Page 12 of 27
OP3.4 | Allergic Conjunctivitis and Vernal Catarrh — SDL Guide (Part 2)
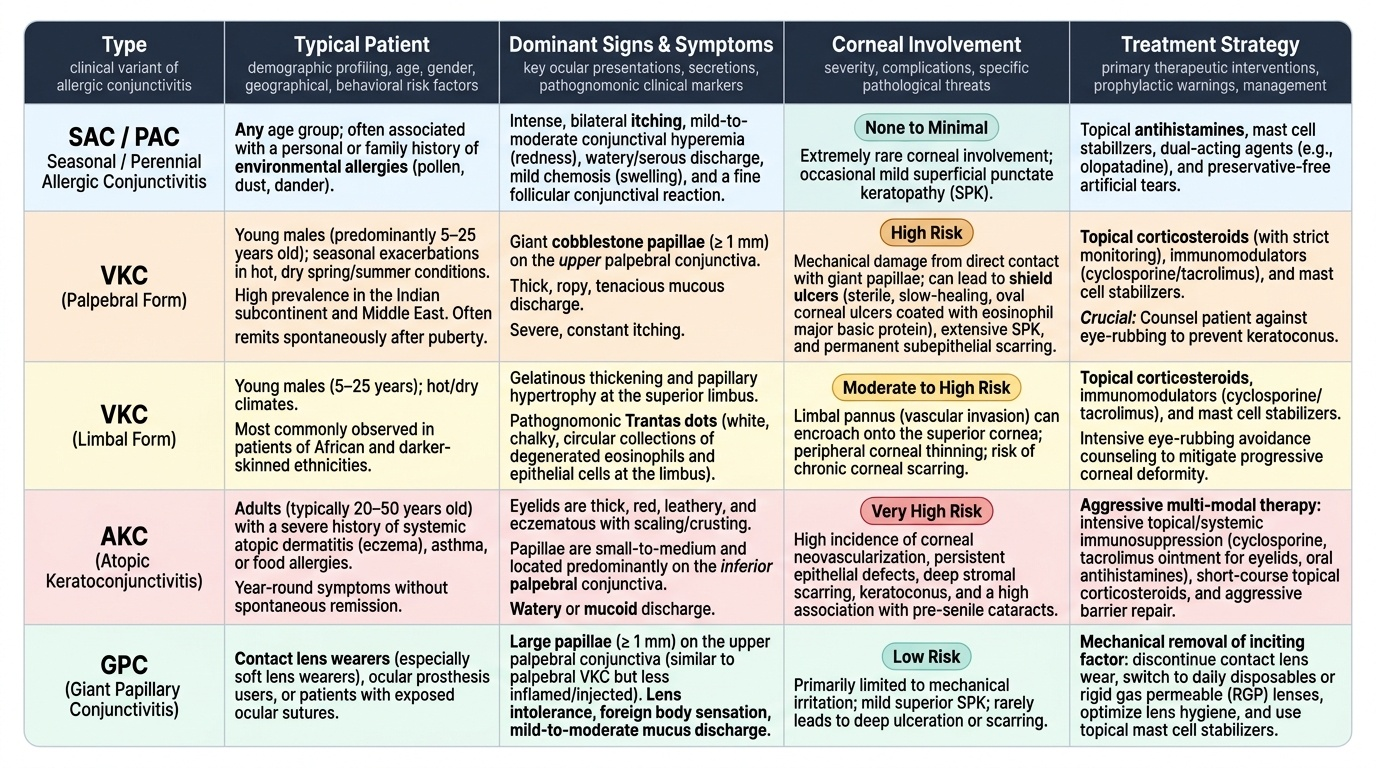
Vernal Keratoconjunctivitis: Forms, Features, and Complications
Vernal keratoconjunctivitis is the dominant form of allergic conjunctivitis in the Indian subcontinent and the most clinically important to understand fully. It predominantly affects males between the ages of 5 and 25 years, with seasonal exacerbations in spring and summer (hot, dry conditions with high allergen loads). It frequently remits spontaneously at or after puberty — though not always. The main clinical forms and their distinguishing features are: The prognosis of VKC depends critically on the form and on whether corneal complications develop: uncomplicated palpebral or limbal VKC that remits at puberty causes no lasting visual impairment; VKC with shield ulcers that are mismanaged (treated as bacterial keratitis with antibiotics alone, without addressing the underlying eosinophilic inflammation) can cause permanent corneal scarring and irreversible visual loss. The association of VKC with keratoconus — mediated by chronic mechanical eye-rubbing from itch — means that a VKC patient who is not counselled against rubbing may develop a progressive corneal deformity that outlasts the VKC itself and requires specialist contact lens fitting or corneal surgery.
Provided image
VKC palpebral form:
- Giant cobblestone papillae (>1 mm) on the UPPER palpebral conjunctiva.
- Ropy mucous discharge, intense itch.
- Corneal complications from direct papillary contact: shield ulcer, superficial punctate keratopathy, subepithelial scarring.
- More common in Indian and Middle Eastern patients.
VKC limbal form:
- Gelatinous thickening and papillary hypertrophy at the superior limbus.
- Trantas dots — pathognomonic white chalky collections of eosinophils at the limbus.
- More common in African patients.
- Limbal pannus can encroach on the cornea.
Mixed form: Both palpebral and limbal features coexist.
VKC complications:
1. Shield ulcer: Superficial corneal ulcer from eosinophil MBP deposition; heals slowly (weeks to months) with appropriate treatment; can leave a corneal scar if mismanaged (treated as infective) or if the patient continues to rub.
2. Pseudomembrane formation: Fibrinous exudate on the tarsal conjunctiva during severe episodes.
3. Corneal vascularisation and scarring: From chronic epithelial insult.
4. Keratoconus: Association between VKC and keratoconus is well established — chronic eye rubbing (from itch) mechanically disrupts the corneal stromal collagen, thinning the cornea and producing the cone shape of keratoconus.
5. Amblyopia: In young children with shield ulcers causing prolonged visual deprivation from corneal opacity.
Distinction from AKC and GPC:
- AKC (Atopic Keratoconjunctivitis): occurs in adults (20–50 years) with severe atopic dermatitis; lower lid folds (Dennie-Morgan lines) are characteristic; can cause anterior subcapsular cataract and keratoconus; does NOT remit at puberty.
- GPC (Giant Papillary Conjunctivitis): giant papillae on the upper palpebral conjunctiva that develop from contact-lens-induced mechanical trauma rather than allergen exposure; resolves on ceasing contact lens wear.
SELF-CHECK
A 10-year-old boy with VKC has developed a grey oval lesion in the upper-central cornea that stains with fluorescein. It is not infiltrated, the anterior chamber is quiet, and there is no discharge. The most appropriate management is:
A. Intensive topical fluoroquinolone antibiotics for bacterial keratitis
B. Topical corticosteroids, lubricants, and possibly a bandage contact lens to promote re-epithelialisation
C. Emergency corneal scraping for culture and systemic antifungals
D. Topical aciclovir for herpes simplex keratitis
Reveal Answer
Answer: B. Topical corticosteroids, lubricants, and possibly a bandage contact lens to promote re-epithelialisation
A superficial grey oval corneal ulcer in the upper-central cornea in a child with VKC and giant papillae is a classic shield ulcer — caused by eosinophil major basic protein deposited by the giant papillae on the corneal epithelium. It is NOT infectious. The correct management is topical corticosteroids (to reduce the underlying allergic inflammation), lubricants (to promote re-epithelialisation), and sometimes a bandage soft contact lens. Antibiotics are sometimes added to prevent secondary infection but are not the primary treatment. Treating a shield ulcer with antifungals or antivirals is inappropriate.
CLINICAL PEARL
The rubbing reflex in VKC is both a symptom and a cause of progression. Itch drives rubbing; rubbing releases more histamine from mast cells (amplifying the allergic reaction) and mechanically traumatises the cornea (promoting shield ulcer and keratoconus). The single most important counselling point for VKC patients and their parents is: do NOT rub the eyes, regardless of the itch. Cold compresses give temporary itch relief without the histamine-release cycle. This advice is as important as any medication.
Management of Allergic Conjunctivitis and VKC
Management of allergic conjunctivitis is stepped according to severity. Simple SAC/PAC responds to allergen avoidance and topical antihistamines. VKC requires a more aggressive and sustained approach targeting both Type I and Type IV pathways.
Step 1 — Allergen avoidance and environmental control:
For SAC/PAC: avoid exposure to identified allergens (pollen, dust mite), use air conditioning, change clothes after outdoor exposure, use wraparound glasses outdoors.
For VKC: avoidance of known exacerbants (sunlight, wind, dust) reduces severity; sun protection.
Step 2 — Topical mast-cell stabilisers:
Sodium cromoglicate (cromolyn) 2% eye drops — inhibit mast-cell degranulation; used prophylactically before allergen season begins; 4× daily. Also available as lodoxamide (10× more potent than cromoglicate). They have no acute relief effect — they prevent degranulation rather than reversing symptoms already present. Begin 2–4 weeks before the season.
Step 3 — Topical antihistamines ± mast-cell stabilisers:
Olopatadine 0.1% is the prototypical dual-action antihistamine (H1 blockade) AND mast-cell stabiliser in a single drop; used 1–2× daily. Azelastine, ketotifen are alternatives. These provide both acute relief (histamine blockade) and ongoing prophylaxis (mast-cell stabilisation).
Step 4 — Cold compresses:
Vasoconstriction from cold provides symptomatic itch relief and reduces conjunctival hyperaemia without pharmacological risk. Safe for all ages; can be used as often as needed.
Step 5 — Topical corticosteroids (VKC — short course):
For acute severe VKC flares (especially with shield ulcer), topical fluorometholone 0.1% or prednisolone acetate 0.5–1% are used as a short course (1–2 weeks, tapering). They rapidly suppress the eosinophilic inflammation and enable shield-ulcer healing. CAUTION: Prolonged topical steroids cause steroid-induced glaucoma (IOP rise in ~30% of steroid responders) and posterior subcapsular cataract — use for the shortest effective duration only, under ophthalmologist supervision with IOP monitoring.
Step 6 — Topical cyclosporine (for steroid-dependent VKC):
Cyclosporine 0.05% or 1% eye drops inhibit T-cell activation and IL-2 production (targeting the Type IV component of VKC) and allow steroid reduction or cessation. Evidence supports its use in moderate-to-severe VKC resistant to mast-cell stabilisers + antihistamines.
Shield ulcer management specifically:
- Topical corticosteroids (short course) to reduce the underlying inflammation.
- Lubricants to facilitate re-epithelialisation.
- Bandage soft contact lens to protect the corneal surface during healing.
- Giant-papilla excision (mechanical debridement or surgical) if papillae are causing persistent corneal trauma.
- Topical antibiotics: added prophylactically to prevent secondary infection in the ulcer, NOT as primary treatment.
Systemic antihistamines: Oral cetirizine or fexofenadine provide adjunctive relief (especially for concurrent rhinitis) but topical therapy is more effective for ocular symptoms with fewer systemic side effects.
SELF-CHECK
A 13-year-old boy with known VKC is started on topical prednisolone 1% four times daily for a severe flare. Which monitoring requirement is mandatory during this treatment?
A. Monthly CBC to detect corticosteroid-related bone marrow suppression
B. IOP measurement to detect steroid-induced glaucoma
C. Serum cortisol to detect systemic HPA-axis suppression
D. Slit-lamp examination for posterior vitreous detachment
Reveal Answer
Answer: B. IOP measurement to detect steroid-induced glaucoma
Topical corticosteroids cause IOP elevation (steroid-induced glaucoma) in approximately 30% of patients ('steroid responders') through reduced aqueous outflow via the trabecular meshwork. In VKC patients — who are often young with a long treatment course anticipated — IOP must be measured at every visit during steroid use. The IOP rise can be dramatic (up to 50–60 mmHg) and lead to optic nerve damage if undetected. This is why topical steroids in VKC should be supervised by an ophthalmologist with access to tonometry, used for the shortest necessary duration, and replaced by cyclosporine for chronic maintenance where possible.
Self-Assessment
Review your mastery of the OP3.4 requirements. You should be able to enumerate the five forms of allergic conjunctivitis (SAC, PAC, VKC, AKC, GPC) with their typical patient demographics; explain the dual Type I + Type IV immunological mechanism of VKC and why antihistamines alone are insufficient; identify the three pathognomonic signs of VKC (giant papillae >1 mm, Trantas dots, shield ulcer) and their locations; explain the pathogenesis of the shield ulcer and why it is not treated with antibiotics as the primary drug; and describe the stepped management from allergen avoidance through mast-cell stabilisers, antihistamines, and short-course steroids to cyclosporine. Paying particular attention to the shield ulcer question: the ability to explain why a fluorescein-staining grey oval corneal ulcer in the upper-central cornea of a young VKC patient is NOT a bacterial corneal ulcer — and therefore should not be managed with intensive topical fluoroquinolones as the primary treatment — is one of the highest-yield clinical reasoning tests in this entire module. The correct reasoning chain (giant papillae → eosinophil MBP deposition on corneal epithelium → epithelial breakdown → superficial shield ulcer → treated with topical steroids to reduce eosinophilic inflammation, not antibiotics) is the kind of mechanism-to-management link that separates a student who has read the material from one who has understood it.
Revision questions:
1. What is the cytological hallmark of VKC on conjunctival scraping and what does it secrete that causes the shield ulcer?
2. Where are Trantas dots found and what do they represent histologically?
3. Why is prolonged topical steroid use specifically dangerous in VKC, and what is the safer alternative?
4. What is the most important non-pharmacological advice for a VKC patient regarding eye rubbing?
If you cannot define Trantas dots or explain why the shield ulcer is not infective, review the examination and pathophysiology sections before your tutorials.