Page 12 of 30
OP2.4 | Orbital Cellulitis — SDL Guide
Learning Objectives
- Describe the aetiology and pathways of infection in orbital cellulitis including sinusitis as the primary source
- Distinguish orbital cellulitis from preseptal cellulitis based on clinical examination findings
- Apply Chandler's five-stage classification to grade the severity of orbital infection
- Describe the investigations required and interpret CT orbital findings in orbital cellulitis
- Outline the medical and surgical management of orbital cellulitis and recognise when to escalate for surgical drainage
- Identify the warning signs of complications including compressive optic neuropathy and cavernous sinus thrombosis
INSTRUCTIONS
Orbital cellulitis is an ophthalmic emergency. Failure to distinguish it from preseptal cellulitis, or to initiate appropriate IV antibiotics promptly, can result in permanent vision loss, cavernous sinus thrombosis, intracranial spread, or death. This module provides the systematic framework for diagnosis, staging (Chandler's classification), and management. The key anatomical concept — the orbital septum as the dividing line — was introduced in OP2.1; this module builds on it with the full clinical depth required at final-year level. Cavernous sinus thrombosis as a complication is introduced here and covered in full in OP2.5.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch 16 (Orbital Diseases) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch 16 (The Orbit) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-year-old boy is brought to casualty by his parents. For three days he has had a cold with nasal congestion and right cheek pain. This morning his right eye is nearly swollen shut, and he cannot open it fully. His temperature is 38.9°C. When you examine him, his right eye is proptosed, and when you try to gently move the eye to the right he screams in pain. His visual acuity is 6/12 on the right. His left eye is completely normal. This child does not have a simple lid infection — the orbital septum has been breached, and the infection is inside the orbit. Every hour without IV antibiotics increases the risk to his vision and his life. What do you do in the next 30 minutes, and how does Chandler's classification tell you whether he needs surgery tonight?
WHY THIS MATTERS
Orbital cellulitis accounts for approximately 1–3% of ophthalmic emergencies and is most common in children, where it typically complicates sinusitis. In India, delayed presentation is common, and patients may arrive with advanced stages including subperiosteal or orbital abscess. The consequences of missed or inadequately treated orbital cellulitis are severe: vision loss from compressive optic neuropathy or central retinal artery occlusion, cavernous sinus thrombosis with bilateral ophthalmoplegia and meningism, intracranial abscess, and death. Competency OP2.4 requires you to describe the aetiology, clinical presentation, complications, and management — this is a ward-based diagnosis you will make as a house officer.
RECALL
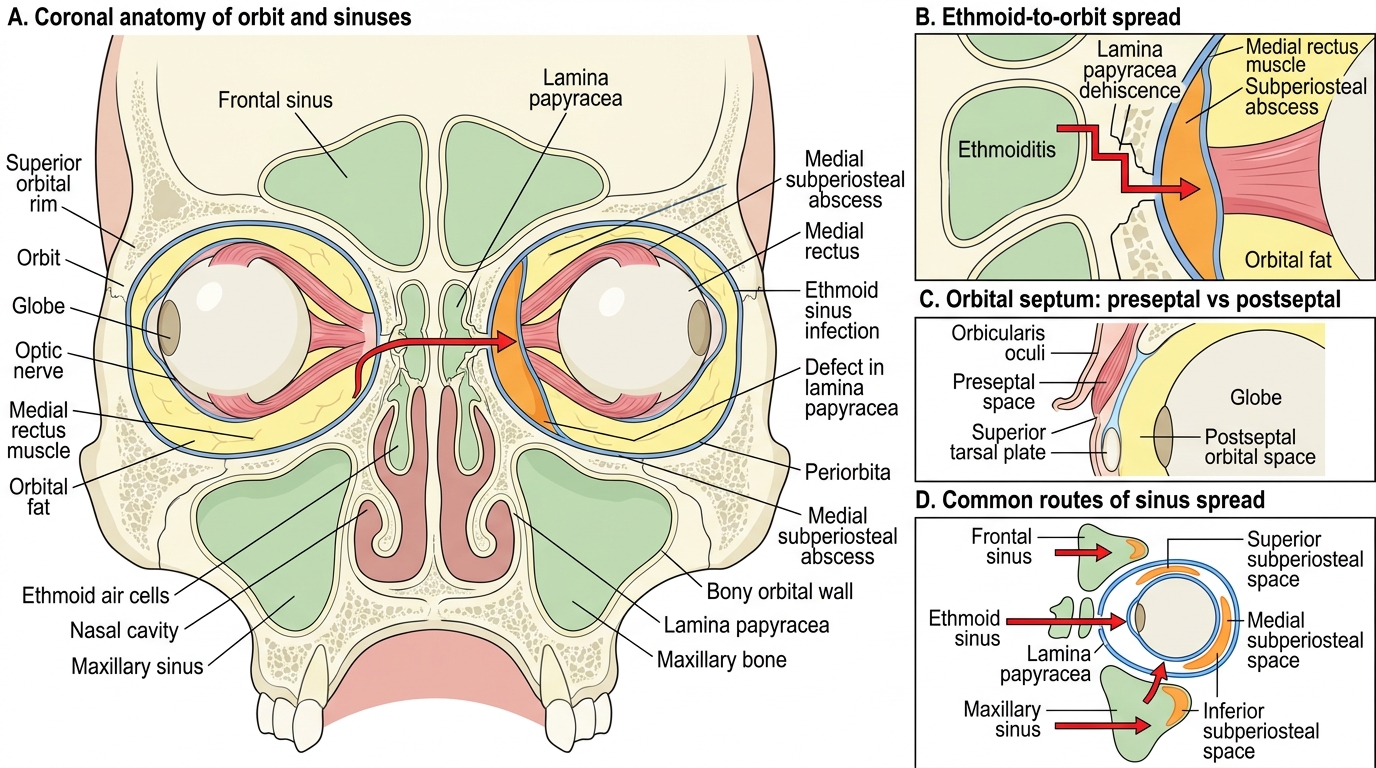
From OP2.1: the orbital septum is a fibrous sheet from the orbital rim periosteum that inserts into the tarsus; it divides the preseptal space (eyelid soft tissues) from the orbital space (postseptal). Preseptal cellulitis (anterior to septum) = no proptosis, no EOM restriction, normal vision. From Year-1 Anatomy: the paranasal sinuses — ethmoid, maxillary, frontal, sphenoid — are adjacent to the orbit. The ethmoid sinus lies directly medial to the orbit, separated only by the lamina papyracea ('paper plate'), an extremely thin bone. In children, the ethmoid sinuses are well-developed and highly vascular — ethmoid sinusitis is the commonest antecedent to orbital cellulitis. The orbit is also bounded superiorly by the frontal sinus and inferiorly by the maxillary sinus. The ophthalmic veins drain without valves into the cavernous sinus — a critical pathway for septic embolisation.
Clinical Presentation: The Swollen, Red, Proptosed Eye with Fever
Orbital cellulitis presents as a unilateral painful orbital syndrome with systemic features of infection. The clinical presentation follows from the anatomy: infection in the postseptal orbital space causes orbital oedema and inflammatory mass effect, pushing the globe forward (proptosis), inflaming and tethering the extraocular muscles (EOM restriction and pain), and potentially compressing the optic nerve (vision loss). The history typically reveals a recent upper respiratory tract infection, sinusitis, or facial trauma in the days preceding the orbital symptoms.
The critical distinction from preseptal cellulitis is the presence of postseptal involvement, evidenced by proptosis, painful or restricted eye movements, or visual disturbance. A clinician who misclassifies orbital cellulitis as preseptal and sends the patient home with oral antibiotics risks sight-threatening or life-threatening complications. The characteristic clinical features of orbital cellulitis that distinguish it from preseptal cellulitis are:
- Proptosis: the globe is pushed forward by orbital oedema and inflammatory mass; measured with Hertel exophthalmometry (or simply estimated by viewing from above the patient's head)
- Restricted and painful extraocular movements: the inflamed orbital fat and muscle sheaths limit and hurt — the patient screams on attempted lateral gaze, or restricts movement voluntarily; this is the single most reliable clinical sign separating orbital from preseptal disease
- Reduced visual acuity: orbital oedema and elevated intraorbital pressure can compromise blood supply to the optic nerve or retina; any VA reduction in a cellulitis patient means the orbit is involved
- Colour desaturation: an early sign of optic nerve involvement, detectable before VA drops significantly
- Chemosis: conjunctival oedema (gelatinous prolapse of conjunctiva) from raised intraorbital pressure
- Systemic signs: fever >38.5°C, raised WBC, elevated CRP/ESR; children may appear toxic
- History of sinusitis: the parent or patient reports recent nasal congestion, sinus pressure, or discharge
Orbital Septum and Sinus Routes of Orbital Infection
Anatomy of the Orbital Septum and Routes of Infection
The pathoanatomy of orbital cellulitis explains why sinusitis is the most common cause in children and young adults. Understanding the routes of spread from sinus to orbit allows you to predict which wall of the orbit will be affected and which anatomical stage of Chandler's classification the patient is likely in.
The lamina papyracea (paper-thin medial orbital wall) is the single most important anatomical structure in orbital cellulitis. It forms the lateral wall of the ethmoid sinuses and the medial wall of the orbit; it is so thin (0.25–0.5 mm) that it may have natural dehiscences even in health, and infection from the ethmoid cells can track through it into the subperiosteal space on the medial side of the orbit. This explains why the vast majority of subperiosteal abscesses in orbital cellulitis are located medially.
Other routes of infection: (1) Superior — from the frontal sinus, producing superior subperiosteal abscess (less common). (2) Inferior — from the maxillary sinus, producing inferior subperiosteal collection. (3) Haematogenous seeding — bacteraemia can seed the orbital fat directly, without an adjacent sinusitis; this route is relatively uncommon but important in immunocompromised patients. (4) Direct extension — from lid or face cellulitis (rare, as the septum provides an effective barrier). (5) Post-traumatic or post-surgical — orbital foreign body or surgical wound contamination.
The valveless ophthalmic veins are the anatomical basis for the spread to the cavernous sinus: the superior and inferior ophthalmic veins drain the orbit and connect posteriorly to the cavernous sinus without valves. Infected thrombi can propagate retrogradely into the cavernous sinus, producing septic cavernous sinus thrombosis — Chandler Stage V. This is covered in detail in OP2.5.
Microbiology: In children, the commonest organisms are Staphylococcus aureus (including community-acquired MRSA in some centres), Streptococcus pneumoniae, and Streptococcus pyogenes. Haemophilus influenzae was once a major pathogen in children under 9 but has been dramatically reduced by Hib vaccination. In immunocompromised patients (diabetics, haematological malignancy), Mucormycosis (Mucor/Rhizopus species) must be excluded — it presents with a characteristic black eschar on the nasal or palatal mucosa, rapid progression, and perineural/perivascular invasion.
Systematic Examination and Investigation of Orbital Cellulitis
Every patient with suspected orbital cellulitis must have a rapid, systematic examination that generates the key clinical information to stage the disease and guide immediate management. Examination should not be delayed by waiting for investigations — clinical staging is needed immediately.
Examination sequence: (1) General: fever, toxic appearance, meningism (neck stiffness, photophobia — indicates possible intracranial extension). (2) Visual acuity (both eyes — compare carefully; even a one-line drop is significant). (3) Colour vision (check with Ishihara plates or simply compare red saturation between eyes). (4) Pupil reactions, including RAPD (swinging flashlight test). (5) Proptosis assessment (Hertel exophthalmometry; if unavailable, compare profiles from above). (6) Extraocular movements in all nine positions of gaze — both restriction and pain on movement (the most reliable clinical sign of orbital involvement). (7) Lid examination — erythema, oedema, a pointing lid abscess, or skin necrosis (black eschar suggests Mucormycosis). (8) Conjunctival examination — chemosis, discharge. (9) Slit-lamp — anterior segment, corneal exposure. (10) Fundal examination (indirect ophthalmoscopy) — papilloedema or disc swelling may indicate raised intracranial pressure; dilated veins or central retinal vein occlusion (CRVO) suggest venous congestion in early CST. (11) ENT examination — nasal endoscopy or anterior rhinoscopy; tenderness over sinuses.
Investigations: Full blood count with differential (leucocytosis in bacterial infection), ESR, CRP, blood cultures (before antibiotics), nasal swab and culture, blood glucose (exclude diabetic ketoacidosis predisposing to Mucormycosis). CT orbits with contrast (axial and coronal cuts): mandatory in all suspected orbital cellulitis. CT shows the anatomical extent of infection, confirms postseptal involvement, identifies subperiosteal or orbital abscess (hypodense collection with rim enhancement), reveals sinus disease (opacification, air-fluid levels), and guides surgical planning. MRI with contrast is preferred when cavernous sinus or intracranial extension is suspected (superior resolution for soft tissue and vascular structures). Lumbar puncture if meningism is present.
SELF-CHECK
A 7-year-old boy presents with right periorbital swelling and fever. Examination reveals right proptosis (20 mm vs 16 mm left), right EOM restriction (cannot adduct fully) and pain on any attempted eye movement, VA right 6/12 (previously 6/6). CT orbits shows a hypodense collection with rim enhancement between the medial orbital wall and the periorbita on the right, from which the periorbita is lifted away from the bone. What Chandler stage is this and what is the next management step?
A. Chandler Stage I — prescribe oral antibiotics and review in 24 hours
B. Chandler Stage III (subperiosteal abscess) — admit for IV antibiotics and surgical drainage criteria assessment
C. Chandler Stage II — IV antibiotics only, no surgery needed
D. Chandler Stage V (cavernous sinus thrombosis) — IV antibiotics and anticoagulation
Reveal Answer
Answer: B. Chandler Stage III (subperiosteal abscess) — admit for IV antibiotics and surgical drainage criteria assessment
A hypodense collection with rim enhancement between the periorbita and the medial orbital wall is a subperiosteal abscess — Chandler Stage III. This requires immediate hospital admission, IV antibiotics (e.g., IV co-amoxiclav or ceftriaxone), and assessment for surgical drainage. Drainage is indicated if: the patient is ≥9 years, the abscess is large (>10 mm on CT), or there is no improvement after 48 hours of IV antibiotics. Vision monitoring (VA and colour vision) twice daily is mandatory. Stage II (orbital cellulitis without abscess) shows postseptal fat stranding without a discrete collection. Stage V involves bilateral signs, meningism, and involvement crossing the midline.