Page 5 of 33
OP4.2 | Congenital Corneal Anomalies and Corneal Inflammations — SDL Guide (Part 2)
Corneal Inflammations: Classification and Approach
Corneal inflammation — keratitis — is classified primarily by depth of involvement and by aetiology. The depth classification is clinically fundamental because it directs the examination technique, the urgency, and the treatment approach.
Superficial keratitis affects the epithelium and superficial stroma. It presents with pain (due to the dense sensory innervation of the epithelium), photophobia, lacrimation, blepharospasm, and reduced visual acuity. Slit-lamp findings include epithelial irregularity, punctate staining with fluorescein or rose bengal, and superficial infiltrates. Causes include viral (adenovirus — the commonest cause of epidemic keratoconjunctivitis), bacterial (marginal keratitis from staphylococcal exotoxins at the limbus), allergic (vernal keratoconjunctivitis with superior limbal Trantas' dots and shield ulcer), and exposure keratitis (lagophthalmos from facial nerve palsy).
Interstitial keratitis (IK) is inflammation within the corneal stroma WITHOUT primary epithelial ulceration. This distinction is important: the surface epithelium is intact (no fluorescein staining of the cornea itself initially), but the deep stroma shows haziness, deep vascularisation ('brush-fire' pattern of deep vessels entering from the limbus), and ciliary flush. It is caused by immune-mediated reactions to organisms (often as a hypersensitivity phenomenon) rather than direct microbial invasion of the stroma. Key causes: treponema pallidum (syphilis — historically the commonest cause globally), Mycobacterium tuberculosis, herpes simplex and herpes zoster viruses, and Cogan's syndrome.
Additional classification by aetiology — bacterial, viral, fungal, parasitic — is addressed in detail in SDL 3 (Infective Keratitis), where the classic differential diagnosis of corneal ulcer is the core competency.
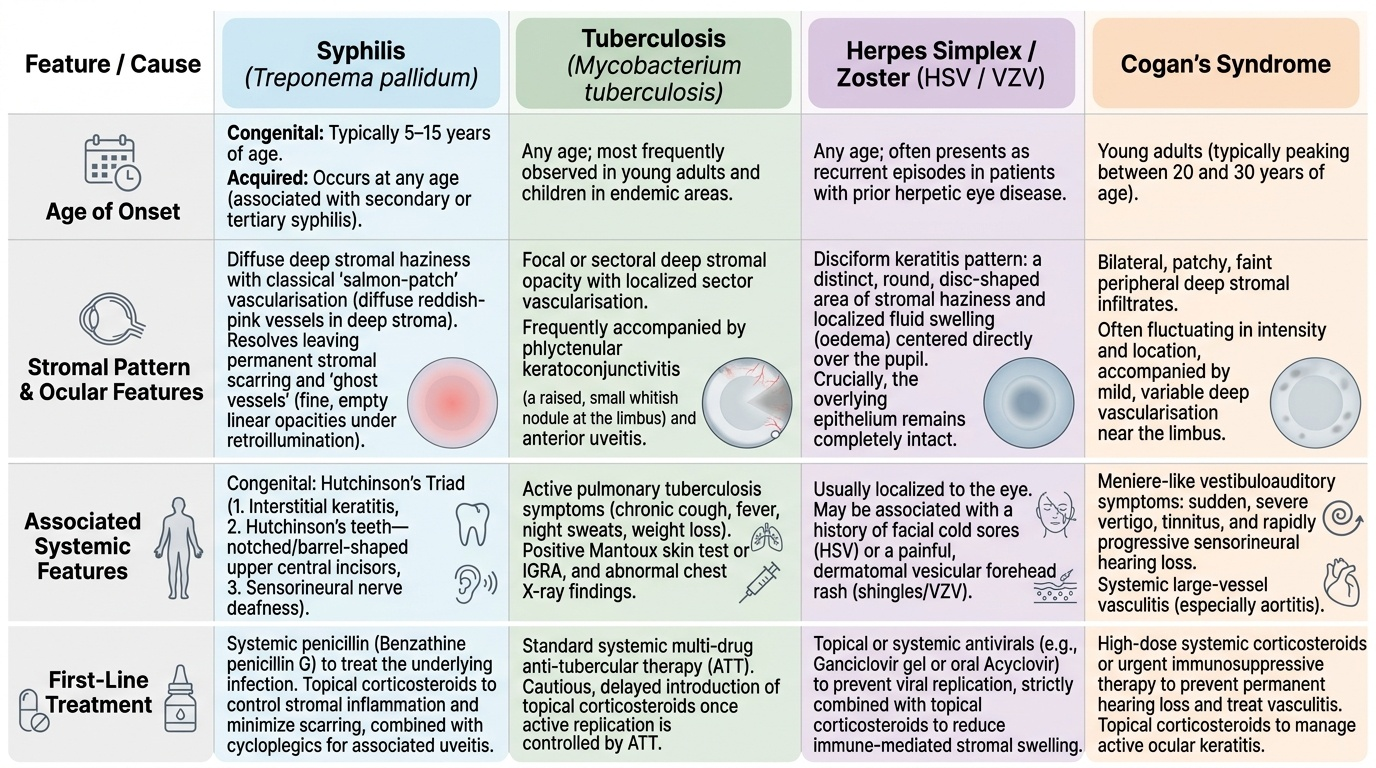
Interstitial Keratitis: Causes, Features and Differential Diagnosis
Interstitial keratitis (IK) is the hallmark ocular manifestation of several systemic infections and one autoimmune syndrome. Recognising it as stromal — not epithelial — is the first step; identifying the cause requires examining the whole patient, not just the eye.
Provided image
Syphilitic interstitial keratitis (caused by Treponema pallidum) is the prototype. In congenital syphilis, IK typically appears between ages 5 and 15 years as part of Hutchinson's triad: (i) interstitial keratitis, (ii) Hutchinson's teeth (notched or barrel-shaped upper central incisors), and (iii) nerve deafness. The IK begins unilaterally with deep stromal haziness and salmon-patch vascularisation — a diffuse reddish-pink deep stromal vascularisation. Both eyes are usually affected sequentially within months. The acute phase resolves, often leaving permanent stromal scarring and ghost vessels — empty, non-functional blood vessel channels in the stroma visible as fine linear opacities, particularly with retroillumination. In acquired syphilis (secondary or tertiary), IK may also occur, presenting with similar deep stromal features. Diagnosis requires serological testing: VDRL (non-specific; may be negative in late disease), FTA-ABS or TPHA (specific treponemal tests). Treatment: systemic penicillin (benzathine penicillin G) addresses the underlying infection; topical corticosteroids reduce the stromal inflammatory reaction and may prevent vascularisation; cycloplegics for uveitis.
Tuberculous interstitial keratitis is less common and typically causes a focal or sectoral deep stromal opacity with sector vascularisation rather than the diffuse salmon-patch pattern of syphilis. It is associated with phlyctenular keratoconjunctivitis (raised whitish nodule at the limbus — a hypersensitivity reaction to mycobacterial proteins) and anterior uveitis. Diagnosis: Mantoux test, IGRA, chest X-ray. Treatment: anti-tubercular therapy.
Herpetic interstitial keratitis (HSV or VZV) produces a disciform pattern of stromal oedema — a round, disc-shaped area of stromal haziness and oedema centred on the pupil — or a more diffuse necrotising stromal keratitis. Unlike surface HSV keratitis (dendritic ulcer staining with fluorescein and rose bengal), herpetic IK has an intact epithelium. Diagnosis is clinical; HSV PCR of aqueous can confirm in uncertain cases. Treatment: oral aciclovir + topical corticosteroids (to suppress the stromal inflammatory component).
Cogan's syndrome is a rare autoimmune condition characterised by non-syphilitic interstitial keratitis combined with audio-vestibular symptoms (fluctuating sensorineural hearing loss, vertigo — mimicking Ménière's disease). It is mediated by autoantibodies against inner ear and corneal antigens. Treatment: systemic corticosteroids and immunosuppression.
| Cause | Typical Age | Corneal Pattern | Systemic Features | Diagnostic Test | Treatment |
|---|---|---|---|---|---|
| Congenital syphilis | 5–15 years | Diffuse salmon-patch vascularisation; ghost vessels | Hutchinson's teeth, nerve deafness | VDRL, FTA-ABS | Penicillin + topical steroids |
| Acquired syphilis | Adults | Deep stromal haziness ± vascularisation | Rash, condylomata lata | VDRL, TPHA | Penicillin + topical steroids |
| Tuberculosis | Any age | Focal/sectoral opacity + sector vessels | Phlyctenule, uveitis | Mantoux, IGRA, CXR | Anti-TB therapy |
| HSV/VZV | Any age | Disciform oedema (central disc-shape) | Lip/skin vesicles (HSV) or dermatomal rash (VZV) | Clinical; HSV PCR aqueous | Aciclovir + topical steroids |
| Cogan's syndrome | Young adults | Non-syphilitic IK, bilateral | Hearing loss, vertigo | Autoantibody screen, MRI | Systemic steroids + immunosuppression |
SELF-CHECK
A 10-year-old girl presents with bilateral deep corneal haziness and 'salmon-pink' deep vascular engorgement. She has notched upper central incisors. Her hearing test shows bilateral sensorineural hearing loss. What is the diagnosis and which serological test is most specific?
A. Cogan's syndrome; autoantibody panel
B. Congenital syphilis (Hutchinson's triad); FTA-ABS or TPHA is the most specific test
C. Tuberculous interstitial keratitis; Mantoux test is diagnostic
D. HSV interstitial keratitis; HSV PCR from aqueous humour
Reveal Answer
Answer: B. Congenital syphilis (Hutchinson's triad); FTA-ABS or TPHA is the most specific test
This is Hutchinson's triad of congenital syphilis: interstitial keratitis (salmon-patch deep corneal vascularisation) + Hutchinson's teeth (notched incisors) + nerve deafness. The FTA-ABS (fluorescent treponemal antibody-absorption) and TPHA (Treponema pallidum haemagglutination assay) are specific treponemal tests. VDRL is non-specific and may be negative in late congenital syphilis. Cogan's syndrome also causes IK and audio-vestibular symptoms but not dental anomalies. TB typically causes a focal/sectoral pattern, not the classic salmon-patch.
Investigation and Management Principles
The investigation approach for congenital corneal anomalies follows a sequence: confirm the anatomical diagnosis (slit-lamp, corneal topography, anterior segment OCT), measure IOP (always — to exclude glaucoma), assess visual function (fixation behaviour in infants, visual acuity in older children), and then identify associated systemic anomalies. For Peters' anomaly and sclerocornea, genetic consultation and systemic examination are essential. Electroretinography (ERG) and visual evoked potentials (VEP) assess retinal and visual pathway function when the media opacity prevents fundal examination.
For corneal inflammations, investigations are stratified by suspected aetiology. For interstitial keratitis, the systemic workup is paramount: serological testing for syphilis (VDRL + specific treponemal test), TB evaluation (Mantoux/IGRA + chest X-ray), viral PCR for HSV/VZV, audiological assessment (Cogan's). Corneal scraping for microbiology is used when surface ulceration is present (as in infective keratitis — covered in SDL 3).
Management principles for congenital anomalies: optical rehabilitation (spectacles, contact lenses, or keratoplasty depending on severity), amblyopia treatment (patching) if one eye is more affected, glaucoma management, and genetic counselling. For keratoconus: CXL for progressive disease, contact lenses for moderate, keratoplasty for advanced. For IK: treat the underlying systemic disease; use topical corticosteroids and cycloplegics to suppress ocular inflammation and prevent posterior synechiae. Ghost vessels after IK treatment indicate resolved but previously severe disease.
CLINICAL PEARL
The key differentiator between megalocornea and buphthalmos is the intraocular pressure and Haab's striae. Megalocornea: IOP normal (10–21 mmHg), cornea clear, no Haab's striae. Buphthalmos (congenital glaucoma): IOP elevated, cornea oedematous and cloudy, horizontal Haab's striae visible in Descemet's membrane. Don't miss congenital glaucoma — it is treatable with surgery (trabeculotomy/goniotomy) and blindness is preventable if caught early.
Self-Assessment: Anomalies and Inflammations
Apply your knowledge to these scenarios before reviewing the summary.
Scenario 1: A 16-year-old male notices his vision getting worse despite frequent spectacle changes. His current glasses give 6/18. Slit-lamp reveals Fleischer's ring. Corneal topography shows 3.5 D of irregular inferior-steepening astigmatism. What is the diagnosis? What is the next investigation to confirm progression, and what is the first-line treatment to halt it? (Answer: keratoconus. Confirm progression with serial topography (increasing keratometry values over 3–6 months). First-line treatment: corneal collagen cross-linking if he is 14+ years, thin stroma >400 µm, and progressive.)
Scenario 2: A newborn's eyes appear opaque centrally. You see a dense central white opacity in both corneas at birth. Anterior segment OCT shows absent posterior corneal layers centrally with iridocorneal adhesions. What is the diagnosis and the two priorities in management? (Answer: Peters' anomaly. Priorities: (1) urgent assessment for glaucoma (IOP measurement under anaesthesia); (2) plan for early keratoplasty and intensive amblyopia management to give any chance of useful vision.)
Scenario 3: Distinguish between the corneal signs in Hutchinson's triad IK vs herpetic disciform keratitis. (Answer: Syphilitic IK — bilateral, diffuse salmon-patch deep vascularisation; ghost vessels after healing. Herpetic disciform — unilateral, central disc of stromal oedema without vascularisation initially, may have a history of recurrent surface HSV dendrites.)