Page 7 of 33
OP4.3 | Infective Keratitis: Differential Diagnosis and Management — SDL Guide
Learning Objectives
- Enumerate the differential diagnosis of infective keratitis (corneal ulcer) by causative organism category
- Describe the aetiopathogenesis, clinical features, and slit-lamp signs of bacterial, fungal, HSV, and Acanthamoeba keratitis
- Identify the staining characteristics that distinguish HSV dendritic ulcer from other types
- Select the correct antimicrobial class for each type of infective keratitis and avoid cross-type treatment errors
- Outline the investigation protocol for corneal ulcer including corneal scraping and culture media
- Recognise the complications of untreated keratitis and their clinical management
INSTRUCTIONS
Infective keratitis — corneal ulceration caused by a pathogen — is one of the leading causes of monocular blindness in India. Unlike other forms of blindness, corneal blindness from keratitis is largely preventable with prompt and accurate diagnosis. The critical skill is identifying WHICH type of keratitis you are facing before starting treatment — because bacterial antibiotics will not help a fungal ulcer, antifungals will not help a herpes simplex ulcer, and treating a dendritic HSV ulcer with steroids alone (without antiviral cover) is a treatment catastrophe. This module teaches the pattern recognition framework for making that distinction at the bedside.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive at your eye outpatient department on a Monday morning. Patient A is a 30-year-old construction worker from rural Karnataka who noticed a painful, white spot in his eye four days ago after a thorn pricked it while clearing undergrowth. The spot has grown slowly and looks grey-white, not violently red. Patient B is a 24-year-old software engineer who wears monthly silicone hydrogel contact lenses and woke yesterday with severe, almost unbearable pain in the right eye, marked redness, and a creamy-white spot near the centre of the cornea. The pain is so severe it seems out of proportion — he says it 'feels like a nerve is on fire.' Same presenting complaint: painful white corneal opacity. Completely different organisms. Fatally different treatment requirements.
WHY THIS MATTERS
Corneal ulcer — infective keratitis — is the second commonest cause of monocular blindness in India after cataract, and unlike cataract, a corneal scar left by untreated or mistreated keratitis is irreversible without keratoplasty. In rural India, fungal keratitis from agricultural trauma is epidemic — yet antifungals are still underused because many healthcare workers default to antibiotics. The treatment mnematch kills corneas. This module is the single highest-impact clinical decision-making SDL in ophthalmology for a doctor working in rural India.
RECALL
From SDL 1: the corneal epithelium is the primary barrier against microbial invasion. Disruption by trauma, contact lens wear, or surgery creates the portal of entry. From SDL 1: the corneal stroma, once infiltrated by inflammatory cells and microbial products, loses the regular collagen spacing required for transparency — hence the white opacity of a corneal ulcer. From general microbiology: Gram-positive cocci (Staphylococcus, Streptococcus) stain purple on Gram stain; Gram-negative rods (Pseudomonas) stain red. From pharmacology: fluoroquinolones (ciprofloxacin, moxifloxacin) are broad-spectrum antibiotics covering most corneal bacteria; natamycin is a polyene antifungal with activity against filamentous fungi; aciclovir is a guanosine analogue antiviral active against HSV.
Clinical Presentation of Corneal Ulcer: Red Flags and Initial Assessment
All forms of infective keratitis share a core presenting syndrome that brings the patient to attention: pain (due to the dense trigeminal innervation of the cornea), photophobia, lacrimation, blepharospasm, and reduced visual acuity. This triad of pain + photophobia + visual impairment in a red eye is the clinical alarm that must not be dismissed as 'simple conjunctivitis'. The danger signs that indicate a sight-threatening cause — keratitis, uveitis, acute glaucoma — are: ciliary flush (a ring of deep red/violet injection around the cornea, from the limbal vessels), reduced or asymmetric visual acuity, corneal opacity or cloudiness, irregular or fixed pupil, and pain that is deep rather than surface gritty.
A corneal ulcer is clinically defined as an epithelial defect with underlying stromal infiltration and necrosis. On slit-lamp examination with fluorescein: the epithelial defect stains bright green (fluorescein pools in the gap where the tight epithelial barrier is broken). The surrounding stroma shows a grey-white infiltrate — aggregated inflammatory cells and necrotic stromal tissue. The infiltrate's character — its margins, satellite lesions, depth, and any hypopyon — is the first set of diagnostic clues to the causative organism.
The history provides additional clues: agricultural or vegetative trauma (thorn, paddy husk, hay) → fungal; contact lens wear (especially extended/continuous wear, tap-water use for lens rinsing) → bacterial Pseudomonas or Acanthamoeba; previous cold sore / labial herpes, recurrent eye episodes → HSV; immunocompromised state → Candida. The initial bedside assessment sets the diagnostic hypothesis before corneal scraping results return — because treatment often must begin empirically.
The key bedside examination steps: (1) Measure visual acuity in both eyes. (2) Assess corneal clarity — slit-lamp with white light, then with fluorescein and cobalt blue light. (3) Look for hypopyon — a layered white exudate in the inferior anterior chamber, indicating severe inflammatory reaction (not infection of the anterior chamber itself). (4) Check the pupillary light reflex. (5) Take a careful history of onset, trauma, contact lens use, systemic illness.
Bacterial Keratitis: Features, Risk Factors and Management
Bacterial keratitis is the most common type of infective keratitis in urban settings and contact-lens wearers. It is characterised by rapid progression — often reaching maximum size within 24–48 hours of onset — and a dense, creamy-white anterior stromal infiltrate with an irregular, indistinct infiltrate border and considerable surrounding oedema.
The commonest organisms are: Pseudomonas aeruginosa (Gram-negative rod) — the most frequent in contact-lens wearers, causing rapidly destructive, ulcers with mucopurulent discharge and a greenish tinge to the infiltrate; Staphylococcus aureus (Gram-positive coccus) — common in post-traumatic and post-operative settings; Streptococcus pneumoniae — associated with prior ocular surface disease (dacryocystitis, dry eye); and Moraxella lacunata — in debilitated, alcoholic, or malnourished patients.
Hypopyon — a white, layered, non-viscous exudate of fibrin and leukocytes settling inferiorly in the anterior chamber — is the hallmark of severe bacterial (and fungal) keratitis. It is a sterile inflammatory response (aqueous itself is not infected in early keratitis), and it shifts with head position ('hypopyon shifts'). Its presence indicates a severe inflammatory burden and demands aggressive treatment. The hypopyon's size does NOT directly indicate AC infection — only in endophthalmitis does the AC truly become infected.
Investigation: corneal scraping is performed under topical anaesthesia, scraping the active edge and base of the ulcer with a sterile Kimura spatula or 23-gauge needle tip. Material is inoculated directly onto blood agar (for bacteria), chocolate agar (for fastidious organisms), Sabouraud's dextrose agar (for fungi), and a glass slide is prepared for Gram stain and Giemsa stain. Results take 24–48 hours for bacteria, 72 hours+ for fungi.
Treatment: empirical fortified topical antibiotics (combination of fortified vancomycin 5% hourly — for Gram-positive cover — and fortified tobramycin or cefazolin for Gram-negative cover), or a fluoroquinolone (ciprofloxacin 0.3% or moxifloxacin 0.5% hourly). As culture results become available, therapy is refined. Systemic antibiotics are rarely needed for keratitis alone unless scleritis or orbital involvement develops. Adjuncts: cycloplegics (cyclopentolate or atropine) to relieve ciliary spasm and prevent posterior synechiae; dark glasses for photophobia; never patch an infected eye.
Bacterial keratitis is a medical emergency — delay of even 12–24 hours can result in perforation in rapidly progressive Pseudomonas ulcers.
SELF-CHECK
A 28-year-old contact lens wearer presents with a rapidly progressive corneal ulcer with mucopurulent discharge, a dense creamy infiltrate, and a 2 mm hypopyon. Corneal scraping Gram stain shows Gram-negative rods. Which organism is most likely, and what is the appropriate empirical treatment?
A. Staphylococcus aureus; topical vancomycin 5% hourly
B. Pseudomonas aeruginosa; topical ciprofloxacin 0.3% or moxifloxacin 0.5% hourly
C. Fusarium species; topical natamycin 5% hourly
D. Herpes simplex virus; topical aciclovir 3% ointment five times daily
Reveal Answer
Answer: B. Pseudomonas aeruginosa; topical ciprofloxacin 0.3% or moxifloxacin 0.5% hourly
Pseudomonas aeruginosa is the most common Gram-negative cause of bacterial keratitis in contact lens wearers. A rapidly progressive ulcer with mucopurulent discharge and Gram-negative rods on scraping is classic. Fluoroquinolones (ciprofloxacin, moxifloxacin) are appropriate empirical first-line agents against Pseudomonas. Natamycin is an antifungal (wrong class for a Gram-negative bacterial infection); aciclovir is an antiviral. Vancomycin covers Gram-positive organisms.
Fungal Keratitis: Features, Risk Factors and Management
Fungal keratitis is the dominant form of infective keratitis in rural India, particularly in agricultural communities. The classic history is injury with a vegetative/agricultural implement — a thorn, paddy husk, sugarcane leaf, or tree branch. This vegetative material carries Aspergillus or Fusarium spores directly into the corneal stroma. The two most common causative organisms in India are Fusarium solani and Aspergillus flavus, both filamentous fungi that grow as branching hyphal networks within the stroma. Unlike bacteria, which trigger an intense acute neutrophilic response that rapidly liquefies tissue, fungal pathogens elicit a slower, more granulomatous-type response — explaining why fungal keratitis has a subacute onset and why the infiltrate looks dry and grey-white rather than creamy and purulent. This temporal mismatch — slower progression but ultimately worse structural destruction — is precisely why the diagnosis is so frequently delayed: the clinician is lulled into a false sense of security by the slower timeline. The onset is subacute — typically 5–14 days after the inciting trauma — with a characteristic constellation of slit-lamp findings that the experienced clinician learns to recognise and that are mechanistically explicable: each feature reflects fungal biology rather than arbitrary morphology.
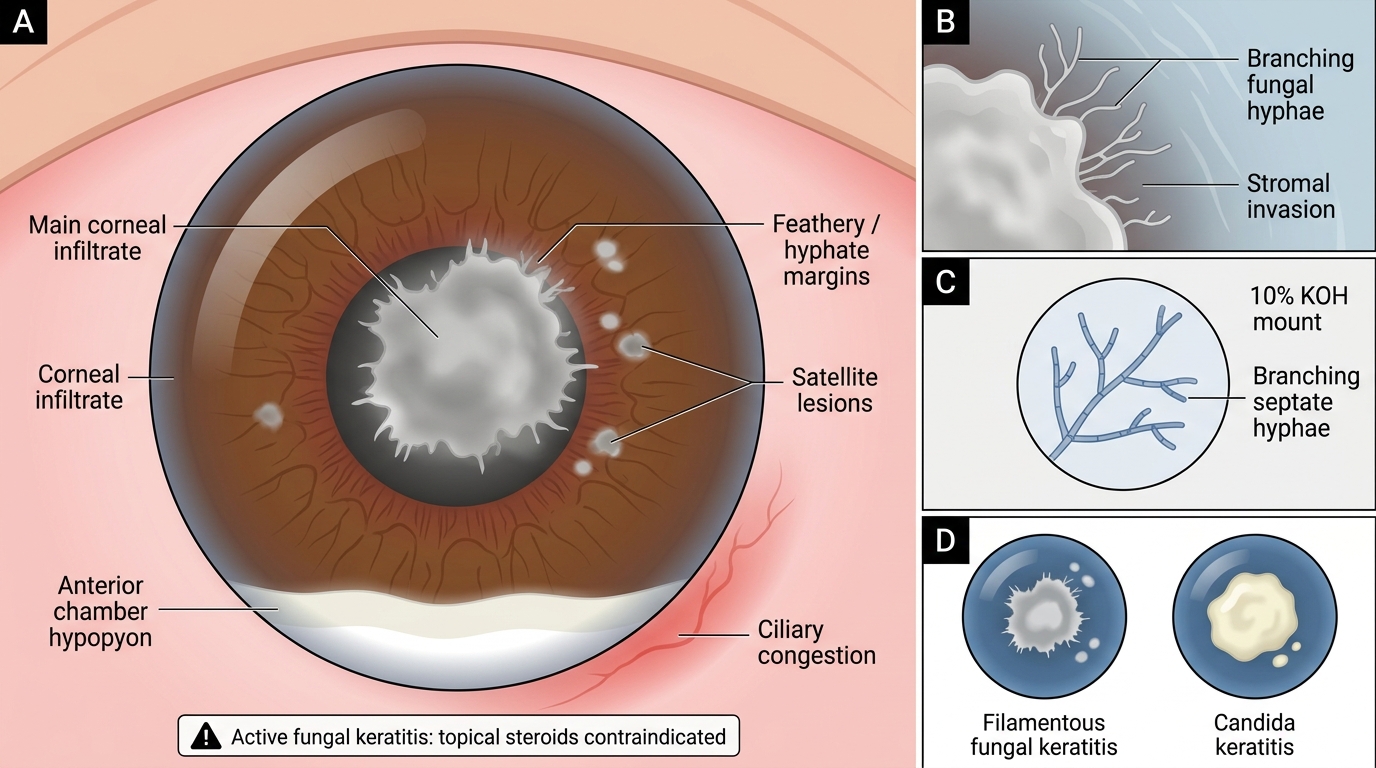
The pathognomonic slit-lamp features of filamentous fungal keratitis are:
- Feathery or hyphate margins — the infiltrate edge has irregular, feather-like extensions (reflecting hyphal growth into the surrounding stroma)
- Satellite lesions — small round infiltrates around the main ulcer, following the direction of hyphal spread
- Dry, greyish-white infiltrate texture (in contrast to the wet, creamy bacterial infiltrate)
- Endothelial plaque — a thick, yellowish-white inflammatory deposit on the endothelial surface behind the ulcer, visible on slit-lamp as a posterior corneal opacity
- Hypopyon — present but tends to be thicker and more viscous than in bacterial keratitis (fungal hypopyon is less mobile, does not shift as freely)
Fungal Corneal Ulcer: Key Diagnostic Features
Candida keratitis is different from filamentous fungal keratitis: it presents in contact-lens wearers, immunocompromised patients, or those on chronic topical steroids; the infiltrate is more creamy and less feathery; satellite lesions are less prominent. Candida is a yeast (not a filamentous fungus).
Investigation: corneal scraping KOH mount (10% KOH dissolves cellular material, leaves fungal hyphae visible as branching, septate structures under microscopy). Sabouraud's dextrose agar culture is specific but takes 72 hours or longer. Confocal microscopy can demonstrate fungal hyphae in vivo and is increasingly available.
Treatment: natamycin 5% eye drops (a polyene antifungal) is the first-line agent for filamentous fungi (Aspergillus, Fusarium) — it is effective because its mechanism targets ergosterol in the fungal cell membrane. Dosing is typically hourly for the first 48 hours. Voriconazole 1% (topical) is an alternative with broader-spectrum activity, preferred for Aspergillus and when natamycin is unavailable. Systemic antifungals (oral voriconazole or itraconazole) are added for deep or severe infections, or when scleral spread is suspected. Duration of treatment is prolonged — 6–12 weeks is common. Topical steroids are absolutely contraindicated in active fungal keratitis.
SELF-CHECK
A 45-year-old farmer presents with a 10-day history of right eye pain after being scratched by a paddy stalk. Slit-lamp shows a grey-white corneal infiltrate with feathery margins, multiple satellite lesions, and an endothelial plaque. KOH mount of corneal scraping shows branching septate hyphae. What is the first-line topical treatment?
A. Topical ciprofloxacin 0.3% every hour
B. Topical aciclovir 3% ointment five times daily
C. Topical natamycin 5% every hour
D. Topical prednisolone 1% four times daily
Reveal Answer
Answer: C. Topical natamycin 5% every hour
The history (vegetative trauma — paddy stalk), slit-lamp findings (feathery margins, satellite lesions, endothelial plaque), and KOH mount (branching septate hyphae) confirm filamentous fungal keratitis. Natamycin 5% is the first-line topical antifungal for filamentous fungi. Ciprofloxacin is a bacterial antibiotic (no antifungal activity). Aciclovir is an antiviral. Prednisolone alone would worsen fungal keratitis catastrophically — steroids are absolutely contraindicated in active fungal infection.