Page 9 of 18
OP6.3 | Hyphema and Hypopyon: Clinical Distinction and Causes — SDL Guide (Part 2)
Hypopyon: Causes and Clinical Distinction from Hyphema
Hypopyon is an accumulation of leucocytes, fibrin, and inflammatory protein in the inferior anterior chamber. Unlike hyphema, which is always a vascular event, hypopyon represents an intense inflammatory or infectious process that has overwhelmed the normal barrier function of the eye. The distinction between sterile and infective hypopyon is the most clinically urgent differential in ophthalmology. Both cause the same dramatic white level in the inferior anterior chamber, yet the correct management diverges completely: sterile hypopyon from severe iridocyclitis demands aggressive corticosteroids, while infective hypopyon from bacterial endophthalmitis demands immediate intravitreal antibiotics — and administering steroids alone to an infective hypopyon will accelerate bacterial proliferation and destroy the eye within hours. No other differential in clinical ophthalmology carries a higher penalty for misclassification, which is why understanding the full spectrum of causes — and the clinical features that distinguish each — is a non-negotiable core competency at the MBBS level.
Sterile hypopyon causes (inflammatory, NOT infectious):
1. Severe iridocyclitis (anterior uveitis): The most common cause of hypopyon in a non-operative setting. In severe iridocyclitis, the inflammatory response floods the AC with white cells that settle inferiorly. The hypopyon in this context is a sterile, inflammatory collection — the eye is not infected. It should resolve with aggressive topical and systemic steroids. (Revisit OP6.1 for the other signs of iridocyclitis.)
2. Behçet's disease: A systemic vasculitis characterised by the classic triad of recurrent oral aphthous ulcers + genital ulcers + ocular inflammation. The hypopyon in Behçet's is classically described as 'migratory' or 'shifting' — it appears suddenly, may shift from one part of the AC to another, and can alternate between eyes. The uveitis is severe, bilateral, and associated with high risk of visual loss. Behçet's is most prevalent along the 'Silk Road' — Turkey, Middle East, Central Asia, and East Asia — and is male-predominant.
3. Toxic Anterior Segment Syndrome (TASS): A sterile, non-infectious, acute inflammatory reaction to intraocular substances introduced during anterior segment surgery (cataract surgery, IOL implantation). TASS typically presents within 12–48 hours of surgery, as opposed to infectious endophthalmitis which usually presents 24–72+ hours post-operatively. The hypopyon in TASS is sterile — aqueous cultures are negative — and responds to intensive topical corticosteroids.
Infective hypopyon causes (infectious — emergency):
1. Post-operative bacterial endophthalmitis: The most common cause in the post-surgical setting. Presents as rapidly worsening pain, redness, and visual loss within 24–72 hours of surgery. The causative organisms are most commonly coagulase-negative staphylococci (particularly Staphylococcus epidermidis) for late-onset cases after cataract surgery, and Staphylococcus aureus for acute post-operative cases. The vitreous is typically hazy (this distinguishes it from iridocyclitis with hypopyon, which has clear or minimally hazy vitreous).
2. Post-traumatic endophthalmitis: Following penetrating eye injury, particularly with organic/vegetable material or soil contamination. Bacillus cereus is notorious in this setting — it produces exotoxins causing rapid, devastating intraocular destruction, often within 12–24 hours.
3. Fungal endophthalmitis: More indolent course than bacterial; associated with IV drug use, immunocompromise, or systemic fungaemia. White intravitreal plaques are characteristic.
4. Corneal ulcer with anterior chamber perforation: A severe bacterial or fungal corneal ulcer may perforate, allowing organisms to enter the AC and produce hypopyon within an infectious context.
5. Endogenous endophthalmitis: Haematogenous seeding of the eye from systemic bacteraemia or fungaemia — associated with immunocompromise, liver disease, IV drug use, or indwelling catheters.
SELF-CHECK
A patient presents 36 hours after uncomplicated phacoemulsification with a painful red eye, drastically reduced vision, and a white level in the inferior anterior chamber. The vitreous appears hazy on B-scan. What is the most urgent next step?
A. Topical prednisolone acetate 1% hourly — this is TASS, which responds to steroids
B. Immediate vitreous tap and intravitreal antibiotic injection (vancomycin + ceftazidime)
C. Observation for 24 hours as early post-operative inflammation is expected
D. Oral ciprofloxacin and review in the morning
Reveal Answer
Answer: B. Immediate vitreous tap and intravitreal antibiotic injection (vancomycin + ceftazidime)
The clinical picture — acute post-operative onset (36 hours), severe pain, drastically reduced vision, hypopyon, and vitreous haze — is bacterial endophthalmitis until proved otherwise. The Endophthalmitis Vitrectomy Study (EVS) and standard guidelines demand immediate vitreous tap for culture + intravitreal antibiotics (vancomycin 1 mg/0.1 mL + ceftazidime 2.25 mg/0.1 mL or amikacin). Delay by even a few hours allows exponential bacterial proliferation and permanent retinal damage. TASS presents within 12–24 hours, usually with clear vitreous, and responds to topical steroids — but vitreous haze rules out TASS here.
Clinical Differentiation: Hyphema vs Hypopyon — A Systematic Comparison
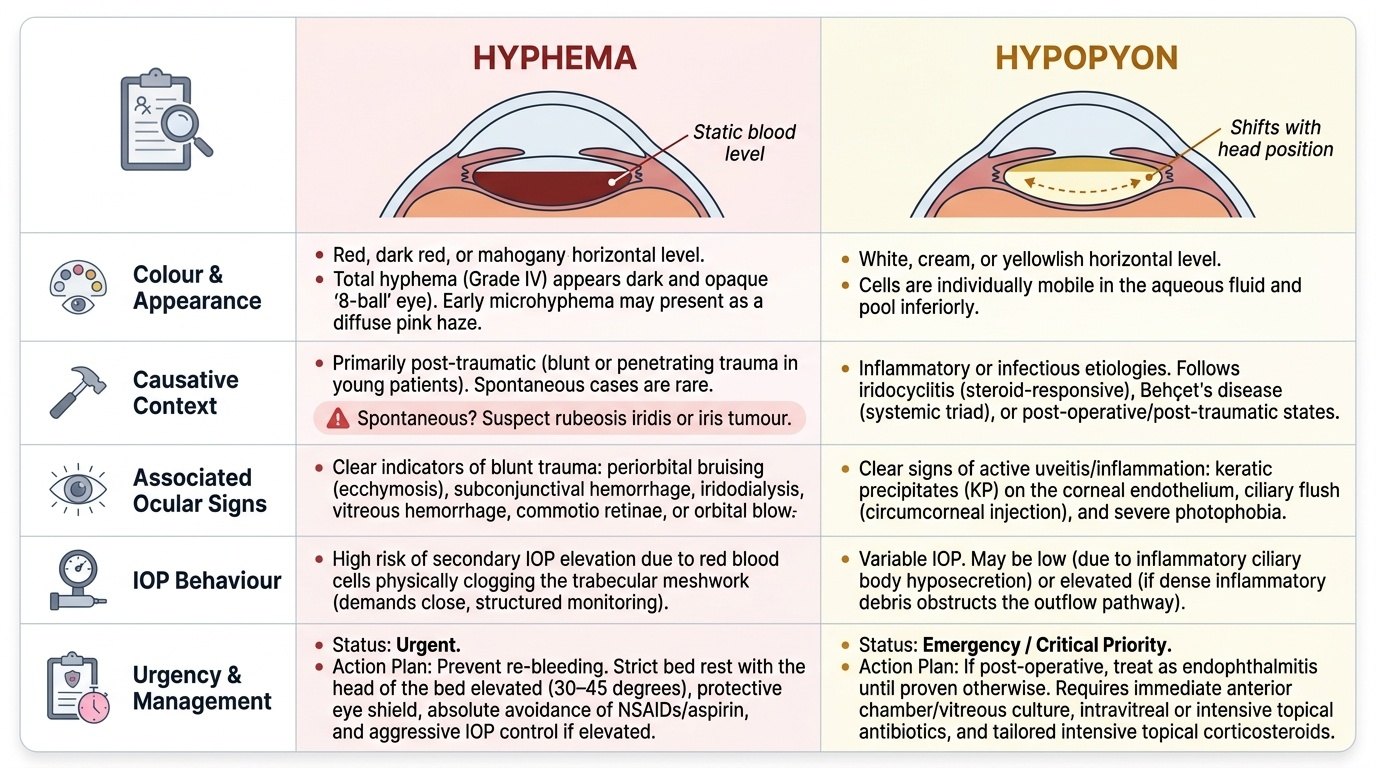
Systematic comparison of hyphema and hypopyon using five clinical axes prevents diagnostic errors even under time pressure. The five axes are: colour and appearance, causative context, associated ocular signs, IOP behaviour, and urgency and management priority. A structured comparison framework matters here precisely because both conditions present with the same anatomical phenomenon — a horizontal level in the inferior anterior chamber — and because the environments in which they appear (busy emergency departments, general practice, post-operative surgical wards) are exactly the settings where time pressure is greatest and the risk of misclassification is highest. Working systematically through all five axes, rather than relying on any single feature, ensures that rare presentations — a pale hyphema from micro-haematuria, or a post-operative red hyphema misread as blood — do not escape correct identification. The framework converts a potentially confusing diagnostic problem into a reliable, reproducible clinical habit.
Provided image
Colour and appearance:
- Hyphema: red, dark red, or mahogany-brown horizontal level. Total hyphema (Grade IV) = dark, opaque ('8-ball'). Does not shift to one side — fills the inferior AC symmetrically. Blood may appear as a diffuse pink haze if very early (microhyphema — individual red cells in AC detected by slit-lamp before a visible level forms).
- Hypopyon: white, cream, or yellowish horizontal level. Shifts with head position (cells are individually mobile in the aqueous fluid).
Causative context:
- Hyphema: almost always follows trauma (blunt or penetrating) in otherwise healthy young patients. Spontaneous hyphema should immediately raise suspicion for rubeosis iridis (diabetic retinopathy, CRVO) or iris tumour.
- Hypopyon: follows iridocyclitis (steroid-responsive), Behçet's disease (systemic triad), or post-operative/post-traumatic states (endophthalmitis — emergency). The clinical history is the single most important differentiating tool.
Associated ocular signs:
- Hyphema: usually associated with other signs of blunt trauma — periorbital bruising, subconjunctival haemorrhage, iridodialysis, vitreous haemorrhage, commotio retinae, orbital blow-out fracture. Vision varies with clot volume.
- Hypopyon: associated with signs of active inflammation — KPs on the corneal endothelium, aqueous flare, ciliary flush — in iridocyclitis. In endophthalmitis: vitreous haze/turbidity (absent or minimal in sterile uveitis), severe conjunctival injection, wound site abnormality post-operatively.
IOP behaviour:
- Hyphema: IOP is variable. Initially may be low (ciliary body trauma reduces aqueous production) or normal; rises if blood clot obstructs the trabecular meshwork. Sickle cell patients at particular risk.
- Hypopyon in iridocyclitis: IOP characteristically LOW (ciliary body inflammation reduces secretion) — as described in OP6.1.
- Hypopyon in endophthalmitis: IOP may be low (severe ciliary body destruction) or variable.
Urgency and management:
- Hyphema: urgent but not immediately minutes-level emergency in most cases. Bed rest, head-of-bed elevation (30°), shield the eye, IOP monitoring, avoid aspirin/NSAIDs (increase bleeding risk), cycloplegia, refer ophthalmology.
- Infective hypopyon: IMMEDIATE hours-level emergency — every hour of delay worsens prognosis. Vitreous tap + intravitreal antibiotics within hours. This is the most time-critical scenario in ophthalmology.
CLINICAL PEARL
The most dangerous hypopyon in clinical practice is the one that looks like 'routine post-operative inflammation.' After any intraocular surgery, a white AC level that appears rapidly (especially after 24 hours), combined with pain, falling vision, and vitreous haze, must be treated as bacterial endophthalmitis until cultures prove otherwise. Time-to-intravitreal-antibiotics is the single most important determinant of visual outcome in post-operative endophthalmitis — hours matter, not days. TASS (sterile post-op hypopyon) typically appears earlier (<24 hours post-op), has clear vitreous, and responds to topical steroids — but if in doubt, treat for endophthalmitis first.
Management Principles for Hyphema and Hypopyon
The management of hyphema and hypopyon diverges sharply depending on the diagnosis — highlighting why correct clinical differentiation is essential before any treatment is initiated. The principles that underpin each management approach are grounded in the mechanism of each condition: traumatic hyphema management is aimed at preventing rebleed (the clot must be preserved until the vessel heals), preventing trabecular obstruction from rising IOP (which risks optic nerve damage), and avoiding corneal blood staining from prolonged total hyphema with elevated IOP. Sterile hypopyon management is aimed entirely at suppressing the underlying inflammatory cascade with corticosteroids, removing the source of leucocyte recruitment into the anterior chamber. Infective hypopyon management is a time-critical antimicrobial emergency — the goal is to deliver bactericidal drug concentrations directly to the vitreous cavity before exponential bacterial growth causes irreversible retinal necrosis. Understanding these mechanistic rationales ensures that even in unusual presentations, the clinician can reason to the correct management rather than relying solely on pattern recognition.
Management of traumatic hyphema:
Conservative management (most Grade I–III cases):
- Bed rest with head of bed elevated at 30–45° — promotes gravity-dependent settling of the hyphema inferiorly, reduces rebleed risk, and allows spontaneous resorption.
- Eye shield — not a pressure pad (which increases IOP); a protective shell to prevent further trauma to the eye.
- Avoid aspirin, NSAIDs, and anticoagulants — these impair clot stability and increase rebleed risk.
- Cycloplegia (atropine 1%) — relieves ciliary spasm pain and prevents posterior synechiae.
- IOP-lowering treatment if IOP elevated — timolol, dorzolamide, or systemic acetazolamide (EXCEPT in sickle cell disease — use CAIs topically, avoid systemic acetazolamide).
- Antifibrinolytic therapy — aminocaproic acid (oral or topical) is used in some centres to prevent clot fibrinolysis and rebleed, particularly in higher-grade hyphemas.
- Topical steroids — reduce intraocular inflammation.
Surgical evacuation (select cases):
Indicated when: (a) total hyphema persists >5 days (risk of corneal blood staining); (b) IOP cannot be medically controlled (risk of optic nerve damage); (c) sickle cell disease with raised IOP not responding to medical therapy. Surgical washout through limbal incisions removes the clot mechanically.
Management of hypopyon — by aetiology:
Sterile hypopyon (iridocyclitis, Behçet's, TASS):
- Intensive topical corticosteroids (prednisolone acetate 1% hourly) — the hypopyon resolves as the underlying inflammation is suppressed.
- Cycloplegia for iridocyclitis component.
- Behçet's disease: systemic immunosuppression (colchicine, azathioprine, ciclosporin, anti-TNF agents).
- TASS: topical steroids; no antibiotics needed (sterile process).
Infective hypopyon (bacterial/fungal endophthalmitis):
- Immediate vitreous tap (aspirate from vitreous cavity for microscopy and culture) followed by intravitreal antibiotic injection — vancomycin 1 mg/0.1 mL (gram-positive coverage) + ceftazidime 2.25 mg/0.1 mL (gram-negative coverage). These are delivered intravitreally in the same session as the diagnostic tap.
- Systemic antibiotics as adjunct in severe cases.
- Pars plana vitrectomy (PPV) — the Endophthalmitis Vitrectomy Study (EVS) showed PPV superior to vitreous tap for patients with hand-movement or worse vision at presentation; for better vision (LP or better), intravitreal antibiotics alone gave equivalent results.
- Fungal endophthalmitis: intravitreal amphotericin B or voriconazole; systemic azoles (voriconazole, fluconazole).
SELF-CHECK
A 25-year-old patient with known sickle cell trait has a Grade II traumatic hyphema. His IOP is 28 mmHg. Which agent should be AVOIDED for IOP control?
A. Topical timolol 0.5%
B. Topical dorzolamide 2%
C. Systemic acetazolamide
D. Topical brimonidine 0.2%
Reveal Answer
Answer: C. Systemic acetazolamide
Systemic acetazolamide (a carbonic anhydrase inhibitor) causes metabolic acidosis, which promotes sickling of red blood cells in patients with sickle cell disease or trait. In the anaerobic, relatively acidic aqueous of the anterior chamber, sickled cells obstruct the trabecular meshwork extremely efficiently, worsening secondary glaucoma. In sickle cell patients with hyphema, use topical agents (timolol, dorzolamide, brimonidine) to control IOP; systemic acetazolamide is contraindicated.
Self-Assessment: Distinguishing and Managing Anterior Chamber Collections
The following clinical scenarios test your ability to distinguish hyphema from hypopyon, identify the most likely aetiology in each case, and select appropriate immediate management. When working through each question, articulate to yourself the key differentiating features: colour, context, vitreous clarity, IOP level, and time from any surgery or trauma. These are the five axes that separate urgent endophthalmitis (hours-to-treat) from sterile hypopyon (treat the inflammation) from traumatic hyphema (bed rest, IOP monitoring, prevent rebleed) — three conditions that look superficially similar but require fundamentally different responses. The scenarios are designed to probe exactly the points where errors are most likely: the post-operative eye that looks like routine inflammation but is not, the traumatic hyphema in a patient with an unrecognised haemoglobinopathy, and the chronic uveitis patient whose hypopyon resolves with steroids. Work through each one before reading the explanation — the diagnostic reasoning process is as important as the final answer.