Page 13 of 30
OP2.4 | Orbital Cellulitis — SDL Guide (Part 2)
Chandler's Classification and Diagnosis
The classification is built on a key anatomical boundary — the orbital septum — and tracks the posterior spread of infection from the pre-septal lid tissues through the sub-periosteal plane, into the orbital fat, and ultimately into the cavernous sinus. Stage I and II lesions are medical emergencies; Stage III to V lesions are surgical emergencies. The practical value of Chandler's staging is that it converts clinical and CT findings into an immediate treatment decision: oral antibiotics for Stage I, intravenous antibiotics for Stage II, surgical drainage for Stage III-V. This decision framework is directly examinable and clinically consequential.
Provided image
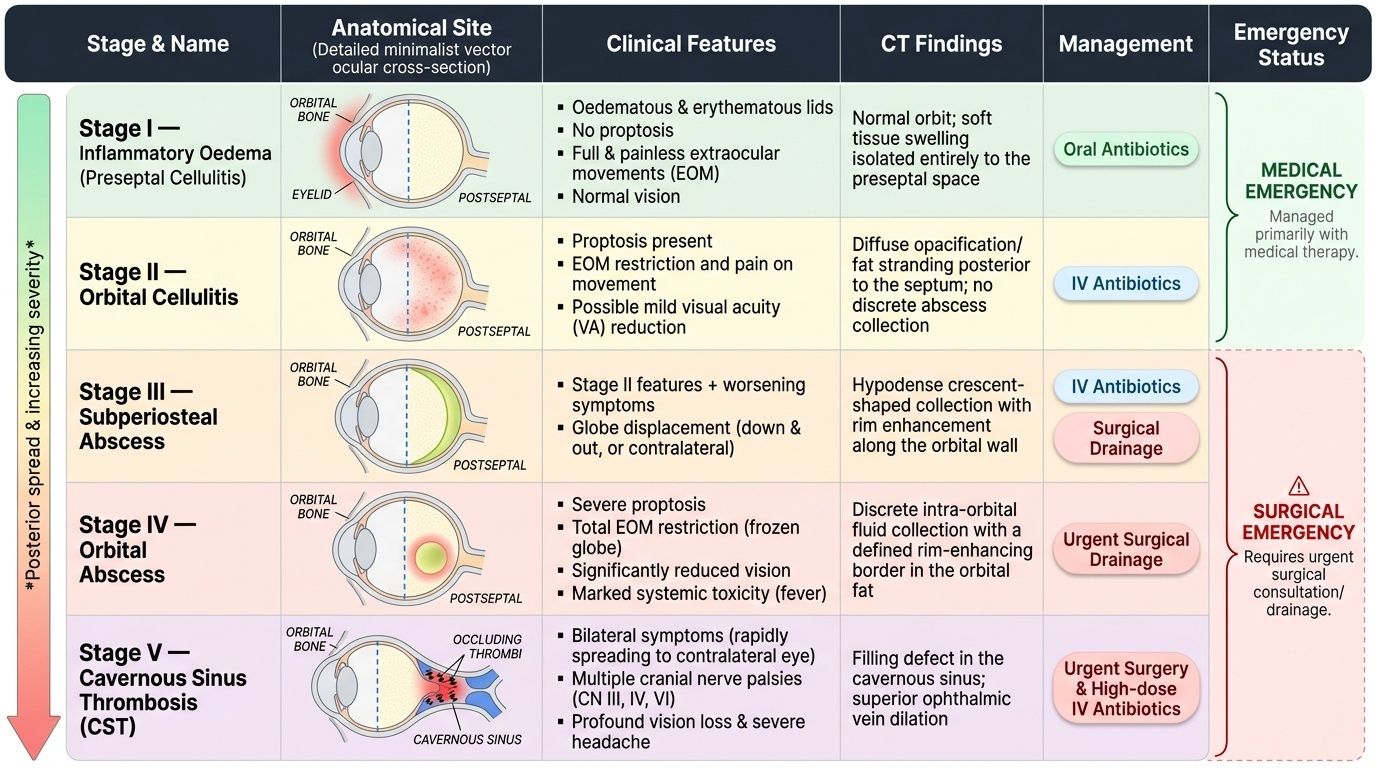
Chandler's classification (1970) remains the standard staging system for orbital infections and directly guides management decisions. Understanding the five stages and their anatomical correlates allows the clinician to select appropriate treatment immediately on seeing the CT and clinical findings.
The five stages are:
- Stage I — Inflammatory oedema (preseptal cellulitis): infection is ANTERIOR to the orbital septum; lids are oedematous and erythematous; NO proptosis; EOM are full and painless; vision is normal. This is NOT orbital cellulitis — it is managed as preseptal cellulitis with oral antibiotics.
- Stage II — Orbital cellulitis: infection has crossed the orbital septum into the postseptal orbital fat; proptosis is present; EOM restriction and pain on movement; possible mild VA reduction; CT shows diffuse opacification/fat stranding posterior to the septum without a discrete abscess. IV antibiotics without surgery.
- Stage III — Subperiosteal abscess: pus collects between the periorbita (periosteum lining the inner orbital wall) and the orbital bone; typically located medially (from ethmoid sinusitis); CT shows a hypodense crescent-shaped collection with rim enhancement along the orbital wall; globe displaced away from the abscess (contralateral globe shift); all Stage II features plus worsening. May require surgical drainage.
- Stage IV — Orbital abscess: pus is now within the orbital fat itself (intra-conal or extraconal); severe proptosis; total EOM restriction; significantly reduced vision; marked systemic toxicity; CT shows a discrete intra-orbital collection. Requires surgical drainage urgently.
- Stage V — Cavernous sinus thrombosis (CST): infection has spread via the ophthalmic veins to the cavernous sinus; BILATERAL proptosis, ophthalmoplegia (CN III, IV, VI palsy), high fever, meningism, papilloedema; this is covered in detail in OP2.5. Life-threatening emergency.
Differential diagnosis of orbital cellulitis: TED (bilateral, painless EOM, known thyroid disease — OP2.3); orbital tumour (slower progression, no fever — OP2.7); orbital pseudotumour / idiopathic orbital inflammation (very painful, steroid-responsive, tendon involvement on CT); carotid-cavernous fistula (pulsatile proptosis, bruit); rhabdomyosarcoma in children (rapidly progressive painless proptosis without systemic infection).
SELF-CHECK
A 12-year-old girl develops bilateral painful proptosis, bilateral complete ophthalmoplegia (she cannot move either eye in any direction), high fever, and neck stiffness over 24 hours after initially having unilateral right orbital cellulitis. What complication has occurred and what is the management?
A. Stage IV orbital abscess — urgent surgical drainage of both orbits
B. Stage V — cavernous sinus thrombosis; IV antibiotics and consider anticoagulation; urgent neurology and neurosurgery consultation
C. Bilateral orbital cellulitis from haematogenous spread — increase IV antibiotic dose
D. Orbital pseudotumour (idiopathic orbital inflammation) — high-dose IV methylprednisolone
Reveal Answer
Answer: B. Stage V — cavernous sinus thrombosis; IV antibiotics and consider anticoagulation; urgent neurology and neurosurgery consultation
Bilateral ophthalmoplegia, bilateral proptosis, high fever, and neck stiffness in a patient with prior unilateral orbital cellulitis is the classic presentation of septic cavernous sinus thrombosis (Chandler Stage V). The infection has spread via the valveless ophthalmic veins to the cavernous sinus, which houses CN III, IV, V1, V2, and VI — bilateral cranial nerve palsies produce the bilateral ophthalmoplegia. Neck stiffness indicates meningeal irritation. Management: urgent IV antibiotics (ceftriaxone + metronidazole); anticoagulation is controversial but may be used to prevent clot propagation; neurosurgery and neurology consultation for possible intracranial abscess; intensive care monitoring. Mortality remains high (~30%) even with treatment.
Management: Medical and Surgical Treatment of Orbital Cellulitis
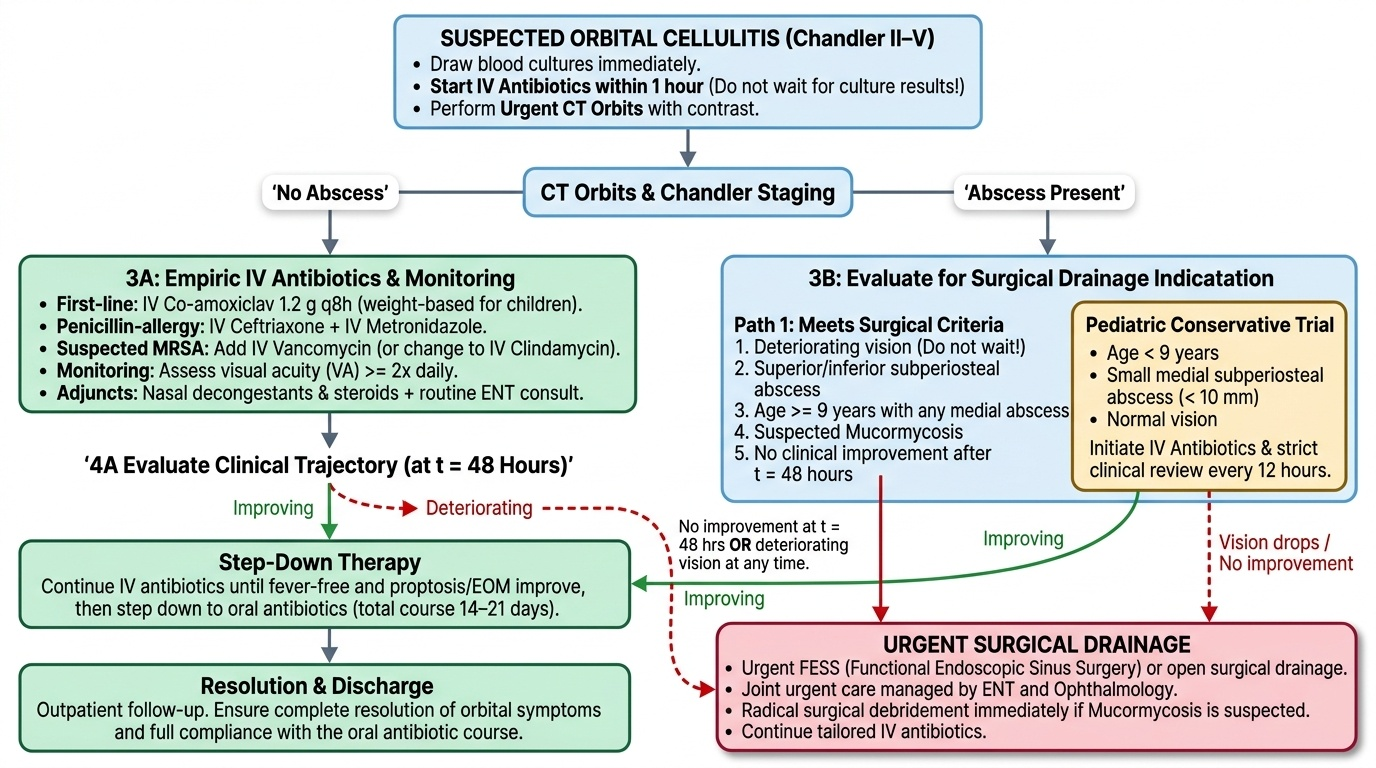
The management of orbital cellulitis is guided by Chandler's stage and the patient's clinical trajectory. The overarching principle is to begin IV antibiotics as soon as blood cultures are drawn (never wait for culture results), perform CT orbits urgently to stage the disease, monitor visual function at least twice daily, and have a low threshold for surgical drainage.
Provided image
Medical management (all stages II–V): Intravenous antibiotics should be started within 1 hour of diagnosis. First-line regimen: IV co-amoxiclav (amoxicillin-clavulanate) 1.2 g every 8 hours (children: weight-based dosing) covers staphylococci, streptococci, and oral anaerobes from sinusitis. If MRSA is suspected (community-acquired MRSA in certain regions, or failure to respond), add IV vancomycin or change to IV clindamycin. In penicillin-allergy: IV ceftriaxone plus IV metronidazole. Duration: IV antibiotics until fever resolved and proptosis/EOM improving, then step down to oral antibiotics; total course typically 14–21 days.
Adjuncts: nasal decongestants and nasal steroids to promote sinus drainage; sinus drainage procedure (functional endoscopic sinus surgery, FESS) as part of surgical management; ENT involvement is routine.
Surgical drainage: Indications: (1) subperiosteal or orbital abscess confirmed on CT; (2) no improvement after 48 hours of appropriate IV antibiotics; (3) vision deteriorating at any time — do not wait; (4) age ≥9 years with any medial subperiosteal abscess (larger abscesses in older children are less likely to resolve with antibiotics alone); (5) superior or inferior subperiosteal abscess (these are less accessible via endoscopic sinus surgery and drain poorly); (6) suspected Mucormycosis (requires urgent radical surgical debridement). Children under 9 with a small (<10 mm) medial subperiosteal abscess without vision compromise can initially be managed with IV antibiotics alone, but must be reviewed every 12 hours and taken to theatre immediately if VA drops.
Mucormycosis (invasive fungal sinusitis/orbital cellulitis): A life-threatening emergency in immunocompromised patients (uncontrolled diabetic, haematological malignancy, post-COVID). Characteristic features: black eschar on nasal or palatal mucosa (tissue necrosis from vascular invasion), rapid progression (hours to days), perineural spread along cranial nerves, and early periorbital skin changes. Management: urgent surgical debridement (often extensive, including orbital exenteration in advanced cases) combined with IV liposomal amphotericin B (3–5 mg/kg/day); posaconazole or isavuconazole as alternatives. Blood glucose control and reversal of immunosuppression are essential.
Monitoring: Visual acuity (Snellen) and colour vision (Ishihara) checked every 12 hours in all admitted orbital cellulitis patients. A drop of even one line in VA, or new RAPD, or colour desaturation — regardless of Chandler stage — is an indication for immediate CT and surgical review.
Complications: Optic Nerve Compromise and Cavernous Sinus Spread
Two complications of orbital cellulitis are immediately sight- and life-threatening and must be monitored for from the moment of admission. Both require recognition within hours, not days.
Optic nerve compromise: The optic nerve can be compressed by an expanding subperiosteal or orbital abscess, or by the diffuse raised intraorbital pressure of orbital cellulitis without a discrete collection. Clinically: reduced visual acuity (any reduction from baseline is significant — even 6/9 from 6/6 must be investigated), impaired colour vision (Ishihara testing or asking if red objects look 'as red' in both eyes), positive RAPD on swinging flashlight test, and visual field defect. Optic disc pallor is a late sign. Action: any new visual change → emergency CT, surgical review, and if optic nerve compression confirmed → immediate surgical drainage or decompression. Central retinal artery occlusion (CRAO) is a rarer but devastating complication in which the artery is thrombosed by septic thrombus.
Cavernous sinus thrombosis (CST): Covered in OP2.5 in full detail. Warning signs of CST onset in a patient with orbital cellulitis: involvement of the CONTRALATERAL eye (bilateral proptosis, bilateral ophthalmoplegia — the pathognomonic sign that infection has crossed the midline via the cavernous sinus), high spiking fever, meningism (neck stiffness, photophobia, Kernig's sign), and rapid clinical deterioration. CT/MRI shows filling defect or non-enhancement of the cavernous sinus. Any bilateral orbital signs in a patient with unilateral orbital cellulitis must be treated as CST until proven otherwise.
Intracranial extension: Orbital cellulitis can spread directly to the brain, producing epidural or subdural abscess, frontal lobe abscess, or meningitis. Clinical signs: worsening headache, altered consciousness, focal neurological deficits, or seizures. Urgent CT brain with contrast is indicated.
SELF-CHECK
During monitoring of a 9-year-old with Chandler Stage III orbital cellulitis on IV antibiotics for 24 hours, you note the right visual acuity has dropped from 6/6 on admission to 6/18, and there is a new right RAPD. The proptosis has increased from 22 mm to 25 mm. What is the correct immediate action?
A. Wait another 24 hours on IV antibiotics before reassessing
B. Repeat CT orbits immediately and arrange emergency surgical orbital drainage
C. Add topical steroid eye drops and review in the morning
D. Switch to a higher-dose IV antibiotic and continue monitoring
Reveal Answer
Answer: B. Repeat CT orbits immediately and arrange emergency surgical orbital drainage
Deteriorating visual acuity (6/6 → 6/18) and a new RAPD indicate developing optic nerve compromise. This is a surgical emergency — do NOT wait. Immediate CT orbits is performed to delineate the abscess, and emergency surgical drainage is arranged without delay. Vision lost from optic nerve compression in orbital cellulitis may not recover if the pressure is not relieved promptly. Increasing IV antibiotic dose or topical drops cannot reverse mechanical compression of the optic nerve.
CLINICAL PEARL
The cardinal rule: monitor visual acuity and colour vision at least every 12 hours in every patient admitted with orbital cellulitis. Vision change is the red flag that demands immediate action — it overrides Chandler staging, antibiotic response, and any other consideration. A patient who is 'improving on antibiotics' but whose VA has dropped from 6/6 to 6/12 in 24 hours must go to CT and possibly to theatre tonight. A second pearl: in the immunocompromised patient with orbital cellulitis — diabetic, haematology patient, post-COVID — always examine the nasal mucosa and palate for a black eschar. Mucormycosis is rapidly fatal without aggressive surgical debridement and antifungal therapy, and it is easily missed as 'just another orbital cellulitis' in the first 24 hours.
Self-Assessment: Orbital Cellulitis
Self-assessment for orbital cellulitis requires integrating four domains: the anatomy of orbital infection spread and the significance of the orbital septum, the clinical and CT features that distinguish preseptal from postseptal disease, Chandler's five-stage classification and its direct mapping to treatment decisions, and the management protocol including antibiotic choice, surgical indications, and the two life-threatening complications that mandate emergency escalation. The most dangerous clinical error in this topic is failure to recognise the transition from Stage I to Stage II — a child with a swollen red lid who also has proptosis and restricted painful eye movements has orbital cellulitis, not preseptal cellulitis, and requires hospital admission, IV antibiotics, and urgent CT. Similarly, any deterioration in visual acuity or colour vision during treatment signals optic nerve compression and demands same-day surgical decompression.
- A 12-year-old boy presents with a swollen, red left upper lid, proptosis of 4 mm, and pain on horizontal gaze. He is febrile at 38.6°C. What is the diagnosis, what investigation is most important, and what is the first-line treatment?
- A patient with orbital cellulitis is admitted on IV co-amoxiclav. After 48 hours, despite clinical improvement in lid swelling, he develops worsening of colour vision in the left eye. What complication has occurred and what is the immediate management?
- Name the five stages of Chandler's classification and state for each whether management is primarily medical or surgical.
- Which sinus is most commonly the source of orbital cellulitis in children, and in which direction does the infection typically spread into the orbit?
- Name three life-threatening complications of orbital cellulitis and for each explain the anatomical route of spread.
Expected answers: (1) Orbital cellulitis (postseptal, Chandler Stage II); CT orbit with contrast; IV co-amoxiclav or piperacillin-tazobactam, ENT review for sinus drainage. (2) Optic nerve compression (Stage III-IV progression); emergency surgical decompression of the orbit. (3) Stage I preseptal (medical), Stage II orbital (medical), Stage III subperiosteal abscess (often surgical), Stage IV orbital abscess (surgical), Stage V cavernous sinus thrombosis (IV heparin + antibiotics + ICU). (4) Ethmoid sinus; medial orbital wall (lamina papyracea). (5) Meningitis (orbital veins → cavernous sinus → dural sinuses), cavernous sinus thrombosis (orbital/ophthalmic veins → cavernous sinus, via valveless retrograde propagation of infected thrombus), brain abscess (direct spread through orbital roof or via venous emissaries).