Page 1 of 18
OP6.1 | Uveitis Classification and Iridocyclitis Recognition — SDL Guide
Learning Objectives
- Define uveitis and classify it anatomically using the SUN Working Group criteria
- Describe the clinical features of anterior uveitis (iridocyclitis) identifiable at the slit-lamp and on clinical examination
- Distinguish granulomatous from non-granulomatous iridocyclitis based on keratic precipitate morphology and iris nodule patterns
- Construct a differential diagnosis of the acute red eye and identify features that differentiate iridocyclitis from other sight-threatening causes
INSTRUCTIONS
Uveitis accounts for approximately 10–15% of legal blindness in the developed world and is a leading cause of preventable visual impairment in India. The uveal tract's rich vascularity and immune privilege make it exquisitely sensitive to systemic inflammation, infection, and autoimmune processes — and anterior uveitis (iridocyclitis) is the most common and most immediately sight-threatening presentation. Recognising the signs of iridocyclitis amid a busy OPD of red eyes is a core MBBS-level skill: missing it means missing a window to prevent posterior synechiae, secondary glaucoma, cataract, and blindness.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch. 8 — Diseases of the Uveal Tract (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch. 17 — The Uveal Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man presents to the eye casualty with a 2-day history of painful, red left eye and blurred vision. He reports photophobia — covering the eye relieves the pain. His vision in the affected eye is 6/18 (does not improve with pinhole). On inspection you see a brick-red ring of injection around the limbus, and the cornea appears slightly hazy. The pupil on the affected side is small and sluggish. He mentions he has had episodes of low back pain for the past two years. What is the most likely diagnosis, and what are you going to look for when you examine him at the slit-lamp?
WHY THIS MATTERS
Uveitis is not a single diagnosis — it is a syndromic term encompassing inflammation of any part of the uveal tract, with diverse aetiologies ranging from autoimmune (HLA-B27-associated spondyloarthropathy, sarcoidosis) to infectious (TB, herpes viruses, toxoplasma) to idiopathic. As a final-year MBBS student and future doctor, you will encounter red eyes regularly in general practice, medicine, and ophthalmology. The ability to confidently distinguish iridocyclitis from conjunctivitis and from acute angle-closure glaucoma is not an academic exercise — acute glaucoma and uveitis are both red-eye emergencies but require fundamentally different treatments; confusing them can cause permanent blindness. Furthermore, iridocyclitis is often the first sign of a systemic disease (ankylosing spondylitis, sarcoidosis, IBD, TB) that requires concurrent systemic management. Recognising and correctly classifying uveitis saves both vision and may reveal a life-altering systemic diagnosis.
RECALL
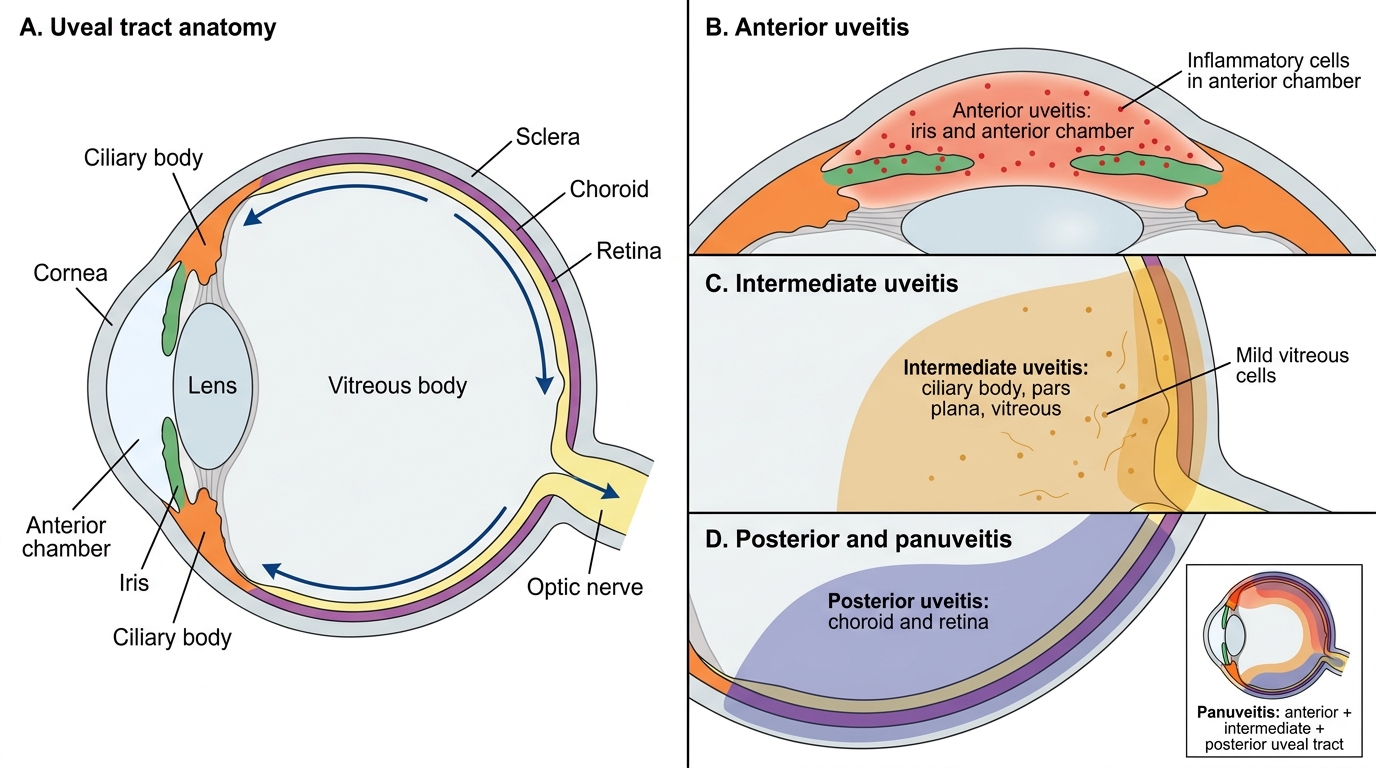
Before diving into uveitis, recall from your Anatomy studies that the uveal tract comprises three continuous layers: the iris anteriorly, the ciliary body in the middle, and the choroid posteriorly. Together these structures form the middle, vascular coat of the eye (between the outer corneoscleral coat and the inner retina). The iris is a thin diaphragm with a central pupillary aperture, controlled by the sphincter pupillae (parasympathetic — constriction) and dilator pupillae (sympathetic — dilation). The ciliary body has two functional parts: the ciliary muscle (responsible for accommodation via the lens zonule) and the ciliary processes (which secrete aqueous humour). The choroid is a dense capillary plexus that provides nutrition to the outer two-thirds of the retina. Recall also the concept of the blood–ocular barrier from Physiology: tight junctions between iris capillary endothelial cells and between ciliary epithelial cells normally prevent large molecules and cells from entering the aqueous or vitreous — when this barrier breaks down in uveitis, protein and inflammatory cells flood into the anterior chamber, producing the characteristic slit-lamp signs you are about to learn.
What Is Uveitis? Anatomical Overview and the SUN Classification
Uveitis is defined as inflammation of the uveal tract — the iris, ciliary body, and/or choroid. The inflammation may be primary (the eye is the principal target) or secondary to systemic disease, infection, trauma, or malignancy (masquerade syndrome). Because the uveal tract is contiguous and vascular, inflammation tends to spread, making anatomical classification both clinically meaningful and practically essential for guiding investigation and treatment. Without a shared classification language, clinicians cannot meaningfully communicate prognosis, compare treatment outcomes, or align systemic investigation with the most likely aetiological diagnoses. Anterior uveitis behaves and responds to treatment very differently from posterior uveitis — lumping them together under a single treatment protocol would cause harm. The uveal tract's anatomical continuity also means that untreated anterior inflammation can propagate posteriorly and vice versa, so the starting site of disease matters both diagnostically and therapeutically.
The internationally accepted framework is the SUN (Standardisation of Uveitis Nomenclature) Working Group classification, which organises uveitis by the primary site of inflammation:
- Anterior uveitis — inflammation primarily in the anterior segment (anterior chamber and/or ciliary body up to the vitreous base). Includes iritis (iris alone), iridocyclitis (iris + ciliary body — the most common form), and anterior cyclitis (ciliary body alone). This is the most frequent anatomical type.
- Intermediate uveitis — primary inflammation in the vitreous, pars plana, and peripheral retina, with no primary anterior segment or posterior pole disease. Also called pars planitis when idiopathic and associated with snowball/snowbank vitreous opacities.
- Posterior uveitis — inflammation posterior to the vitreous base, involving the choroid (choroiditis), retina (retinitis), or both (chorioretinitis, retinochoroiditis). Includes toxoplasma chorioretinitis, CMV retinitis, and serpiginous choroidopathy.
- Panuveitis — inflammation involving all three segments simultaneously, without a single predominant site.
This classification matters because anterior uveitis is managed predominantly with topical agents, intermediate and posterior uveitis usually require systemic or periocular treatment, and the systemic disease associations differ by anatomical site.
Uveal Tract and Anatomical Classification of Uveitis
The Uveal Tract: Anatomy and Why Inflammation Here Is Dangerous
Understanding why uveitis is sight-threatening requires appreciating the unique anatomy and physiology of the uveal tract and its relationship to adjacent ocular structures. The uveal tract is the most vascular tissue in the body per unit volume, and this rich vascularity — while essential for nourishing the avascular lens and the outer retina — also means it is exquisitely susceptible to immune-complex deposition, haematogenous seeding, and autoimmune attack. Blood flow through the choroidal circulation is among the highest of any tissue in the human body, exceeding even the renal cortex on a per-gram basis. This relentless perfusion is a double-edged sword: it sustains the metabolically demanding outer retinal photoreceptors, but it also delivers circulating immune complexes, pathogens, and autoreactive lymphocytes directly to the uveal stroma. The eye's enclosed, rigid compartment means that even modest volumes of inflammatory exudate raise intraocular pressure or distort delicate optical surfaces, translating cellular-level inflammation into clinically measurable visual loss. Appreciating these anatomical vulnerabilities is the foundation for understanding every clinical sign of iridocyclitis.
The blood–ocular barrier is the anatomical basis for ocular immune privilege. Two components are relevant here:
- The blood–aqueous barrier: tight junctions between iris capillary endothelial cells and between non-pigmented ciliary epithelial cells prevent most serum proteins and leucocytes from entering the aqueous humour under normal conditions.
- The blood–retinal barrier: tight junctions between retinal pigment epithelium cells (outer barrier) and between retinal vascular endothelial cells (inner barrier).
When the uveal tract is inflamed, breakdown of the blood–aqueous barrier releases protein into the anterior chamber (producing aqueous flare on slit-lamp) and allows inflammatory cells (predominantly lymphocytes and macrophages in non-granulomatous disease, macrophages and epithelioid cells in granulomatous disease) to flood into the aqueous. These cells settle on the cool corneal endothelium as keratic precipitates (KPs).
Secondary dangers arise from the anatomy:
- The iris lies against the anterior lens surface — inflammatory exudate can glue the posterior iris surface to the lens capsule, forming posterior synechiae.
- The ciliary body produces aqueous humour — inflammation reduces aqueous production (lowering IOP acutely) but inflammatory debris can block the trabecular meshwork (raising IOP chronically).
- The choroid lies adjacent to the retinal pigment epithelium — choroidal inflammation can disrupt the outer retinal barrier and cause exudative retinal detachment or macular oedema.
SELF-CHECK
A student looks at the slit-lamp and sees a 1mm x 1mm beam revealing 20 white cells floating in the anterior chamber. According to the SUN grading system, this is grade:
A. 0.5+ (1–5 cells)
B. 1+ (6–15 cells)
C. 2+ (16–25 cells)
D. 3+ (26–50 cells)
Reveal Answer
Answer: C. 2+ (16–25 cells)
SUN anterior chamber cell grading: 0.5+ = 1–5 cells; 1+ = 6–15 cells; 2+ = 16–25 cells; 3+ = 26–50 cells; 4+ = >50 cells per 1 mm × 1 mm slit-beam field. 20 cells falls in the 2+ (16–25) range.
Recognising Anterior Uveitis (Iridocyclitis): The Clinical Signs
Iridocyclitis — inflammation of the iris and ciliary body together — is the most common form of uveitis encountered in clinical practice. Its recognition depends on a systematic slit-lamp examination supplemented by careful clinical observation before the instrument is even used. Learning each sign with its pathophysiological basis makes the clinical picture memorable and reduces diagnostic error.
1. Ciliary flush (circumcorneal injection): The hallmark of deep ocular inflammation (as opposed to conjunctival disease). It appears as a brick-red to violaceous ring of injection around the limbus, distinct from the bright-red peripheral injection of conjunctivitis. It reflects dilatation of the deep episcleral and limbal vessels — branches of the anterior ciliary arteries that supply the ciliary body. Unlike conjunctival injection, ciliary flush does NOT blanch with topical phenylephrine (a key bedside test).
2. Keratic precipitates (KPs): Inflammatory cells, pigment, and fibrin deposited on the corneal endothelium. They are seen at the slit-lamp as discrete deposits, typically in the inferior triangle of the cornea (Arlt's triangle — gravity-dependent accumulation). KP morphology is diagnostically crucial (see next heading).
3. Aqueous cells and flare: Cells (inflammatory, chiefly lymphocytes) and protein (flare) in the anterior chamber are the direct result of blood–aqueous barrier breakdown. Cells are counted in a 1 mm × 1 mm high-power slit-beam (SUN grading 0 to 4+). Flare is graded by the haziness of the beam as it passes through the aqueous (1+ faint to 4+ fibrinous/plastic aqueous). Fibrinous aqueous in severe iridocyclitis can produce visible strands or a fibrin clot in the anterior chamber.
4. Miosis (small, irregular pupil): Spasm of the sphincter pupillae due to ciliary body inflammation causes miosis. Posterior synechiae (see below) can produce an irregular pupil when synechiae are partial, pulling the pupil margin towards the adhesion sites.
5. Posterior synechiae: Adhesions between the posterior surface of the iris and the anterior capsule of the lens. These develop when inflammatory exudate glues the apposed surfaces. When synechiae are widespread (360°), they occlude the pupil completely — seclusio pupillae — blocking aqueous flow from posterior to anterior chamber, causing iris bombé and secondary angle-closure glaucoma. Posterior synechiae are the most important complication to prevent; this is why cycloplegia is the first treatment.
6. Hypopyon: A sterile (or infective) layered collection of white cells in the inferior anterior chamber — visible as a whitish level. In iridocyclitis, it represents an intense inflammatory response. Although it looks dramatic, a small hypopyon in the context of other iridocyclitis features is a sterile phenomenon distinct from infective endophthalmitis (which produces a much more severe reaction). Hypopyon is distinguished from hyphema (blood) and from infective causes (covered in detail in OP6.3).
7. Reduced IOP (acutely): Ciliary body inflammation reduces aqueous secretion, characteristically lowering IOP below the normal range (10–21 mmHg) in acute iridocyclitis — the opposite of angle-closure glaucoma (where IOP is markedly elevated). This IOP difference is a key differential point.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
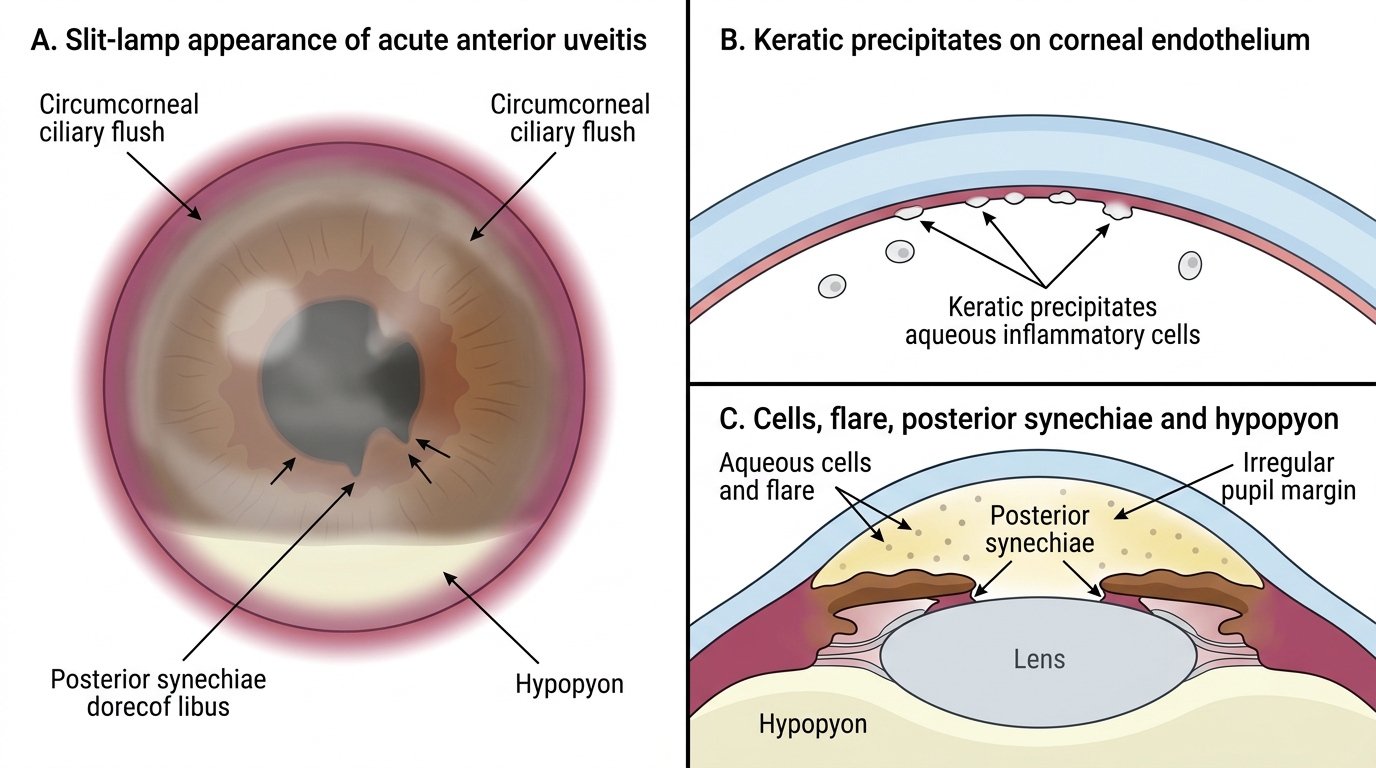
Slit-Lamp Signs of Acute Anterior Uveitis