Page 4 of 20
OP7.2 | Primary Open Angle Glaucoma — SDL Guide
Learning Objectives
- Describe the etiopathogenesis of primary open-angle glaucoma (POAG) including the role of trabecular outflow resistance and intraocular pressure
- Explain why POAG causes painless, gradual peripheral visual field loss and often presents late
- Outline the clinical investigations: Goldmann tonometry, gonioscopy, optic disc assessment (C:D ratio, neuroretinal rim), and perimetry
- Distinguish POAG from normal-tension glaucoma, ocular hypertension, PACG, and pseudoexfoliation glaucoma
- List the drug classes used in POAG management, identify prostaglandin analogues as first-line, and state their mechanism
- Describe when laser trabeculoplasty and trabeculectomy are indicated
INSTRUCTIONS
Primary open-angle glaucoma is the leading cause of irreversible blindness worldwide after cataract, and its silent nature — painless, slowly progressive peripheral field loss — means patients often present when significant optic nerve damage has already occurred. This module follows the OP arc (presentation → pathophysiology → examination → diagnosis → management → self-assessment) to build both the conceptual and clinical framework needed for a final-year MBBS student. Pay particular attention to the CRITICAL contrast with primary angle-closure glaucoma: same end-result (optic nerve damage and blindness) but opposite mechanism, angle finding, and management — confusing the two is a dangerous error.
References
- AK Khurana — Comprehensive Ophthalmology, 7th edition, Chapter: Glaucoma (textbook)
- Parsons' Diseases of the Eye, 23rd edition, Chapter: Glaucoma (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old retired schoolteacher presents to the eye OPD for a routine refraction. He has no complaints — his vision for reading is slightly blurred but he attributes this to 'age'. Fundus examination by the resident reveals a cup:disc ratio of 0.8 bilaterally (the fellow eye is 0.75), with marked inferior neuroretinal rim thinning and disc pallor. IOP on Goldmann tonometry is 26 mmHg in both eyes. Visual field testing with automated perimetry shows a dense arcuate scotoma in the superior field of the right eye and an early nasal step in the left. He is shocked — he thought his vision was fine. 'How can I have glaucoma if I have no pain and can see clearly?' he asks. How would you explain what has happened to his visual system over the past decade, without his awareness?
WHY THIS MATTERS
Primary open-angle glaucoma (POAG) is the commonest form of glaucoma worldwide, accounting for approximately 74% of all glaucoma cases. It is estimated that over 60 million people globally have glaucoma, with POAG responsible for the majority. In India, POAG is the leading cause of irreversible blindness in adults over 40, ahead of primary angle-closure glaucoma (which has a higher acute impact per episode but lower prevalence). The challenge is epidemiological as much as clinical: because POAG causes no pain, no redness, and no visual symptoms until the disease is advanced, more than 50% of patients are undiagnosed in high-income countries and up to 90% in low-income settings. By the time central vision is threatened, the optic nerve has already lost over 90% of its retinal ganglion cell axons. The MBBS graduate must be equipped not only to diagnose and manage POAG in the clinic, but to counsel patients about the importance of regular screening (especially those with a family history or elevated IOP) — because the only intervention that works is early detection and IOP reduction before irreversible damage accumulates.
RECALL
Before examining POAG in detail, recall the fundamentals of aqueous humour drainage and intraocular pressure regulation from your Year 1 physiology. Aqueous humour is produced continuously by the ciliary body and flows from the posterior chamber through the pupil into the anterior chamber. Approximately 85–90% drains via the conventional (trabecular) route: through the trabecular meshwork at the iridocorneal angle → Schlemm's canal → aqueous veins → episcleral venous system. The remaining 10–15% drains via the uveoscleral (unconventional) route: across the ciliary body and supraciliary space → sclera. Normal intraocular pressure (IOP) is 10–21 mmHg (measured by Goldmann applanation tonometry) and represents the equilibrium between aqueous production and outflow. Also recall the anatomy of the optic disc: the central cup (physiological excavation) surrounded by the neuroretinal rim (containing retinal ganglion cell axons). The cup:disc (C:D) ratio expresses cup width as a proportion of disc width; a C:D ratio ≤0.4 is normal in most adults. Glaucomatous optic neuropathy involves progressive loss of the neuroretinal rim and expansion of the cup.
The Silent Thief: How POAG Presents
The defining clinical characteristic of primary open-angle glaucoma is its silence. Unlike primary angle-closure glaucoma (PACG), which presents dramatically with severe ocular pain, redness, haloes, and nausea, POAG causes no symptoms until the disease is advanced. This is because the retinal ganglion cell (RGC) loss in POAG is predominantly peripheral — affecting the far temporal and nasal visual fields first — while central (macular) vision is preserved until late in the disease. The brain also 'fills in' mild peripheral scotomas through a process of cortical adaptation, so patients remain symptom-free even as significant damage accumulates.
When patients do present symptomatically, the complaints are characteristically vague: 'my glasses need changing' (in reality, the refractive change is minimal; the visual difficulty is from field loss), 'I'm bumping into things' (late nasal field loss causing navigation difficulty), or simply a complaint of visual blurring noticed on routine examination. In a small proportion, monocular field loss is noticed when the fellow eye is accidentally occluded.
Risk factors for POAG:
- Age: prevalence increases sharply after 40 years; over 65 years, prevalence exceeds 5%
- Elevated IOP (ocular hypertension): a major modifiable risk factor — but NOT diagnostic of POAG alone
- Family history: first-degree relatives of POAG patients have a 4-fold increased risk (autosomal dominant tendency with variable penetrance)
- Race: Black African populations have a 3–4× higher prevalence and more severe disease at presentation than White European populations
- Myopia (high degree): associated with larger optic discs and thin lamina cribrosa, increasing susceptibility
- Thin central corneal thickness (CCT): CCT <555 µm is an independent risk factor for glaucoma development (also causes underestimation of IOP by applanation tonometry)
- Diabetes mellitus and systemic hypertension: associated with increased risk
- Normal-tension glaucoma (NTG): a variant of POAG where IOP is consistently ≤21 mmHg but the optic nerve shows typical glaucomatous damage — more common in East Asian populations and may involve vascular dysregulation at the optic nerve head
Pathophysiology: Why the Nerve Dies Silently
The pathophysiology of POAG centres on a progressive increase in resistance to aqueous outflow through the trabecular meshwork, despite the iridocorneal angle remaining anatomically open on gonioscopy — which is the defining structural feature that distinguishes POAG from angle-closure glaucoma. The mechanisms underlying this increased trabecular resistance are incompletely understood but include: accumulation of extracellular matrix material within the trabecular meshwork beams, loss of trabecular endothelial cells, and dysfunction of the juxtacanalicular tissue adjacent to Schlemm's canal. The result is a progressive rise in IOP, which in turn exerts mechanical and vascular stress on the optic nerve head.
At the optic nerve head, two broad mechanisms converge to kill retinal ganglion cell (RGC) axons:
1. Mechanical compression: The elevated IOP bows the lamina cribrosa (a perforated scleral plate through which RGC axons exit the eye), compressing and distorting the axonal transport pathways. This starves RGC cell bodies in the retina of neurotrophic factors (particularly brain-derived neurotrophic factor, BDNF) arriving from the lateral geniculate body, triggering apoptosis.
2. Vascular ischaemia: Elevated IOP reduces ocular perfusion pressure (= mean arterial pressure − IOP). In vulnerable optic nerves (NTG, systemic hypotension, nocturnal dip in blood pressure), ischaemia of the optic nerve head from reduced blood supply contributes independently to RGC death. This explains why NTG occurs without elevated IOP — the primary insult is vascular.
The consequence of RGC death is progressive loss of their axons in the retinal nerve fibre layer (RNFL), most prominently in the superior and inferior arcuate bundles (which serve the nasal visual field). RNFL thinning precedes visible field defects by years, which is why OCT of the RNFL is now a cornerstone of early detection.
IMPORTANT CONTRAST (the glaucoma trap): POAG = OPEN angle on gonioscopy, gradual painless field loss, trabecular outflow resistance. PACG = CLOSED/narrow/occludable angle, acute painful red eye with haloes, pupil block mechanism. Their management is fundamentally different — prostaglandin analogues are first-line in POAG; pilocarpine (a miotic) is emergency treatment in PACG acute angle-closure. Never apply PACG management principles to POAG.
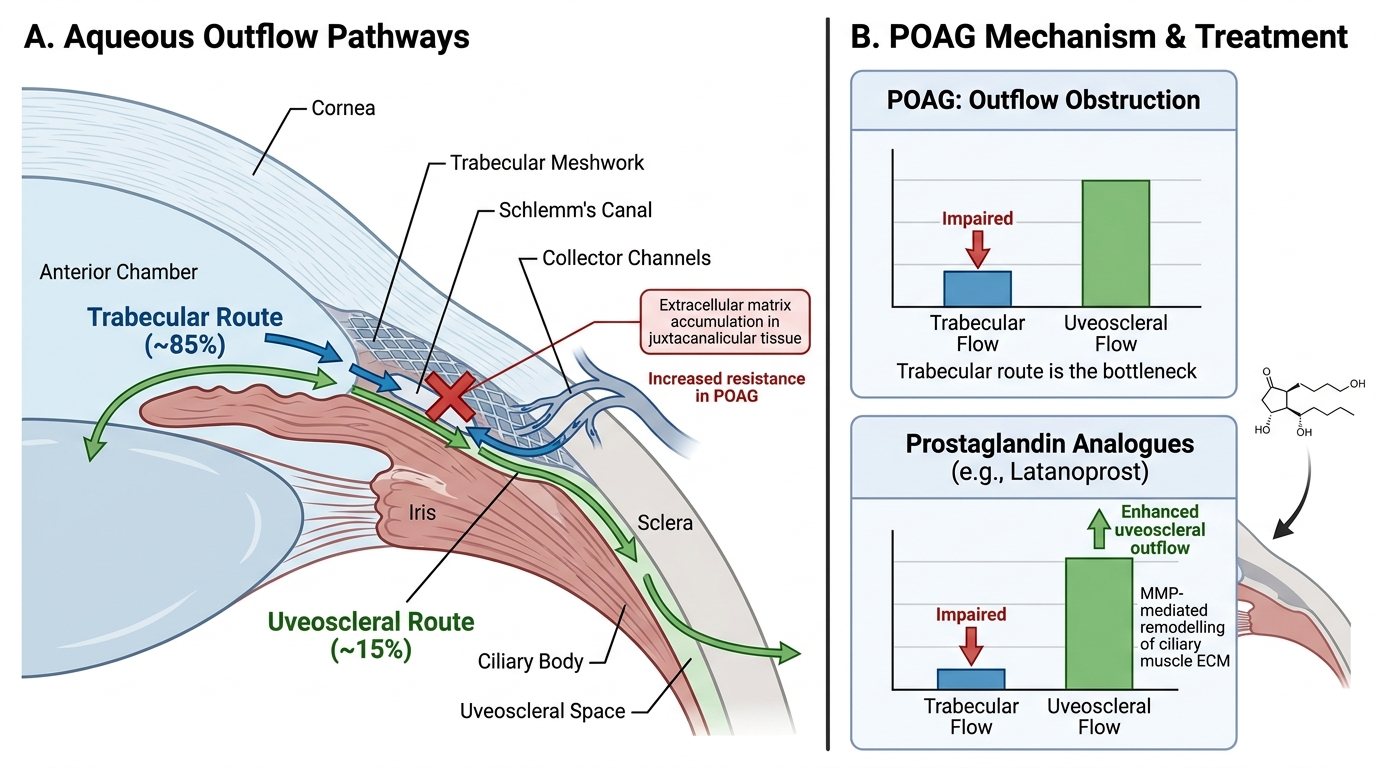
Aqueous Humour Outflow Pathways, POAG Resistance Site, and Prostaglandin Analogue Mechanism
Investigating POAG: IOP, Disc, and Fields
The diagnosis of POAG requires a triad of findings: characteristic glaucomatous optic nerve damage, corresponding visual field defects, and an open iridocorneal angle on gonioscopy. No single test is diagnostic; POAG is a clinical diagnosis based on the convergence of multiple investigations.
1. Intraocular Pressure (IOP) Measurement:
The gold standard is Goldmann applanation tonometry (GAT), which measures the force required to flatten a fixed area (3.06 mm diameter) of the corneal surface. Normal IOP is 10–21 mmHg (population-based ±2 SD). Critical caveat: IOP measurement by GAT is influenced by central corneal thickness (CCT); thin corneas (<555 µm) underestimate true IOP, thick corneas overestimate it. This is clinically significant — a patient with thin CCT and 'borderline' IOP of 21 mmHg may have truly higher pressure than measured.
2. Gonioscopy (CRITICAL for POAG diagnosis):
Gonioscopy uses a goniolens to visualise the iridocorneal angle. In POAG, the angle is OPEN — the trabecular meshwork, scleral spur, and ciliary band are all visible. This finding DEFINES POAG as distinct from PACG (where the angle is closed/narrow/iridotrabecular contact present). Gonioscopy must be performed on every patient with suspected glaucoma — it determines the TYPE of glaucoma and hence the treatment approach.
3. Optic Disc Assessment:
The optic disc is examined at the slit lamp with a +78D or +90D non-contact lens, or by direct ophthalmoscopy. Key glaucomatous disc changes:
- Increased cup:disc (C:D) ratio: C:D >0.6 is suspicious; asymmetry >0.2 between fellow eyes is highly suspicious
- Neuroretinal rim thinning or notching: the ISNT rule (normal rim is thickest Inferiorly > Superiorly > Nasally > Temporally); POAG characteristically thins the inferior then superior rim first
- Bayoneting of vessels: vessels appear to disappear into the cup and re-emerge (due to deep cupping)
- Splinter haemorrhages at the disc margin (Drance haemorrhages): highly specific for glaucoma progression
- Pale disc (not all disc pallor = glaucoma; ischaemic optic neuropathy or compressive lesions also cause pallor)
4. Visual Field Testing (Perimetry):
Automated static perimetry (Humphrey Field Analyser, 30-2 programme) tests the central 30 degrees. Classic POAG visual field defects correspond to superior and inferior arcuate RGC bundle damage:
- Arcuate scotoma (Bjerrum scotoma): a curved field defect following the arcuate RNFL bundle, arching from the blind spot to the nasal horizontal raphe
- Nasal step: a step defect at the nasal horizontal midline
- Paracentral scotoma: early small defect within 10 degrees of fixation
- Tubular (gun-barrel) vision: a late-stage finding when only the central field survives
5. OCT of the RNFL and Optic Disc:
Optical coherence tomography (OCT) quantifies RNFL thickness in all quadrants and measures optic disc parameters objectively. RNFL thinning (especially inferotemporal and superotemporal sectors) precedes visual field defects by an estimated 4–6 years — making OCT the most sensitive tool for early detection.
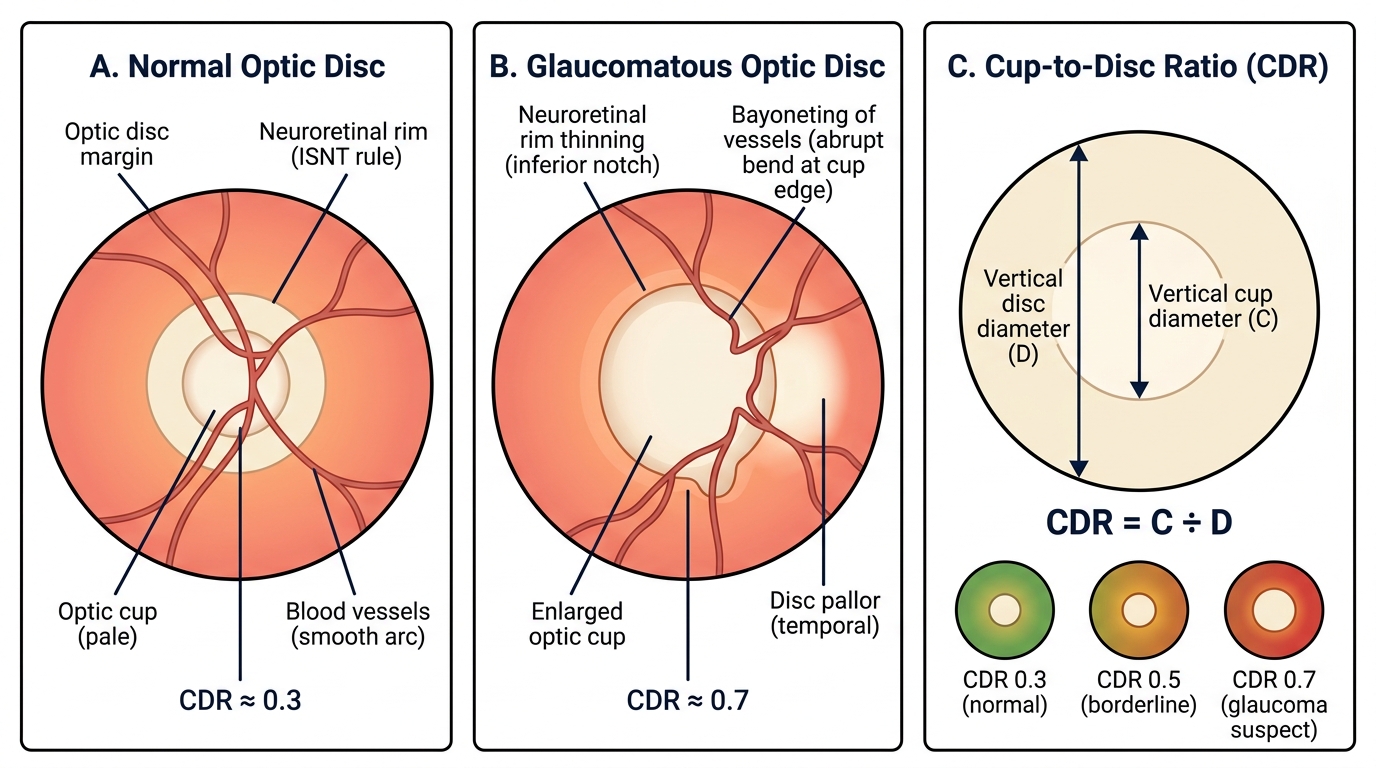
Normal vs. Glaucomatous Optic Disc — Features and Cup-to-Disc Ratio
SELF-CHECK
A 55-year-old man is found to have IOP of 24 mmHg, cup:disc ratio of 0.7 bilaterally, and a superior arcuate scotoma on automated perimetry. Gonioscopy shows an open angle. Central corneal thickness is 540 µm. What is the most likely diagnosis?
A. Ocular hypertension (no disc or field changes)
B. Primary open-angle glaucoma (POAG)
C. Primary angle-closure glaucoma (PACG)
D. Normal-tension glaucoma (NTG)
Reveal Answer
Answer: B. Primary open-angle glaucoma (POAG)
POAG is diagnosed by the triad of characteristic optic nerve damage (C:D 0.7 with neuroretinal rim changes), corresponding visual field defect (superior arcuate scotoma), and OPEN angle on gonioscopy — with elevated IOP (24 mmHg, true IOP may be higher given thin CCT 540 µm). Ocular hypertension has raised IOP but no disc or field changes. PACG has a closed/narrow angle. NTG has IOP consistently ≤21 mmHg.