Page 1 of 30
OP2.1 | Common Lid Disorders: Aetiology, Features and Treatment — SDL Guide
Learning Objectives
- Describe the aetiology and distinguishing clinical features of hordeolum externum and hordeolum internum
- Explain the types, causes and ocular consequences of ectropion, entropion and lagophthalmos
- Describe the clinical features and subtypes of blepharitis
- Distinguish preseptal cellulitis from orbital cellulitis and explain the management of each common lid disorder
- Apply a systematic approach to examining a patient with a red, swollen eyelid
INSTRUCTIONS
Diseases of the eyelid account for a large proportion of ophthalmic outpatient consultations in India. Recognising and correctly classifying lid disorders — from a simple stye to preseptal cellulitis — prevents missed diagnoses and avoids the serious complication of orbital or intracranial spread. This module builds directly on your Year-1 anatomy of the orbit and eyelid and integrates with the study of orbital cellulitis (OP2.4), thyroid eye disease (OP2.3), and lacrimal system procedures (OP2.2).
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch 1 (Diseases of the Eyelids) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch 1 (The Eyelids) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman presents to the ophthalmic OPD with a painful red lump on her right upper eyelid that appeared two days ago. She says it hurts when she blinks. On examination you find a tender, localised, pointing swelling at the lid margin with overlying skin erythema. Her visual acuity is 6/6 in both eyes, and the globe is white. Before you decide between reassurance and antibiotics, a different patient in the next cubicle has diffuse swelling of the entire upper and lower lids, cannot open her eye, and her mother says the eye 'looks pushed forward.' Same ward — but these two presentations could not have more different management urgencies. Understanding the anatomy of the eyelid and the pathological processes that affect it will let you sort them instantly.
WHY THIS MATTERS
Eyelid disorders are encountered daily in general practice, paediatric clinics, and ophthalmic OPDs across India. A hordeolum is self-limiting; blepharitis requires long-term management; entropion silently destroys the cornea if untreated; preseptal cellulitis can be managed with oral antibiotics, but failing to distinguish it from orbital cellulitis can cost a patient their vision or their life. As a final-year student rotating through ophthalmology, you are the first point of contact. These conditions will appear in your clinical postings, your professional examinations (Short and Long Cases), and in your practice as a medical officer. The NMC 2024 competency OP2.1 mandates knowledge of aetiology, clinical features, investigations and treatment of all seven conditions covered here.
RECALL
Before we proceed, revisit the following from Year-1 Anatomy and Physiology: (1) The eyelid has four layers from front to back — skin and subcutaneous tissue, orbicularis oculi muscle, tarsus (fibrous skeleton containing meibomian glands), and palpebral conjunctiva. (2) The orbital septum is a fascial sheet that runs from the orbital rim and inserts into the tarsus; it separates the preseptal space (superficial) from the orbital space (deep). (3) Sensory supply: upper lid = lacrimal, supraorbital, and infratrochlear branches of V1; lower lid = infraorbital branch of V2. (4) Motor: orbicularis oculi (lid closure) = facial nerve (VII); levator palpebrae superioris (lid elevation) = oculomotor nerve (III) with Müller's muscle (sympathetic). (5) Lymphatic drainage: medial lid → submandibular nodes; lateral lid → preauricular nodes — this matters when the lid is infected.
Clinical Presentation: Red, Swollen Lid Lesions
The clinical presentation of lid disorders spans a spectrum from a focal, painful lump at the lid margin to diffuse orbital swelling with systemic toxicity. Correct clinical reasoning starts with localising the lesion within the eyelid's anatomical compartments, because the compartment determines the diagnosis, the treatment, and the urgency. In practice, the five questions that drive the consultation are: Is the swelling focal or diffuse? Is it acute or chronic? Is it painful? Is the globe displaced forward (proptosis)? Is vision normal? A focal, tender, acute lid-margin swelling in a young adult almost always points to an infected gland. A chronic, painless, non-inflamed nodule in the mid-tarsus points to a chalazion. Diffuse lid oedema with fever in a child makes you think preseptal cellulitis. Proptosis with restricted eye movement in any age group demands immediate orbital cellulitis workup. This framework will anchor the seven conditions covered in this module.
The seven conditions in OP2.1 cluster naturally by their anatomy:
- Glandular infections: hordeolum externum (external stye), hordeolum internum
- Positional anomalies: ectropion, entropion, lagophthalmos
- Chronic inflammation: blepharitis
- Preseptal space: preseptal (periorbital) cellulitis
A consistent examination approach — visual acuity, position of the lesion (margin vs tarsus vs periorbital), palpation, eversion of the lid, and assessment of ocular motility and proptosis — will discriminate between them reliably.
Anatomy of the Eyelid and Relevant Glands
Understanding the anatomy of the eyelid is prerequisite to understanding why each disorder arises where it does. The eyelid is a multilayered structure whose precise anatomy governs gland positions, fascial planes, and therefore the clinical behaviour of infections and structural anomalies.
The anterior lamella consists of skin (the thinnest in the body, allowing rapid oedema formation) and the orbicularis oculi muscle, which is responsible for lid closure and is supplied by the facial nerve (VII). The posterior lamella consists of the tarsus — a dense fibrous plate approximately 29 mm wide, 10 mm tall in the upper lid and 5 mm tall in the lower lid — which provides the structural skeleton of the lid. Within the substance of the tarsus lie the meibomian glands (30–40 in the upper lid, 20–30 in the lower), which are specialised sebaceous glands whose ducts open at the posterior lid margin; they secrete lipid into the tear film. The orbital septum arises from the periosteum of the orbital rim and attaches to the anterior surface of the tarsus; this fibrous sheet is the critical anatomical barrier between the preseptal and orbital compartments, making it the dividing line in the cellulitis diagnosis.
At the anterior lid margin, two additional sets of glands are found: the glands of Zeis are modified sebaceous glands opening into the hair follicles of the eyelashes, and the glands of Moll are modified apocrine sweat glands also situated at the lash root. Both Zeis and Moll glands are superficial to the orbital septum, placing their infections (hordeolum externum) in the preseptal space. Meibomian gland infections (hordeolum internum) are also preseptal but deeper within the tarsus, and can point to either the skin surface or, more often, to the palpebral conjunctival surface.
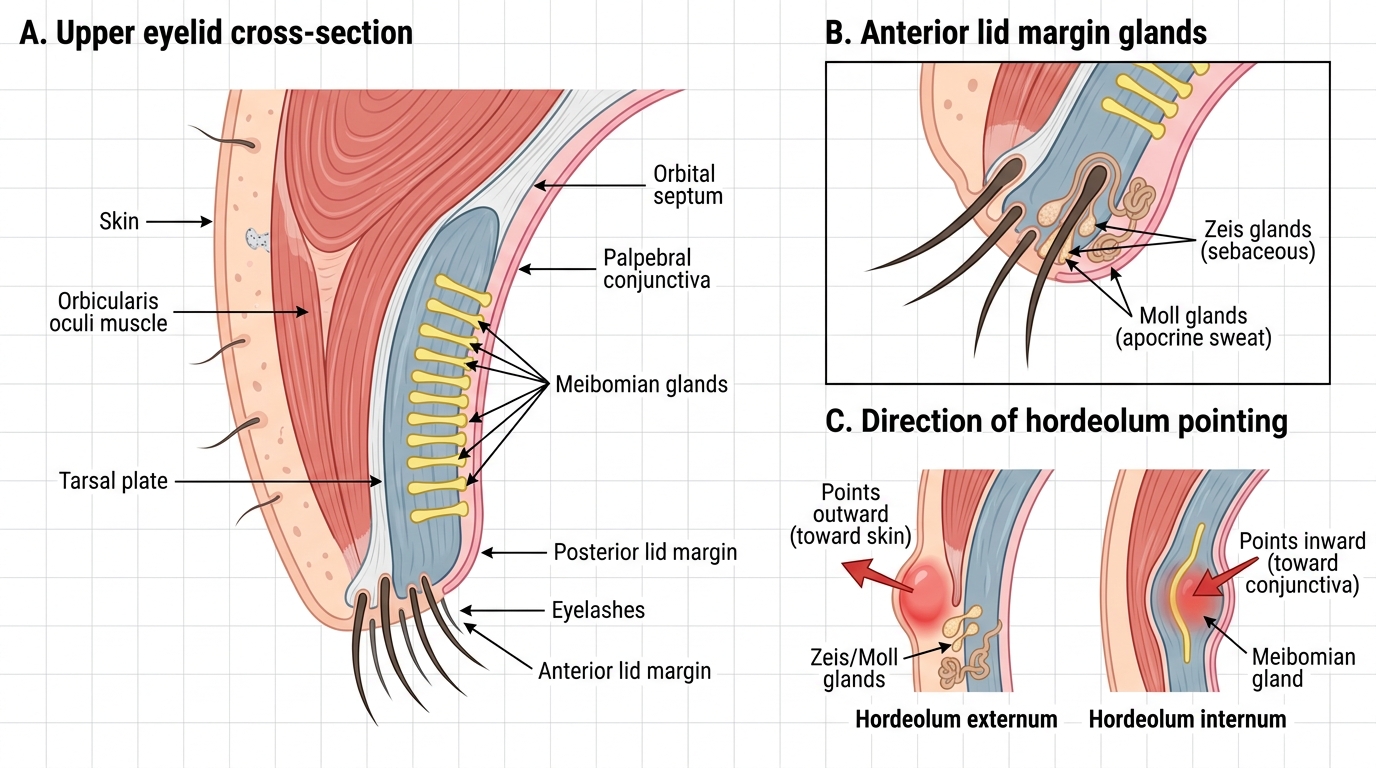
Cross-Section of Eyelid Layers and Glands
Hordeolum Externum and Internum: Aetiology and Examination
Hordeolum externum and hordeolum internum are both acute bacterial infections of eyelid glands, most commonly caused by Staphylococcus aureus, but they arise from different glands and behave differently on examination. Making this distinction guides whether the lesion will point to the skin surface or to the conjunctival surface, and influences incision technique when drainage is required.
Hordeolum externum (the common 'stye') is an acute purulent infection of the glands of Zeis or Moll at the anterior lid margin. It presents as a small, painful, erythematous nodule at the lid margin, with the swelling pointing outward toward the skin. Because Zeis glands lie in the eyelash follicles, the stye is characteristically located at the base of a lash and the lash may be lost when the abscess points and drains. On palpation, exquisite local tenderness is found over a firm-to-fluctuant swelling no more than 3–5 mm in diameter. The overlying skin is red and oedematous; a yellow pointing tip may be visible if the abscess is near rupture. An internal hordeolum must be ruled out by everting the lid.
Hordeolum internum is an acute suppurative infection of one or more meibomian glands within the tarsal plate. It is more severe than the externum because the meibomian glands are deep and surrounded by dense fibrous tarsus, making spontaneous pointing and drainage slower and more painful. The swelling is diffuse within the tarsus, extending over a larger area than the externum. When the lid is everted, a yellowish area of hyperaemia and purulent accumulation is visible on the palpebral conjunctival surface — the meibomian orifice is the usual pointing site. The external skin may show diffuse redness without a discrete follicular lesion.
Chalazion is the chronic non-infectious sequel: a lipogranulomatous reaction to retained meibomian secretion following obstruction without infection. It is painless, non-tender, and has no overlying skin inflammation — the tarsus simply feels indurated. Distinguishing a chalazion from an internal hordeolum is clinically important: the former requires intralesional steroid injection or surgical curettage; the latter requires antibiotics and, if pointing, drainage.
Treatment for both types of hordeolum begins with warm compresses (3–4 times daily for 5–10 minutes) to promote pointing and drainage. Topical antibiotic ointment (e.g., chloramphenicol or fusidic acid) to the lid margin prevents secondary spread. If the lesion does not spontaneously drain within 1–2 weeks, or if it is causing significant discomfort, incision and curettage under local anaesthesia is performed — externum is incised vertically at the skin, internum is incised through the conjunctival surface parallel to the lid margin (to avoid dividing the tarsal fibres unnecessarily). Systemic antibiotics are not required unless there is preseptal spread.
SELF-CHECK
A 19-year-old student presents with a painful, tender, erythematous nodule at the base of an eyelash in the upper lid. On eversion of the lid, the palpebral conjunctiva appears normal. Which structure is most likely infected?
A. Meibomian gland within the tarsus
B. Gland of Zeis at the lash follicle
C. Lacrimal gland in the superolateral orbit
D. Goblet cells of the conjunctiva
Reveal Answer
Answer: B. Gland of Zeis at the lash follicle
The glands of Zeis are modified sebaceous glands situated at the base of eyelash follicles on the anterior lid margin. An acute infection here produces hordeolum externum — a stye that points externally at the skin surface, at the lash root, with a normal palpebral conjunctiva on eversion. Meibomian gland infection (hordeolum internum) presents as a deeper lesion within the tarsus with conjunctival hyperaemia on eversion. Lacrimal gland dacryoadenitis presents in the superolateral orbit, not at the lid margin.