Page 8 of 18
OP6.3 | Hyphema and Hypopyon: Clinical Distinction and Causes — SDL Guide
Learning Objectives
- Distinguish hyphema from hypopyon clinically on the basis of colour, aetiology, associated features, and IOP profile
- Enumerate the causes of hyphema (traumatic, spontaneous) and hypopyon (sterile, infective)
- Grade traumatic hyphema and identify the complications specific to each grade
- Outline the management priorities for traumatic hyphema and for hypopyon, including when to suspect infective endophthalmitis
INSTRUCTIONS
A visible collection in the anterior chamber — whether red or white — is an emergency sign that demands immediate attention and correct interpretation. Hyphema (blood) and hypopyon (white cells) are clinically similar in appearance (both form a horizontal level in the lower anterior chamber) but arise from completely different mechanisms and demand opposite initial management priorities. Confusing them — or failing to distinguish infective from sterile hypopyon — can result in vision loss from delayed treatment of endophthalmitis or from inappropriate surgery in a traumatic eye. This module gives you the clinical reasoning framework to never confuse these two entities again.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch. 8 — Diseases of the Uveal Tract; Ch. 19 — Injuries to the Eye (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch. 17 — The Uveal Tract; Ch. 29 — Injuries of the Eye (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients present within the same hour to your eye casualty. Patient A is a 19-year-old cricketer hit in the eye by a ball. His eye is painful, vision is reduced to counting fingers, and you see a dark red fluid level in the lower third of his anterior chamber. Patient B is a 55-year-old who had cataract surgery 36 hours ago. She reports pain, severe redness, and decreasing vision since this morning. You see a creamy white fluid level in the lower quarter of her anterior chamber, and the vitreous looks hazy. Both patients have a 'level' in their anterior chamber — but they could not be more different in urgency and management. What is in each patient's eye, what caused it, and what are your immediate priorities?
WHY THIS MATTERS
Hyphema and hypopyon are two of the most visually dramatic and diagnostically important signs in ophthalmology — and both can occur in a general practitioner's or emergency physician's consultation room, not just in specialist settings. Knowing how to distinguish them allows you to triage correctly: a traumatic hyphema needs rest, IOP monitoring, and referral; a post-operative hypopyon with vitreous involvement needs immediate intravitreal antibiotics within hours to prevent permanent blindness from bacterial endophthalmitis. Failing to recognise the urgency gradient between sterile and infective hypopyon is a serious clinical error.
RECALL
From OP6.1 and OP6.2, recall that the anterior chamber is the fluid-filled space between the cornea anteriorly and the iris/lens posteriorly, containing aqueous humour secreted by the ciliary body. Normal aqueous is crystal clear. Also recall that hypopyon was introduced in OP6.1 as a possible sign of severe iridocyclitis — a white layer of cells in the inferior AC. Here you will learn the full differential (it can also be infective). From your anatomy studies, recall that the iris root — where the iris attaches to the ciliary body at the angle — contains a rich vascular arcade fed by the long and short posterior ciliary arteries via the major arterial circle of the iris. This is the anatomical basis for why blunt trauma to the globe so commonly produces hyphema: the iris root vessels are the most vulnerable to shear forces from a blunt impact.
The Anterior Chamber Collection: Hyphema vs Hypopyon at First Sight
When you look at a patient's anterior chamber and see a horizontal level of material settling in the inferior portion of the eye, you are seeing one of two things: blood (hyphema) or white cells (hypopyon). The distinction is usually immediately apparent from colour — but it requires more than colour to determine the aetiology and urgency.
Hyphema is the presence of red blood cells in the anterior chamber. The blood settles under gravity to form a characteristic red or dark red horizontal level in the inferior AC. In very fresh haemorrhage, the blood may be bright red; older blood darkens to dark red or mahogany-brown as the red cells break down. A very severe (Grade IV or 'total') hyphema fills the entire anterior chamber with dark clotted blood, creating the dramatic appearance known as the 8-ball hyphema or blackball hyphema — the whole eye appears dark through the cornea.
Hypopyon is the presence of white blood cells (leucocytes), fibrin, and inflammatory protein, which settle in the inferior AC as a white or cream-coloured level. It is gravity-dependent (like hyphema) but is white/cream rather than red. Because it contains cells rather than blood, it moves and shifts with positional change — if the patient tilts their head, the level shifts accordingly.
Both conditions are visible to the naked eye (without slit-lamp) if the collection is large enough, making them uniquely recognisable clinical signs even outside ophthalmology settings.
Anatomy of the Anterior Chamber and Why Collections Layer Here
The anterior chamber is a closed compartment bounded anteriorly by the corneal endothelium and posteriorly by the iris diaphragm and the anterior lens surface. It communicates with the posterior chamber (between the iris and lens) through the pupil. Aqueous humour, which fills both chambers, drains from the anterior chamber through the trabecular meshwork at the angle (where the cornea meets the root of the iris), and then into Schlemm's canal and the episcleral venous system.
Why do blood and cells layer in the inferior anterior chamber? The anterior chamber has a volume of approximately 0.25 mL of aqueous. When blood or inflammatory cells enter this enclosed space, they mix initially but settle rapidly under gravity to form a dependent level — collecting in the most inferior position. The cornea is essentially a windowed container: the collection is visible from the front because the cornea is transparent, and the level forms exactly where the law of gravity dictates — at the bottom of this fluid-filled chamber.
The iris root vasculature is critically important for understanding traumatic hyphema. The major arterial circle of the iris (formed by the long posterior ciliary arteries) lies within the ciliary body just posterior to the iris root. Branches from this circle supply the iris radial vessels. When blunt trauma deforms the globe, shear forces at the iris root tear these vessels — specifically the anterior ciliary arteries and iris radial vessels at the iris root — causing the haemorrhage that constitutes traumatic hyphema. This is why even moderate blunt force (a fist, a squash ball, a cork) can produce significant hyphema without penetrating the eye.
Hyphema: Causes, Grading, and Clinical Features
Hyphema — blood in the anterior chamber — occurs when vessels in or around the iris and ciliary body are disrupted. Understanding the causes determines both the immediate and subsequent management. Traumatic hyphema in a young patient from a sports injury and spontaneous hyphema in an elderly diabetic patient represent entirely different clinical scenarios that demand different investigations and different levels of systemic urgency — yet both manifest as the same red horizontal level in the inferior anterior chamber. Recognising the cause from the clinical context prevents the serious error of treating both identically. Spontaneous hyphema in any adult must never be assumed to be idiopathic: rubeosis iridis from ischaemic retinal disease, iris melanoma, and coagulopathy all require urgent systemic investigation and management that would be missed if the clinician focused only on the eye. Establishing the cause is therefore not a secondary concern after treating the hyphema — it is a simultaneous and equally urgent priority.
Causes of hyphema:
1. Traumatic (the most common cause): Blunt trauma (contusion) to the eyeball produces sudden deformation of the globe, generating shear forces at the iris root that tear the iris root vessels. Common agents: cricket/squash balls, fists, airbag deployment, rubber bullet injuries. This is the dominant cause in young patients and constitutes a true ocular emergency. A related injury is iridodialysis — avulsion of the iris root from the ciliary body.
2. Spontaneous (non-traumatic) — always signifies an underlying pathology:
- Rubeosis iridis (iris neovascularisation): New blood vessels grow on the iris surface in proliferative diabetic retinopathy, central retinal vein occlusion (CRVO), and ocular ischaemic syndrome — these fragile new vessels bleed spontaneously into the AC.
- Iris tumours: Iris melanoma or iris metastasis can bleed.
- Anticoagulation/coagulopathy: Patients on warfarin, direct oral anticoagulants (DOACs), or with haematological disorders.
- Microhaematuria syndromes: Rare (Fuchs heterochromic iridocyclitis can cause haemorrhage at surgery).
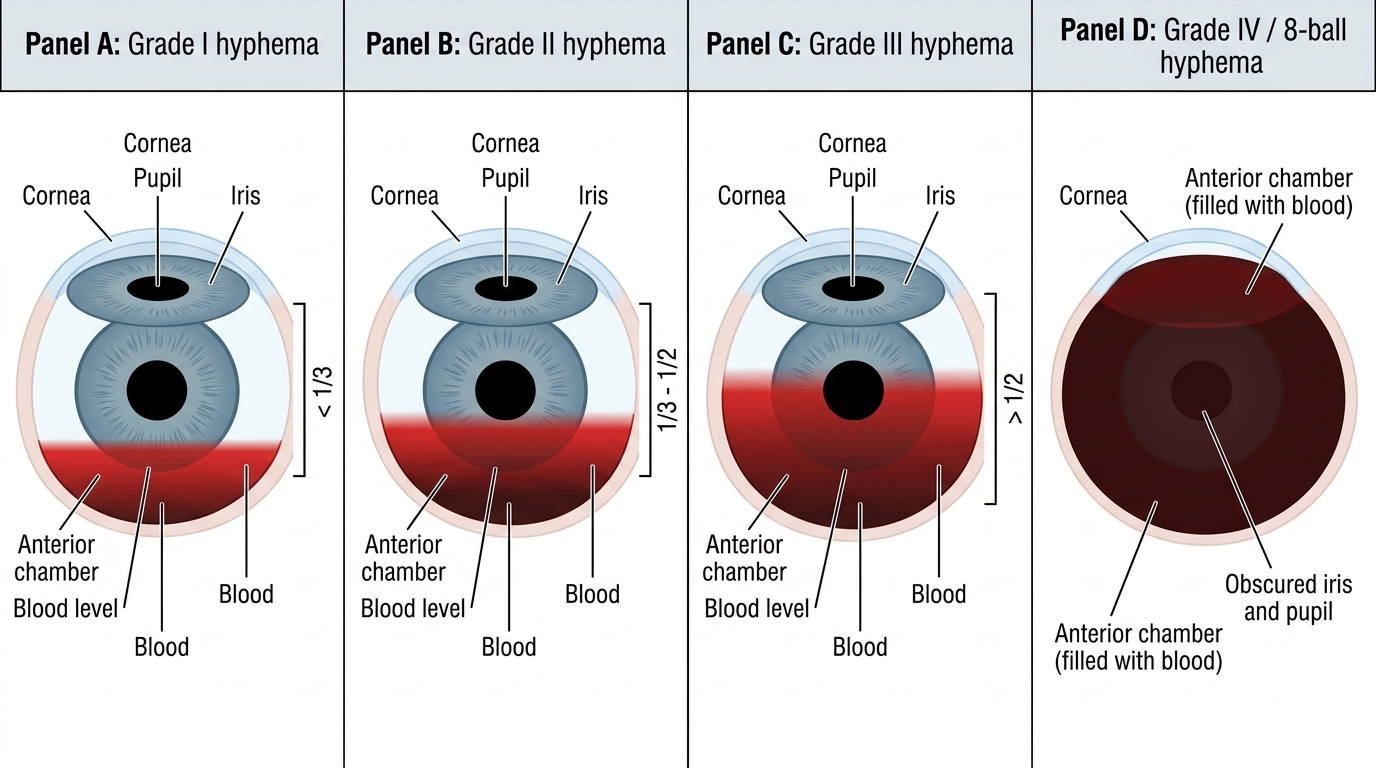
Grading of traumatic hyphema (Sheppard classification):
- Grade I: Blood fills less than 1/3 of the anterior chamber. Most common; usually resolves spontaneously.
- Grade II: Blood fills 1/3 to 1/2 of the anterior chamber.
- Grade III: Blood fills more than 1/2 but not the total AC.
- Grade IV (8-ball or blackball hyphema): Total anterior chamber filled with dark clotted blood. Most serious grade.
Clinical features: reduced visual acuity (proportional to blood volume), eye pain, photophobia, circumcorneal injection. IOP may be normal initially but can rise as blood clots block the trabecular meshwork.
Complications of traumatic hyphema:
1. Rebleed: The most feared acute complication. Fresh blood clot undergoes fibrinolysis by day 2–5, and the vessel may rebleed before it has fully healed — rebleeding produces a larger (sometimes total) hyphema and dramatically worsens the prognosis. Antifibrinolytic therapy (aminocaproic acid) is used in some centres to prevent this.
2. Corneal blood staining: Haemoglobin iron products diffuse into corneal stroma when (a) the hyphema is total (Grade IV), (b) IOP is elevated, and (c) the corneal endothelium is compromised. Corneal blood staining is a permanent, visually disabling complication that may require corneal transplantation.
3. Secondary glaucoma: Clot and red cell debris block the trabecular meshwork → raised IOP → optic nerve damage if not managed.
4. Sickle cell disease interaction: A critical special case. In patients with sickle cell disease or trait, red cells in the AC can sickle within the anaerobic, relatively acidic aqueous — the sickled cells block the trabecular meshwork very efficiently. IOP rises dramatically even with small hyphemas. Acetazolamide is AVOIDED in sickle cell disease (induces red cell sickling by causing metabolic acidosis).
Clinical Grading of Hyphema