screen in this context: it separates refractive from organic causes of reduced vision in under a minute, at zero cost. A VA that improves from 6/60 to 6/12 with a pinhole tells you immediately that the patient's vision could be restored to near-normal with spectacles — a correctable cause requiring optometry, not ophthalmology. A VA that does not improve with a pinhole points to a structural cause requiring further clinical workup. Every student should perform the pinhole test reflexively on every patient with reduced visual acuity before arriving at any diagnostic conclusion.
Visual acuity assessment:
- Distance VA: Snellen chart at 6 m (or logMAR/ETDRS chart for research settings). Record each eye separately with the current correction.
- Near VA: Jaeger card or N-notation at 33 cm.
- Pinhole test: VA improvement with pinhole = refractive component (potentially correctable); no improvement = organic (structural) cause.
- Below 6/60: test for counting fingers (CF) at 1–3 m, hand movements (HM), perception of light (PL/PLPR), or no perception of light (NPL).
Visual field assessment:
- Confrontation visual field testing: a rapid bedside screen using the examiner's hands as targets in four quadrants — detects gross hemianopias and large scotomas.
- Formal perimetry (Humphrey automated perimetry or Goldmann kinetic perimetry): quantifies the visual field for glaucoma monitoring, retinitis pigmentosa staging, and disability certification.
Low vision assessment:
A person with low vision has VA between 6/18 and 3/60 (or restricted visual field <20°) despite best possible treatment and optical correction, and uses or is potentially able to use vision for planning and execution of tasks. Low vision assessment measures functional vision with magnifiers, telescopes, and CCTV aids, to determine appropriate rehabilitation devices.
NPCBVI survey tools: Population surveys use the Snellen chart with tumbling E optotypes or Landolt C (for non-literate populations) under standardised lighting. The INBVS used a comprehensive protocol: Snellen VA, auto-refraction, slit-lamp examination, intraocular pressure, and dilated fundus examination — to both categorise visual impairment and attribute it to a specific cause.
Diagnosis and Differential: Avoidable vs Unavoidable Blindness
The most clinically important diagnostic task in the assessment of a visually impaired patient, from a public health perspective, is determining whether the cause of vision loss is avoidable — specifically, whether a simple intervention could restore or preserve vision. This determination drives referral decisions and programme planning. The concept of avoidable blindness is not merely an academic taxonomy — it is the organising principle of every national and global blindness prevention programme, including NPCBVI and Vision 2020. By quantifying how much of the blindness burden is avoidable, programme planners can calculate the return on investment for specific interventions: if 66% of blindness is due to cataract and cataract surgery has a 90% success rate and costs approximately ₹1,500 per procedure in the public sector, then the cost-effectiveness of scaling up cataract surgery is extraordinarily high compared to almost any other health intervention. This is why cataract surgery is the flagship component of NPCBVI. For you as a clinician, the avoidable vs unavoidable distinction determines whether your primary role is treatment (cataract, refractive error, infections) or rehabilitation (retinitis pigmentosa, geographic atrophy, phthisis). Both roles are legitimate and important, but conflating them — for example, telling a patient with retinitis pigmentosa that their vision can be restored with treatment — causes harm through false hope and delayed rehabilitation uptake.
Avoidable blindness — treatable with intervention:
- Cataract: Visually significant cataract causing VA <6/60 can be treated with surgery (phacoemulsification or MSICS under local anaesthesia, an outpatient procedure) with restoration of near-normal vision in the great majority of cases. Delayed cataract surgery is the single largest cause of avoidable blindness in India.
- Uncorrected refractive error: A patient with VA 6/60 due to high myopia or hypermetropia who improves to 6/6 with a pinhole = uncorrected refractive error; spectacles will restore vision completely. This is the most common cause of visual impairment and the cheapest to correct.
- Glaucoma: Blindness can be prevented (or its progression arrested) with timely diagnosis and treatment (pressure-lowering drugs, laser, or surgery) — though existing visual field loss is irreversible. Early detection by routine IOP screening and fundus examination is key.
- Corneal blindness from treatable infections: Herpes simplex keratitis treated with topical acyclovir; vitamin A deficiency treated with supplementation (before scarring); bacterial keratitis with appropriate antibiotics.
Avoidable blindness — preventable:
- Vitamin A deficiency / xerophthalmia: prevented by supplementation and dietary education.
- Trachoma: prevented by the WHO SAFE strategy (Surgery for trichiasis, Antibiotics (azithromycin), Facial cleanliness, Environmental improvement).
- Diabetic retinopathy: prevented by glycaemic and blood pressure control; screened by dilated fundus examination in all diabetics.
Unavoidable blindness:
- Retinitis pigmentosa (inherited; no cure, though gene therapy is investigational).
- Advanced AMD with complete macular atrophy (geographic atrophy stage).
- Severe optic atrophy from longstanding trauma or ischaemia.
- Phthisis bulbi.
For these patients, low vision rehabilitation is the appropriate intervention: magnifiers, screen readers, mobility training, occupational therapy, and social welfare support (disability certification, assistive devices, benefits under the Rights of Persons with Disabilities Act, 2016).
SELF-CHECK
Of the following, which represents 'avoidable blindness' that can be PREVENTED before onset rather than treated after it occurs?
A. Cataract causing VA <3/60 in a 70-year-old
B. Advanced glaucoma with complete visual field loss in a 65-year-old
C. Vitamin A deficiency causing keratomalacia in a 3-year-old on a rice-based diet
D. Retinitis pigmentosa causing progressive night blindness in a 25-year-old
Reveal Answer
Answer: C. Vitamin A deficiency causing keratomalacia in a 3-year-old on a rice-based diet
Vitamin A deficiency and xerophthalmia are PREVENTABLE by vitamin A supplementation (NPCBVI schedule) and dietary education — the blindness never needs to occur. Cataract is TREATABLE (but cannot be prevented); advanced glaucomatous field loss is irreversible (the blindness has already occurred — future progression can be prevented but not the current loss); retinitis pigmentosa is currently unavoidable (inherited). Prevention = the cause never leads to vision loss at all.
National Programme for Control of Blindness and Visual Impairment (NPCBVI)
The National Programme for Control of Blindness (NPCB) was launched in India in 1976 as one of the earliest national blindness control programmes in the developing world. It was renamed the National Programme for Control of Blindness and Visual Impairment (NPCBVI) in 2017 to reflect its expanded scope to include all visual impairment, not just blindness. The programme is centrally sponsored and operates through district hospitals, CHCs, PHCs, and partnerships with NGO-run eye hospitals. Understanding NPCBVI in depth — its historical origins, its structural components, its targets, and its implementation mechanisms — is a CBME OP10.7 competency and a frequent examination topic in community medicine as well as ophthalmology. The programme was launched in 1976 because India's blindness prevalence at that time was estimated at approximately 1.4% of the population — a figure that placed India among the highest-burden countries in the world. Cataract was already recognised as the leading cause, and the architects of the programme correctly identified that the bottleneck was not the availability of surgical technique (cataract surgery had been performed in India for centuries) but the lack of organised delivery infrastructure reaching rural populations. The programme therefore focused primarily on building district-level eye surgery capacity, training surgeons and ophthalmic assistants, and organising outreach camps to bring surgical services to rural areas where patients lacked the means to travel. Over the subsequent four decades, this infrastructure investment — combined with the introduction of intraocular lens implantation (replacing aphakic spectacles, which had very poor compliance) and the shift from intracapsular to extracapsular and then phacoemulsification surgery — transformed the cataract surgical landscape in India. The programme is centrally sponsored and operates through district hospitals, CHCs, PHCs, and partnerships with NGO-run eye hospitals.
Provided image
Programme objectives (NPCBVI):
1. To reduce the prevalence of blindness from 1.1% (1986–89 survey) to 0.3% by 2020 (a target partly achieved — INBVS 2015–19 estimates prevalence of <3/60 blindness at ~1.99% in the 50+ age group by the older broader criterion, still indicating substantial burden).
2. To develop eye care infrastructure — district hospitals with functional eye operation theatres, adequate surgical equipment, and trained ophthalmologists.
3. To develop human resources — training of ophthalmic assistants, optometrists, and community health workers for vision screening.
4. To strengthen eye banking and corneal transplantation services.
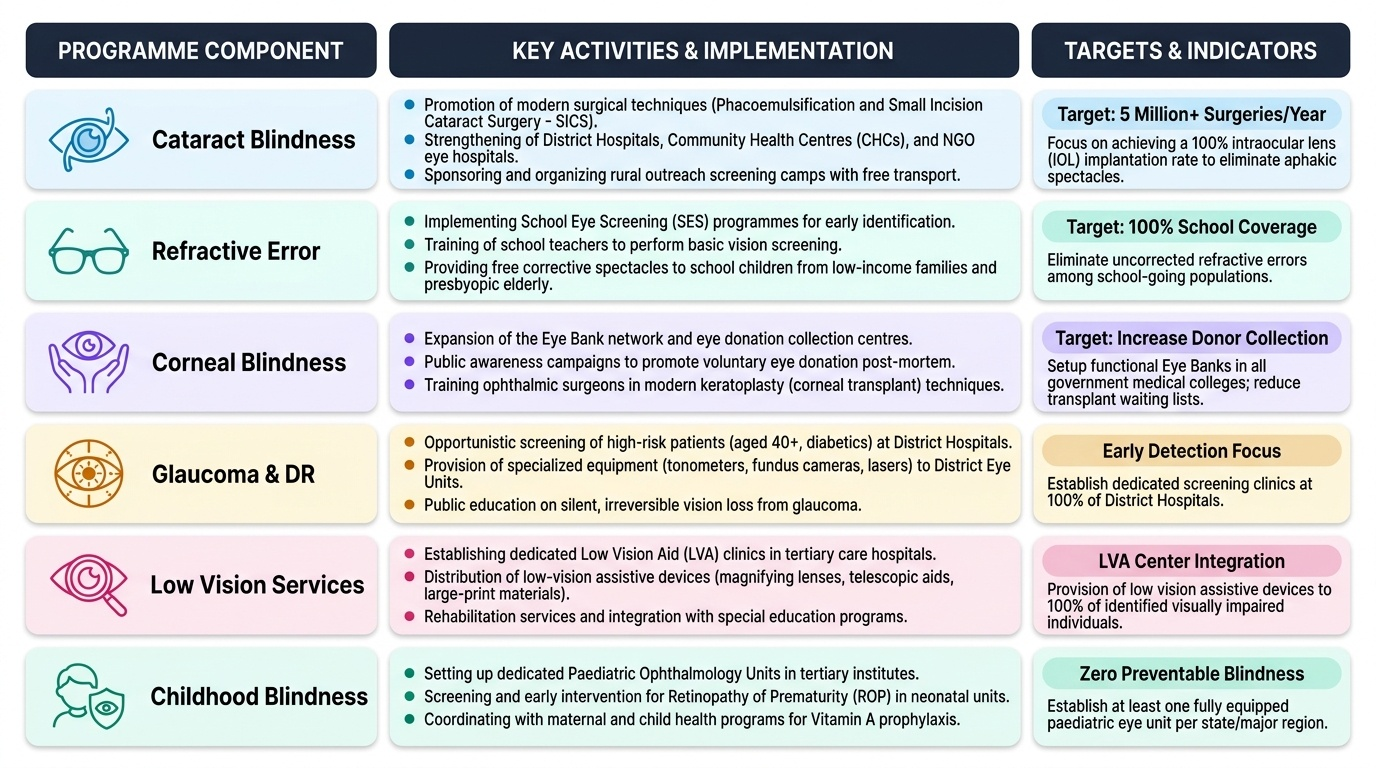
Programme components:
1. Cataract surgery: The flagship component. Free cataract surgery with IOL implantation is provided at district hospitals, vision centres, and NPCBVI-empanelled NGO hospitals. The target is to progressively increase the cataract surgical rate (CSR) and reduce the cataract backlog. Surgical outreach camps bring services to rural areas.
2. Refractive error management: School eye screening for children; distribution of spectacles at subsidised cost; training of optometrists at district level.
3. Corneal blindness: Strengthening of eye banks, promotion of eye donation (pledges and actual donations), and support for penetrating keratoplasty at tertiary centres.
4. Glaucoma: Screening for glaucoma in districts with dedicated glaucoma management protocols; free anti-glaucoma medications at district hospitals.
5. Childhood blindness: Vitamin A supplementation (100,000 IU at 6 months; 200,000 IU every 6 months until 5 years — described in OP10.4 SDL), school eye health screening, universal newborn screening for retinopathy of prematurity (ROP) in eligible NICUs.
6. Low vision: Training and provision of low vision aids (magnifiers, telescopes, screen readers) and rehabilitation services through district-level vision rehabilitation centres.
7. Diabetic retinopathy: Screening programmes integrated with NCD clinics at district hospitals.
District implementation: The District Blindness Control Society (DBCS) is the operational unit — chaired by the district collector and involving the civil surgeon, ophthalmologists, NGOs, and community representatives. The DBCS plans and monitors the annual programme, including the cataract surgery target, outreach camps, school screening, and eye banking activities.