Page 2 of 30
OP2.1 | Common Lid Disorders: Aetiology, Features and Treatment — SDL Guide (Part 2)
Blepharitis: Types, Features and Examination
Blepharitis is a chronic, often bilateral inflammation of the eyelid margins that is among the most common conditions seen in ophthalmic outpatient practice worldwide. It is classified anatomically and aetiologically into anterior blepharitis, involving the anterior lid margin and lash bases, and posterior blepharitis (meibomian gland dysfunction, MGD), involving the posterior lid margin and meibomian gland orifices. Both types can coexist, and both cause a chronic 'gritty, burning, sticking eyelids in the morning' symptom complex that significantly impairs quality of life.
Anterior blepharitis is further subdivided into staphylococcal and seborrhoeic types. In staphylococcal anterior blepharitis, the cardinal signs are hard, fibrinous 'collarettes' or crusts tightly adherent to the bases of the eyelashes that bleed when removed (hard scales); these are the toxin-mediated response to Staphylococcus aureus colonisation. There may be loss of lashes (madarosis), misdirection of lashes (trichiasis), and marginal corneal infiltrates (peripheral corneal staining at the 2, 4, 8, 10 o'clock positions — so-called 'catarrhal infiltrates' from staph exotoxin). In seborrhoeic anterior blepharitis, the scales are soft, greasy, and easily wiped off the lash bases without bleeding; it is associated with seborrhoeic dermatitis of the scalp and brows.
Posterior blepharitis (MGD) is characterised by dysfunction of the meibomian glands. On slit-lamp examination, the posterior lid margin shows telangiectasia, meibomian orifice plugging (inspissated secretions or 'meibomian caps'), and expression of turbid or toothpaste-like secretion on digital pressure over the lid margin. The meibomian lipid layer of the tear film is disrupted, leading to evaporative dry eye — a very common associated complaint. Over time, foam may appear in the tear meniscus (saponification of abnormal meibomian lipid).
Both forms are examined under the slit-lamp: the biomicroscope reveals lash changes, margin thickening, vascular engorgement, and gland secretion quality. Management hinges on lid hygiene — warm compresses to melt inspissated secretions followed by lid-margin scrubs (using baby shampoo diluted 1:10 or commercially prepared lid wipes) twice daily. Topical antibiotic ointment (chloramphenicol) is added in staphylococcal type. Systemic doxycycline 100 mg daily for 6–12 weeks is used for moderate-severe posterior blepharitis/MGD because tetracyclines have an anti-inflammatory effect on meibomian secretion and alter the lipase-producing bacteria; they are contraindicated in children and pregnant women. Lubricating eye drops address the secondary dry eye. Long-term maintenance with lid hygiene is essential, as blepharitis is incurable but controllable.
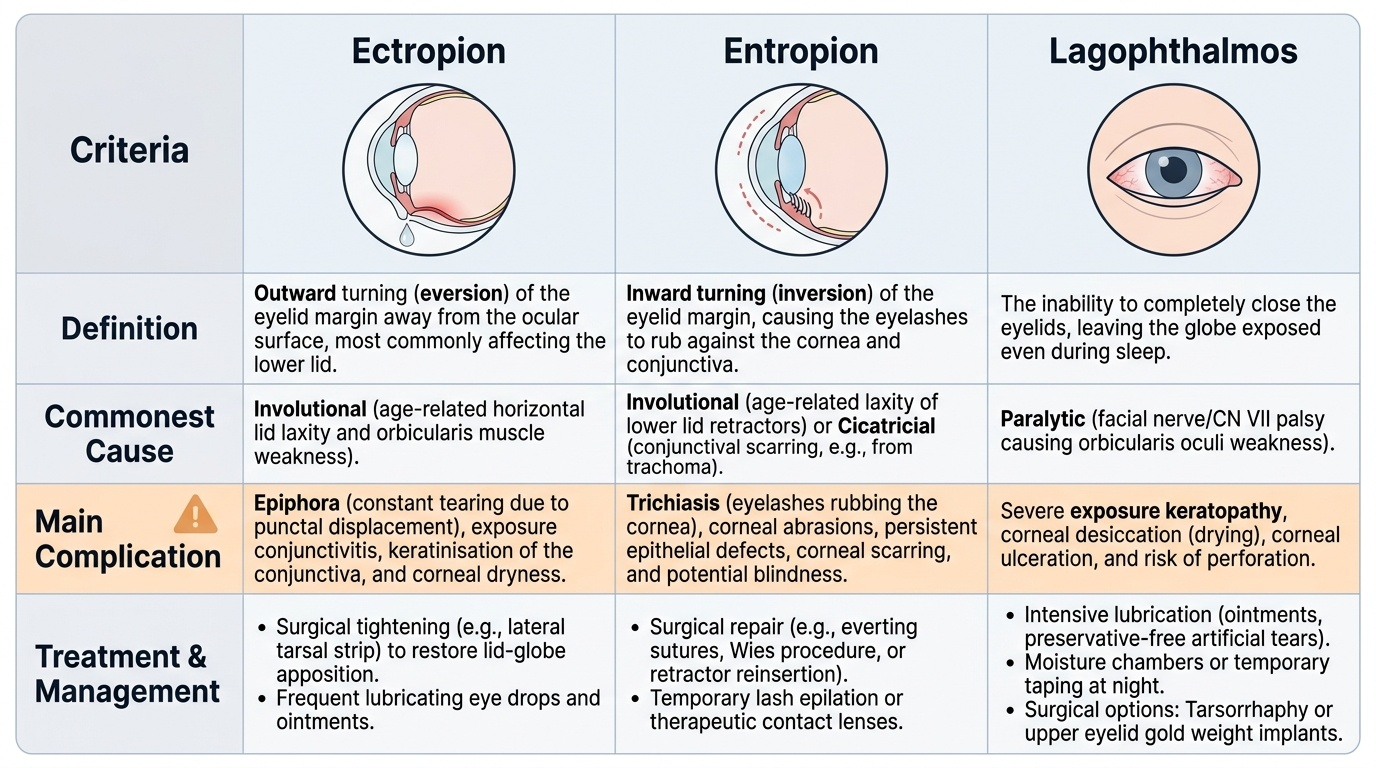
Positional Lid Anomalies: Ectropion, Entropion and Lagophthalmos
Positional lid anomalies — ectropion, entropion, and lagophthalmos — share a common threat to the eye: they all disrupt the normal relationship between the eyelid and the ocular surface, leading to exposure keratopathy, drying, and ultimately corneal ulceration and blindness if untreated. Each condition has a different anatomical mechanism and a different cause profile, but the management principle is the same: restore normal lid-globe apposition and protect the cornea.
Provided image
Ectropion is the outward turning (eversion) of the lid margin away from the globe. The lower lid is almost always affected. The four aetiological types are: (1) Involutional (senile) ectropion — the commonest; caused by horizontal lid laxity and orbicularis weakness with ageing; the lower lid hangs away from the globe, resulting in epiphora (watering eye) because the lower punctum is displaced away from the tear lake. (2) Cicatricial ectropion — caused by contracture of anterior lamellar skin or scar (burns, skin diseases, chronic dermatitis). (3) Paralytic ectropion — orbicularis palsy from facial nerve (VII) palsy; the lid cannot appose the globe. (4) Mechanical ectropion — a lid tumour or oedema weighing the lid down. On examination, the palpebral conjunctiva of the lower lid is visible and exposed, appearing thickened and keratinised over time; exposure conjunctivitis and punctal eversion are documented.
Entropion is the inward turning (inversion) of the lid margin so that the eyelashes rub against the cornea and conjunctiva — a condition known as trichiasis when the lashes themselves turn inward without lid inversion, and distichiasis when an accessory row of lashes arises from the meibomian orifices. The three subtypes are: (1) Involutional (senile) entropion — age-related laxity of lower lid retractors and horizontal lid laxity; the lid buckles inward, typically in the lower lid. (2) Cicatricial entropion — caused by conjunctival scarring; trachoma is the commonest cause worldwide (and a major cause of preventable blindness in India); other causes include chemical burns, Stevens-Johnson syndrome, ocular pemphigoid. In cicatricial entropion, the posterior lamella contracts, pulling the margin inward. (3) Spastic entropion — from overaction of the orbicularis, often with ocular irritation. On examination, lash-corneal touch is confirmed; fluorescein staining shows fine punctate epithelial erosions in the inferior cornea.
Lagophthalmos is incomplete closure of the eyelids, exposing the inferior cornea. The commonest cause is facial nerve palsy (Bell's palsy being the most frequent), where orbicularis weakness prevents voluntary lid closure. Other causes include proptosis (from thyroid eye disease or orbital mass pushing the globe forward), cicatricial changes of the posterior lamella, or post-surgical shortening of the anterior lamella. The hallmark is an area of exposed corneal epithelium inferiorly, because the Bell's phenomenon (upward rotation of the globe on attempted closure) protects the visual axis in most cases — but exposure keratitis of the inferior cornea still develops without treatment. Fluorescein staining will demonstrate the inferior corneal epithelial defect.
Management of all three is aimed at corneal protection while the underlying cause is treated. Lubricating eye drops and ointment at night are immediate protective measures. Definitive surgical correction: ectropion — horizontal lid tightening (lateral tarsal strip procedure) ± anterior lamellar repair; entropion — lower lid retractor advancement, horizontal lid tightening, or posterior lamellar grafting (mucous membrane graft for cicatricial disease); lagophthalmos — treat the underlying cause (facial nerve palsy may recover; gold weight implant in upper lid for permanent palsy; tarsorrhaphy in severe cases).
SELF-CHECK
A 68-year-old woman presents with a two-year history of bilateral watery eyes and a sensation of grittiness. Examination shows the lower lid margin is visible below the level of the globe, the inferior punctum is displaced laterally away from the tear lake, and the palpebral conjunctiva of the lower lid appears reddened and mildly keratinised. What is the most likely diagnosis and its commonest cause in this age group?
A. Entropion — involutional laxity of lower lid retractors
B. Ectropion — involutional horizontal lid laxity and orbicularis atonia
C. Lagophthalmos — age-related facial nerve weakness
D. Blepharitis — seborrhoeic gland dysfunction
Reveal Answer
Answer: B. Ectropion — involutional horizontal lid laxity and orbicularis atonia
Ectropion is outward turning of the lid margin, causing the punctum to be displaced away from the tear lake (producing epiphora despite normal tear production) and exposing the palpebral conjunctiva. Involutional (senile) ectropion is the commonest type, caused by age-related horizontal lid laxity and orbicularis atonia. Entropion involves inward turning with lash-corneal touch; lagophthalmos is incomplete lid closure. Both bilateral presentation and the age group strongly support involutional ectropion.
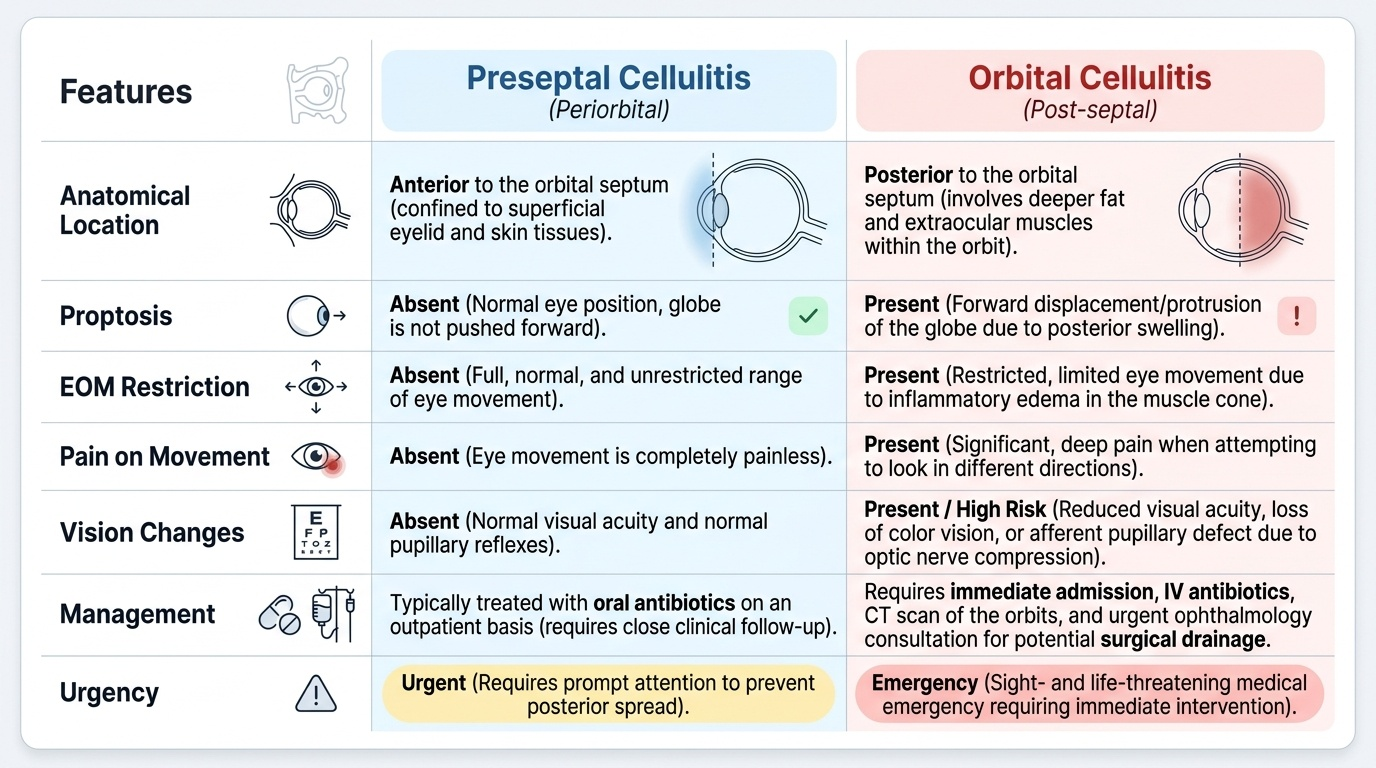
Preseptal Cellulitis: Features and Distinction from Orbital Cellulitis
Preseptal cellulitis (also called periorbital cellulitis) is an acute bacterial infection of the soft tissues of the eyelid anterior to the orbital septum. It is the most important diagnosis to make correctly among all lid disorders, because its look-alike — orbital cellulitis (posterior to the orbital septum) — is a sight- and life-threatening emergency. The orbital septum, the fibrous diaphragm you reviewed in the anatomy section, is the anatomical boundary that determines not just the name but the urgency, the route of administration of antibiotics, and the need for surgical drainage.
Provided image
Preseptal cellulitis typically follows local lid trauma, an insect bite, skin infection (impetigo), or dacryocystitis in children, or a lid hordeolum or chalazion in adults. The child or adult presents with oedema, erythema, and warmth of the eyelid(s), often with mild tenderness on palpation. Crucially, in preseptal cellulitis: the globe is NOT proptosed, extra-ocular muscle (EOM) movements are full and painless, and visual acuity is normal. There may be a low-grade fever and mild leucocytosis. CT orbits is obtained if the diagnosis is in doubt (especially in children under 5 years, who can progress rapidly).
Orbital cellulitis (posterior to septum) presents with all of the above plus the classic additional features: proptosis (forward displacement of the globe), restricted and painful EOM movements (chemosis, restriction from inflammatory oedema in the cone), and the risk of reduced visual acuity and afferent pupillary defect (optic nerve compression). Systemic signs — high fever, toxicity, elevated WBC and CRP — are more pronounced. Orbital cellulitis is a medical emergency: without urgent IV antibiotics and, often, surgical drainage of any subperiosteal abscess, the infection can spread via the orbital veins to the cavernous sinus, causing cavernous sinus thrombosis (a feared complication covered in OP2.5).
The most common cause in both is Staphylococcus aureus and Streptococcus pneumoniae; in children under 5, Haemophilus influenzae was historically important (now reduced by vaccination). Management of preseptal cellulitis: oral co-amoxiclav (amoxicillin-clavulanate) for 5–7 days plus warm compresses; hospital admission and IV antibiotics if the child is under 1 year, systemically unwell, or not improving within 24–48 hours. Management of orbital cellulitis: immediate IV antibiotics (IV co-amoxiclav or ceftriaxone ± metronidazole), CT orbits with contrast to look for subperiosteal or orbital abscess, and urgent surgical drainage if abscess is confirmed.
CLINICAL PEARL
The single most important clinical distinction in lid disease is preseptal versus orbital cellulitis. The three danger signs that tell you the infection has crossed the orbital septum are: (1) proptosis — the globe is pushed forward; (2) restricted or painful eye movements — inflammatory oedema in the orbit limits extraocular muscle function; (3) reduced visual acuity or an afferent pupillary defect — the optic nerve is at risk. Any one of these three findings in a patient with periorbital cellulitis mandates urgent CT orbits, immediate IV antibiotics, and ophthalmology senior review. A second pearl: a chalazion that does not resolve after 4–6 weeks of warm compresses and is confirmed to be in the upper tarsal plate in a patient over 50 should be biopsied, because sebaceous gland carcinoma can mimic a recurrent chalazion — do not treat the 'chalazion' with steroid injections repeatedly without biopsy.