Page 2 of 18
OP6.1 | Uveitis Classification and Iridocyclitis Recognition — SDL Guide (Part 2)
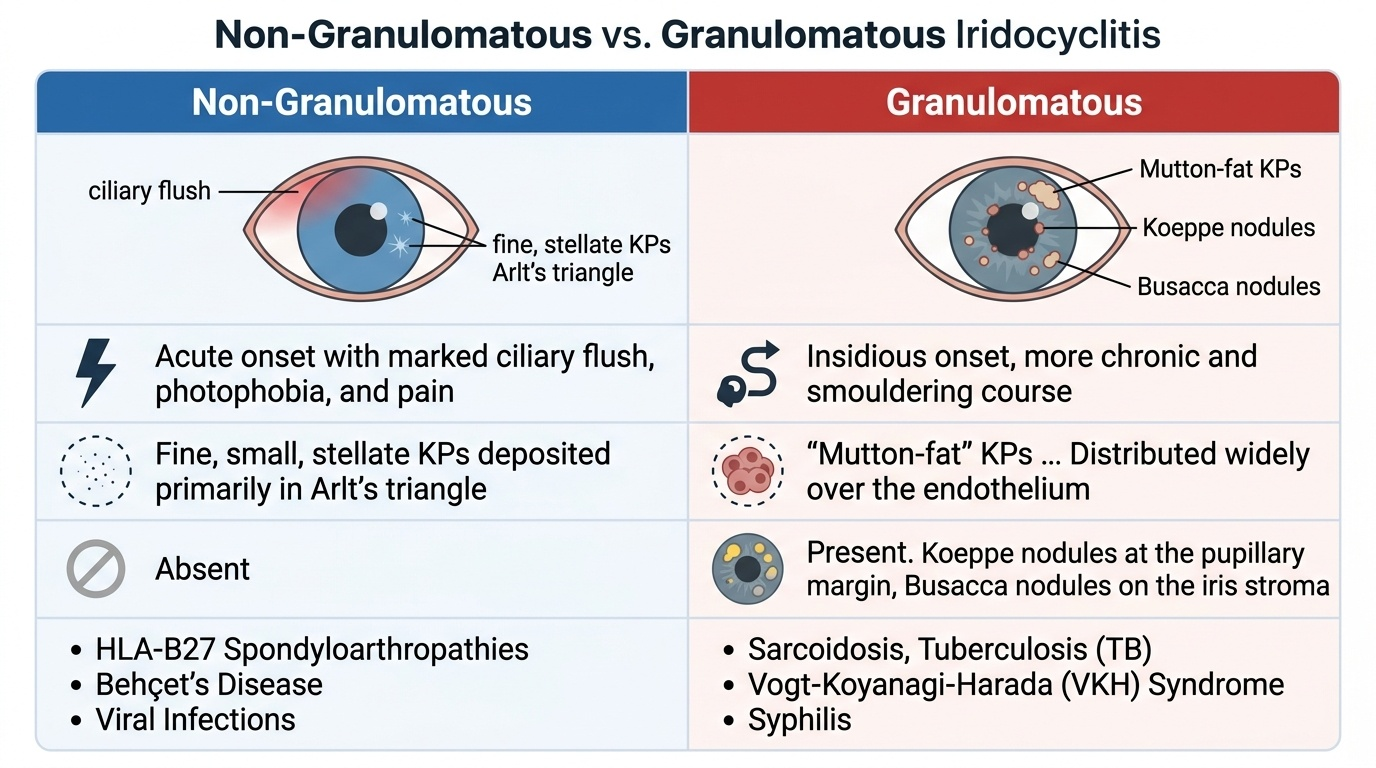
Granulomatous vs Non-Granulomatous Iridocyclitis: How to Distinguish Them
The distinction between granulomatous and non-granulomatous iridocyclitis is not merely histological — it has direct implications for the aetiological workup and systemic disease associations. An ophthalmologist can make this distinction at the slit-lamp on the first visit, before any investigations are done. The KP morphology and the presence or absence of iris nodules are the two slit-lamp features that drive this classification, and getting it right on the first encounter saves time, guides investigation efficiently, and narrows the aetiological differential from many conditions to a short, manageable list. Non-granulomatous disease prompts immediate HLA-B27 testing and a focused rheumatology history; granulomatous disease mandates a systemic workup for sarcoidosis, tuberculosis, and VKH — conditions whose treatment is fundamentally different from simple anti-inflammatory steroid therapy. Misclassifying a granulomatous uveitis as non-granulomatous risks missing a treatable systemic disease and underinvestigating the patient. The morphological distinction is therefore both diagnostically and therapeutically consequential.
Provided image
Non-granulomatous iridocyclitis is the more common type. It is characterised by:
- Fine, small, stellate KPs deposited primarily in Arlt's triangle on the inferior corneal endothelium.
- No iris nodules.
- Acute onset with marked ciliary flush, photophobia, and pain.
- Frequent recurrences (especially in HLA-B27-associated disease) with alternating eyes in many patients.
- Associations: HLA-B27-positive spondyloarthropathies (ankylosing spondylitis, reactive arthritis, psoriatic arthritis, IBD-associated) — the most common identified cause of acute anterior uveitis; also Behçet's disease (with hypopyon); herpes simplex/zoster (may have pigmented KPs and raised IOP from trabecular involvement).
Granulomatous iridocyclitis is characterised by:
- Mutton-fat KPs: large, greasy, grey-white KPs composed of epithelioid macrophages and giant cells, distributed over a wider area of the corneal endothelium.
- Iris nodules in two locations:
- Koeppe nodules: at the pupillary margin (pupillary ruff area).
- Busacca nodules: on the anterior iris stroma surface (away from the pupillary margin).
- Insidious onset, more chronic and smouldering course.
- Associations: sarcoidosis (bilateral, chronic, with posterior involvement), tuberculosis (classically unilateral, chronic; anterior or posterior), Vogt-Koyanagi-Harada (VKH) syndrome (bilateral, with choroidal involvement, systemic features), leprosy, sympathetic ophthalmia.
- Fuchs heterochromic iridocyclitis: a special category — fine stellate KPs distributed evenly across the whole endothelium (not inferior triangle), characteristic iris heterochromia (the affected eye is lighter), NO posterior synechiae despite chronic low-grade inflammation, complicated cataract is the main complication.
SELF-CHECK
A 35-year-old woman presents with chronic bilateral red eyes. Slit-lamp shows large, greasy grey-white KPs distributed broadly on the endothelium, and nodules seen at the pupillary margin. The most likely type of uveitis is:
A. Non-granulomatous anterior uveitis
B. Granulomatous anterior uveitis
C. Intermediate uveitis
D. Fuchs heterochromic iridocyclitis
Reveal Answer
Answer: B. Granulomatous anterior uveitis
Large 'mutton-fat' KPs and nodules at the pupillary margin (Koeppe nodules) are the hallmarks of granulomatous iridocyclitis. Non-granulomatous disease has fine stellate KPs and no iris nodules. Intermediate uveitis has vitreous involvement without primary anterior segment signs. Fuchs heterochromic iridocyclitis has fine, evenly distributed KPs across the whole endothelium and no posterior synechiae.
Differential Diagnosis of the Acute Red Eye: Ruling Out Other Dangerous Causes
The acute red eye is a common emergency presentation with several sight-threatening causes. A structured approach using five clinical parameters — pain, vision, pupil, corneal clarity, and IOP — allows rapid differentiation.
Anterior uveitis (iridocyclitis): moderate-to-severe deep aching pain, photophobia (periorbital/brow pain from ciliary spasm), vision reduced (6/18 to 6/36 in moderate cases), pupil miotic and irregular (posterior synechiae), cornea may show hazy endothelium with KPs, IOP low or normal, ciliary flush prominent, NO purulent discharge.
Acute angle-closure glaucoma (AACG): severe acute pain, markedly reduced vision (often counting fingers or worse), pupil mid-dilated and fixed (oval or vertically oval), corneal oedema (steamy/hazy cornea), very HIGH IOP (typically >40 mmHg), circumcorneal injection present, coloured halos around lights. This is the most dangerous mimic — a missed angle-closure may result in blindness within hours. The IOP and mid-dilated fixed pupil are the key differentiators.
Infective keratitis (corneal ulcer): pain, photophobia, reduced vision, circumcorneal injection, but the hallmark is a visible corneal ulcer/infiltrate — white opacity on the cornea with fluorescein staining. Purulent discharge may be present (bacterial). A dendritic ulcer (HSV) stains green with fluorescein. The corneal lesion and specific ulcer morphology identify keratitis.
Scleritis: severe, boring, deep pain often radiating to the jaw and temple (worse at night), photophobia, reduced vision if posterior scleritis; dark red/bluish injection of the scleral vessels; scleral tenderness; does NOT blanch with phenylephrine; often associated with systemic rheumatological disease (RA, granulomatosis with polyangiitis).
Conjunctivitis: bright red, diffuse conjunctival injection (not circumcorneal), discharge (bacterial = purulent, viral = watery, allergic = stringy/mucoid), NO photophobia, NO pain (only grittiness/discomfort), vision NORMAL, pupil NORMAL, IOP NORMAL. Conjunctivitis does not threaten sight — distinguishing it from the dangerous causes above is the key clinical skill.
| Feature | Iridocyclitis | Acute Glaucoma | Keratitis | Conjunctivitis |
|---|---|---|---|---|
| Pain | Moderate, photophobic | Severe, acute | Moderate-severe | Mild grittiness |
| Vision | Reduced | Markedly reduced | Reduced | Normal |
| Pupil | Miotic, irregular | Mid-dilated, fixed | Normal | Normal |
| Cornea | KPs, slight haze | Steamy oedema | Ulcer/infiltrate | Clear |
| IOP | Low/normal | Very high (>40) | Normal | Normal |
| Discharge | None | None | ± purulent | Prominent |
CLINICAL PEARL
The mnemonic CAMP helps remember iridocyclitis signs: Ciliary flush, Aqueous cells and flare, Miosis (miotic pupil), Posterior synechiae (and KPs). The IOP is characteristically LOW in acute anterior uveitis — the opposite of angle-closure glaucoma. When you see a red eye with photophobia, a miotic irregular pupil, and NO discharge, the diagnosis is iridocyclitis until proved otherwise. In a patient with known HLA-B27-related disease (e.g. ankylosing spondylitis), any red eye should be referred urgently to ophthalmology — even if mild — because recurrent acute iridocyclitis is highly associated with spondyloarthropathies and the window for treatment to prevent synechiae is narrow.
First-Line Management Principles of Iridocyclitis
The immediate management of iridocyclitis follows two parallel goals that should begin as soon as the diagnosis is established, before the results of any investigation are available: suppress inflammation and prevent synechiae. These are not contradictory — they are complementary.
1. Cycloplegia (mydriatics): The first, most urgent step. Atropine 1% eye drops or homatropine 2% are given to keep the pupil dilated and the ciliary body in spasm-free state. Cycloplegia achieves two things: it prevents the posterior iris from resting on the lens (thus blocking posterior synechiae formation), and it relieves ciliary spasm, reducing pain. In a patient with posterior synechiae already forming (irregular pupil), intensive mydriatics with alternating instillation of atropine and phenylephrine (the 'Traquair's cocktail') are used to break nascent synechiae before they organise.
2. Topical corticosteroids: Prednisolone acetate 1% or dexamethasone 0.1% eye drops are the cornerstone of anti-inflammatory treatment. They are given frequently (up to hourly in severe cases) and tapered as inflammation resolves. Topical steroids suppress the blood–aqueous barrier breakdown, reduce cellular infiltrate, and lower the risk of complications. Detailed pharmacology, indications for systemic steroids, and treatment of specific aetiologies are covered in OP6.2 (Iridocyclitis Complications, Investigations and Treatment).
3. Analgesia and dark glasses: Systemic NSAIDs or paracetamol for pain; dark glasses to reduce photophobia from ciliary spasm and pupillary light reflex.
The key management principle at this stage is: never delay cycloplegia waiting for investigations — posterior synechiae can form within 24–48 hours of onset and are irreversible once organised.
SELF-CHECK
Why is atropine (a cycloplegic) given as the FIRST treatment in acute iridocyclitis, before starting topical steroids?
A. To lower intraocular pressure
B. To prevent posterior synechiae by keeping the posterior iris away from the lens
C. To dilate pupil for fundus examination
D. To reduce corneal oedema
Reveal Answer
Answer: B. To prevent posterior synechiae by keeping the posterior iris away from the lens
Cycloplegia (atropine) prevents posterior synechiae by dilating the pupil and pulling the posterior iris surface away from the anterior lens capsule. Posterior synechiae can form within hours and are irreversible once organised — hence this is the most urgent first step. Steroids suppress inflammation but do not prevent mechanical adhesion. The other options are not the primary rationale for cycloplegia in iridocyclitis.
Self-Assessment: Identifying and Classifying Uveitis
Test your understanding of uveitis classification and iridocyclitis recognition with the following clinical scenarios. After working through each, review your reasoning against the explanation provided. The key skills being assessed are: (1) applying SUN anatomical classification to a clinical description; (2) identifying granulomatous vs non-granulomatous features; (3) differentiating iridocyclitis from other red-eye emergencies using IOP, pupil shape, and corneal signs; and (4) identifying the urgency of cycloplegia in acute anterior uveitis. Strong performance here means you can not only name the correct diagnosis but articulate the mechanistic chain that links each clinical sign to its anatomical cause.
Remember: in the exam and in clinical practice, you will be expected to not just name the diagnosis but justify it — which signs support which classification, and what pathophysiological mechanism underlies each sign. Work through the micro-quiz questions before reading the explanations.