Page 11 of 27
OP3.4 | Allergic Conjunctivitis and Vernal Catarrh — SDL Guide
Learning Objectives
- Enumerate the causes of allergic conjunctivitis and classify them by immunological mechanism
- Describe the aetiology, pathophysiology, and ocular features of vernal keratoconjunctivitis (VKC)
- Identify the clinical signs of VKC — giant papillae, Trantas dots, shield ulcer — and their significance
- Outline the management of allergic conjunctivitis and VKC including topical mast-cell stabilisers, antihistamines, and steroids
INSTRUCTIONS
Allergic conjunctivitis is the most common chronic eye condition in the world, affecting up to 40% of the population in some surveys. It ranges from the mild, seasonal discomfort of hay-fever eye to the sight-threatening giant-papillary and corneal complications of vernal keratoconjunctivitis (VKC). VKC is particularly important in India and other hot-climate countries where it is prevalent, predominantly affects young males, and can cause irreversible visual loss from corneal scarring if poorly managed. The NMC OP3.4 competency requires you to enumerate causes, describe the pathophysiology and features of VKC, and outline its management.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 6: Diseases of Conjunctiva (Allergic section) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 8: Diseases of the Conjunctiva (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 12-year-old boy is brought to your clinic every summer with intensely itchy eyes, a thick stringy discharge, and swollen eyelids. He rubs his eyes constantly. His mother says it starts every March and improves after the monsoon. She also reports that his teacher sent a note last week because the boy was not able to see clearly on the blackboard. On examining his eyes, you find a normal visual acuity today, a ropy whitish discharge in the fornices, and — on everting the upper eyelid — a dramatic cobblestone surface of large, flat-topped elevations covering the entire palpebral conjunctiva. What has caused this dramatic picture? What are the complications you need to look for? And why does this boy need more than a simple antihistamine?
WHY THIS MATTERS
Allergic eye disease affects approximately 20–40% of people with atopy and is the most common cause of chronic bilateral conjunctival inflammation in school-age children in India and other tropical countries. Vernal keratoconjunctivitis (VKC) — the most severe allergic conjunctivitis — is particularly prevalent in the Indian subcontinent, Middle East, and sub-Saharan Africa, where hot dry climates, high pollen loads, and outdoor activity in young males create a perfect epidemiological storm. Unlike simple seasonal hay-fever conjunctivitis, VKC can cause corneal complications (shield ulcer, scarring) that permanently damage vision. The OP3.4 competency requires you to know both the common allergic forms and the potentially sight-threatening VKC in full clinical detail.
RECALL
From your immunology module, recall that Type I (immediate) hypersensitivity is IgE-mediated: on first exposure to an allergen, B-cells produce allergen-specific IgE antibodies that bind to high-affinity FcεRI receptors on mast cells and basophils. On re-exposure, allergen cross-links the surface-bound IgE, triggering mast-cell degranulation and release of preformed mediators (histamine, tryptase) and newly synthesised lipid mediators (prostaglandins, leukotrienes). Histamine binds H1 receptors on conjunctival blood vessels (vasodilation → redness) and on sensory nerve endings (itch). Type IV (delayed) hypersensitivity is T-cell mediated: sensitised T helper cells recruit macrophages and eosinophils over 24–72 hours. From your earlier study of acute conjunctivitis, recall that papillary reaction indicates bacterial or allergic stimulation — and the 'giant papillae' of VKC are the allergic extreme of this spectrum.
The Itchy Eye — Allergic Conjunctivitis as a Spectrum
Allergic conjunctivitis encompasses a spectrum of conditions unified by immune-mediated conjunctival inflammation in response to allergen exposure. Across all forms, itch is the dominant symptom — the single most important feature that distinguishes allergic from infective conjunctivitis. Patients describe intense, irresistible itching that worsens with rubbing; rubbing releases further histamine from mast cells, perpetuating the cycle. Tearing, redness, and photophobia may accompany the itch, but itch without infective discharge in a bilateral eye presentation should always raise allergic disease as the primary diagnosis.
The spectrum of allergic conjunctivitis includes four forms:
1. Seasonal allergic conjunctivitis (SAC): Most common form; triggered by seasonal allergens (pollen — tree pollen in spring, grass pollen in summer). Bilateral, acute onset, resolves with the season. Associated with hay fever (allergic rhinitis) and atopy.
2. Perennial allergic conjunctivitis (PAC): Similar to SAC but triggered by perennial allergens (house dust mite, animal dander, mould). Milder but year-round. Both SAC and PAC are IgE-mediated Type I reactions and are not sight-threatening.
3. Vernal keratoconjunctivitis (VKC): The most severe form; affects young males (5–25 years) in hot climates; seasonal exacerbations in spring and summer. Mixed Type I and Type IV hypersensitivity. Can cause corneal complications (shield ulcer, corneal scarring, amblyopia). This is the focus of OP3.4.
4. Atopic keratoconjunctivitis (AKC): Associated with atopic dermatitis (eczema); affects adults 20–50 years; year-round, more severe than SAC/PAC. Can cause anterior subcapsular cataract, keratoconus, and corneal scarring. Less common in India than VKC.
5. Giant papillary conjunctivitis (GPC): Caused by mechanical trauma from contact lenses, exposed suture, or an ocular prosthesis rather than allergen exposure. Giant papillae on the upper palpebral conjunctiva; resolves on removing the offending contact lens.
Immunology of Allergic Conjunctivitis: Mast Cells, IgE, and Eosinophils
Understanding the immunological mechanisms of allergic conjunctivitis explains why different forms respond to different treatments and why VKC is more severe and more difficult to control than simple SAC. This mechanism-first approach is not academic: every drug used in allergic eye disease — antihistamines, mast-cell stabilisers, topical steroids, cyclosporine — has a precise mechanistic target, and knowing where each drug acts in the pathway explains both why the drug works and why it may fail in isolation. Simple seasonal allergic conjunctivitis involves only the Type I (IgE/mast-cell) limb, and antihistamines alone provide satisfactory control. VKC involves both Type I and Type IV (T-cell/eosinophil) limbs, which is why antihistamines are necessary but insufficient — the eosinophilic tissue damage continues even after mast-cell mediators are blocked, and a second agent targeting T-cell activation (topical cyclosporine) or suppressing eosinophilic inflammation broadly (topical steroids) is needed.
The Type I (IgE-mediated) pathway — common to all forms:
The conjunctival stroma contains abundant mast cells — up to 5,000 per mm² — which are sensitised to specific allergens via surface IgE. On re-exposure, allergen cross-links the IgE on mast cells within seconds, triggering degranulation. The released mediators produce the acute symptoms:
- Histamine → itching (H1 nerve receptors), vasodilation (redness), increased vascular permeability (chemosis and tearing).
- Prostaglandins → sustained vasodilation and pain sensitisation.
- Leukotrienes (LTC4, LTD4) → sustained chemotaxis and more prolonged vascular changes.
- Platelet-activating factor (PAF) → eosinophil recruitment.
In simple SAC/PAC, this is the complete mechanism — symptoms are driven by mast-cell mediators and respond well to H1-antihistamines and mast-cell stabilisers.
The Type IV (T-cell mediated) component — unique to VKC and AKC:
In VKC, repeated allergen exposure triggers a second delayed-hypersensitivity limb. CD4+ Th2 lymphocytes are recruited and release IL-4, IL-5, and IL-13 — cytokines that drive B-cell class-switching to IgE (amplifying the Type I response) and eosinophil recruitment and survival. The infiltrating eosinophils are the primary mediators of chronic tissue damage in VKC:
- Eosinophil major basic protein (MBP) is directly toxic to the corneal epithelium — deposited by degranulating eosinophils directly on the corneal surface by the giant papillae, it causes the corneal epithelial loss that forms the shield ulcer.
- Eosinophilic mediators also drive fibroblast activation and collagen deposition, contributing to conjunctival scarring.
- Histological hallmark of VKC: eosinophils in the conjunctival stroma (seen on scraping cytology) — their presence distinguishes VKC from purely infective conjunctivitis.
This dual mechanism — Type I and Type IV — is why VKC does NOT respond adequately to antihistamines alone. Mast-cell stabilisers and immunomodulators (cyclosporine) are needed to address both pathways.
SELF-CHECK
A 14-year-old boy with chronic bilateral itchy eyes and giant papillae on his upper palpebral conjunctiva has conjunctival scrapings performed. The finding most characteristic of vernal keratoconjunctivitis is:
A. Multinucleated giant cells on Giemsa stain
B. Eosinophils on Giemsa stain
C. Gram-positive diplococci on Gram stain
D. Neutrophils with intracellular inclusions
Reveal Answer
Answer: B. Eosinophils on Giemsa stain
Eosinophils are the hallmark cytological finding of vernal keratoconjunctivitis on conjunctival scraping (Giemsa stain). They reflect the Type IV hypersensitivity (Th2-driven eosinophil recruitment) component of VKC and are responsible for corneal epithelial damage through the toxic eosinophil major basic protein (MBP). Multinucleated giant cells suggest viral infection. Gram-positive diplococci indicate bacterial infection. Intracellular inclusions are seen in Chlamydia (trachoma/inclusion conjunctivitis) or viral infection.
Examining the Allergic Eye and Identifying the Form
Clinical examination of the allergic eye follows the same sequence as acute conjunctivitis, with particular attention to the palpebral conjunctiva (for papillae size and distribution) and the limbus and cornea (for Trantas dots and shield ulcer). The examination technique for VKC requires careful upper lid eversion and often double eversion to expose the upper fornix. The reason upper lid eversion is so central to VKC examination — and not merely optional — is that the giant papillae of the palpebral form are confined to the upper tarsal conjunctiva and are invisible without eversion. A clinician who examines only the visible bulbar conjunctiva in a patient with VKC will see redness and mucoid discharge but will completely miss the diagnostic cobblestone papillae that confirm the diagnosis and determine the treatment. Similarly, Trantas dots at the upper limbus in the limbal form require deliberate examination of the corneoscleral junction under good illumination, not a cursory glance at the front of the eye.
Cardinal clinical signs of VKC:
- Ropy/stringy mucous discharge: A thick, white, mucoid discharge — ropy in character, forming long threads ('mucus strings') — is characteristic of VKC. It is produced by goblet cells responding to IL-4 signalling and is quite different from the thin watery discharge of viral conjunctivitis or the frankly purulent discharge of bacterial disease.
- Giant papillae (cobblestone papillae): On eversion of the upper eyelid in the palpebral form of VKC, the upper tarsal conjunctiva shows papillae exceeding 1 mm in diameter — the 'cobblestone' or 'cauliflower' appearance. Each papilla has a flat top, a central vascular core, and surrounding eosinophilic infiltration. The papillae mechanically rub against the cornea with each blink, depositing eosinophil major basic protein on the corneal epithelium. Normal papillae in bacterial conjunctivitis are small (0.2–0.5 mm); giant papillae >1 mm are pathognomonic of VKC or GPC.
- Trantas dots: In the limbal form of VKC, white chalky deposits appear at the upper corneal limbus — these are Trantas dots, collections of degenerated eosinophils and epithelial cells. They are pathognomonic of VKC limbal form and disappear with treatment. Limbal VKC is more common in African children; palpebral VKC is more common in Indian and Middle Eastern patients.
- Shield ulcer: A superficial horizontal oval grey epithelial defect in the upper-central cornea, caused by mechanical trauma from giant papillae depositing eosinophil MBP on the corneal surface. Critically: the shield ulcer is superficial (epithelial, not stromal) and is NOT infectious — it does NOT have a bacterial aetiology. Prescribing intensive topical antibiotics alone will not heal it. It stains with fluorescein and can be seen clearly under cobalt-blue light.
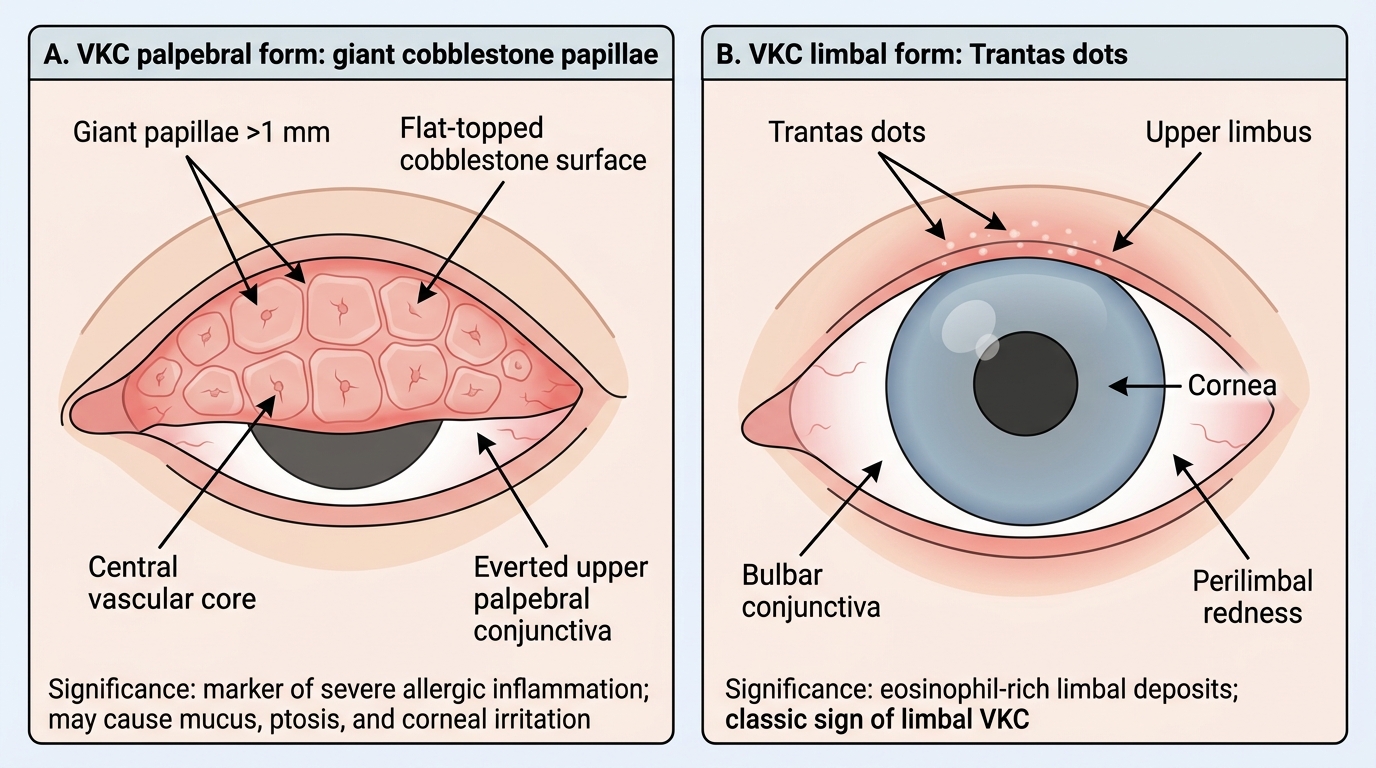
Clinical Signs of Vernal Keratoconjunctivitis