Page 5 of 20
OP7.2 | Primary Open Angle Glaucoma — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The differential diagnosis of POAG encompasses several conditions that can mimic its disc or field findings, and the precise diagnosis drives fundamentally different management. The most critical distinction — and the most dangerous to confuse — is between POAG and PACG; both cause optic nerve damage and visual field loss, but their mechanisms, angle findings, and treatments are opposite in every clinically meaningful way. POAG has an open iridocorneal angle on gonioscopy with a gradual, painless course and is treated with prostaglandin analogues as first-line therapy; PACG has a closed or occludable angle, can present as an acute emergency with severe pain and haloes, and requires pilocarpine acutely and laser peripheral iridotomy definitively. Confusing the two and administering a prostaglandin analogue to an acute angle-closure attack — rather than pilocarpine plus mannitol — is a dangerous clinical error that delays angle opening and allows ongoing optic nerve ischaemia. A second important differential is normal-tension glaucoma (NTG), which shares all of POAG's disc and field features but has IOP consistently within the normal range (≤21 mmHg), implying that vascular factors at the optic nerve head are as important as mechanical IOP-related injury. Before diagnosing NTG, a compressive lesion of the optic nerve or optic chiasm must be excluded with MRI of the brain and orbits.
| Condition | IOP | Angle (gonioscopy) | Optic disc | Visual fields | Key distinguishing feature |
|---|---|---|---|---|---|
| POAG | >21 mmHg (or NTG ≤21) | Open | Cupped, rim thinning | Arcuate scotoma, nasal step | Gradual, painless; no redness |
| Normal-tension glaucoma (NTG) | ≤21 mmHg (consistently) | Open | Cupped (may be more disc haemorrhages) | Same as POAG | IOP 'normal'; vascular risk factors; more common in East Asians |
| Ocular hypertension (OHT) | >21 mmHg | Open | Normal C:D, no rim damage | Normal | Raised IOP but NO glaucomatous disc or field changes — requires monitoring |
| PACG | High during attack; may be normal between attacks | Closed/narrow (occludable) | Cupped (after repeated attacks) | Field loss | Acute red eye, pain, haloes; angle CLOSED — critical contrast |
| Pseudoexfoliation glaucoma | Often markedly elevated | Open (PXF material on angle) | Cupped | Arcuate | White PXF material on lens/pupil margin; worst IOP fluctuation of any open-angle glaucoma |
| Pigmentary glaucoma | May be elevated (exercise-induced spikes) | Open (dense pigment on TM) | Cupped | Arcuate | Young myopic males; Krukenberg spindle on cornea; reverse pupil block |
Key differential points to memorise:
- If the angle is open → POAG or its variants (NTG, OHT, secondary open-angle)
- If the angle is closed/narrow → PACG
- If there is white flocculent material on the pupil margin and anterior lens surface → pseudoexfoliation (PXF glaucoma — commonest secondary open-angle glaucoma; higher IOP fluctuation; harder to control)
- NTG vs POAG: identical except IOP ≤21 mmHg in NTG; vascular risk factors (nocturnal hypotension, Raynaud's, migraine) more prominent; exclude compressive optic neuropathy (MRI brain/orbit) before diagnosing NTG
CLINICAL PEARL
The ISNT rule is a quick bedside disc assessment tool: in a NORMAL optic disc, the neuroretinal rim is thickest Inferiorly, then Superiorly, then Nasally, then Temporally (ISNT). Glaucoma preferentially damages the inferior then superior rim first, violating the ISNT rule — especially thinning or notching of the inferior rim. A disc that violates ISNT should be treated with high suspicion for glaucoma, even before formal perimetry is available. Also remember: a C:D ratio is only meaningful in the context of disc size. Large discs have physiologically larger cups — a C:D of 0.7 in a large disc may be normal, whereas a C:D of 0.5 in a very small disc may indicate significant loss. Disc size is assessed by the diameter of the light reflex during ophthalmoscopy.
Management: Stepwise IOP Reduction
The only proven, evidence-based treatment for POAG is reduction of intraocular pressure (IOP). Every 1 mmHg reduction in IOP reduces the risk of glaucoma progression by approximately 10% over 5 years (data from EMGT and other trials). The target IOP is individualised — typically 20–30% below the presenting IOP for early disease, and lower (≤12–14 mmHg) for advanced disease or NTG.
Provided image
Treatment follows a stepwise approach:
Step 1 — First-line topical therapy:
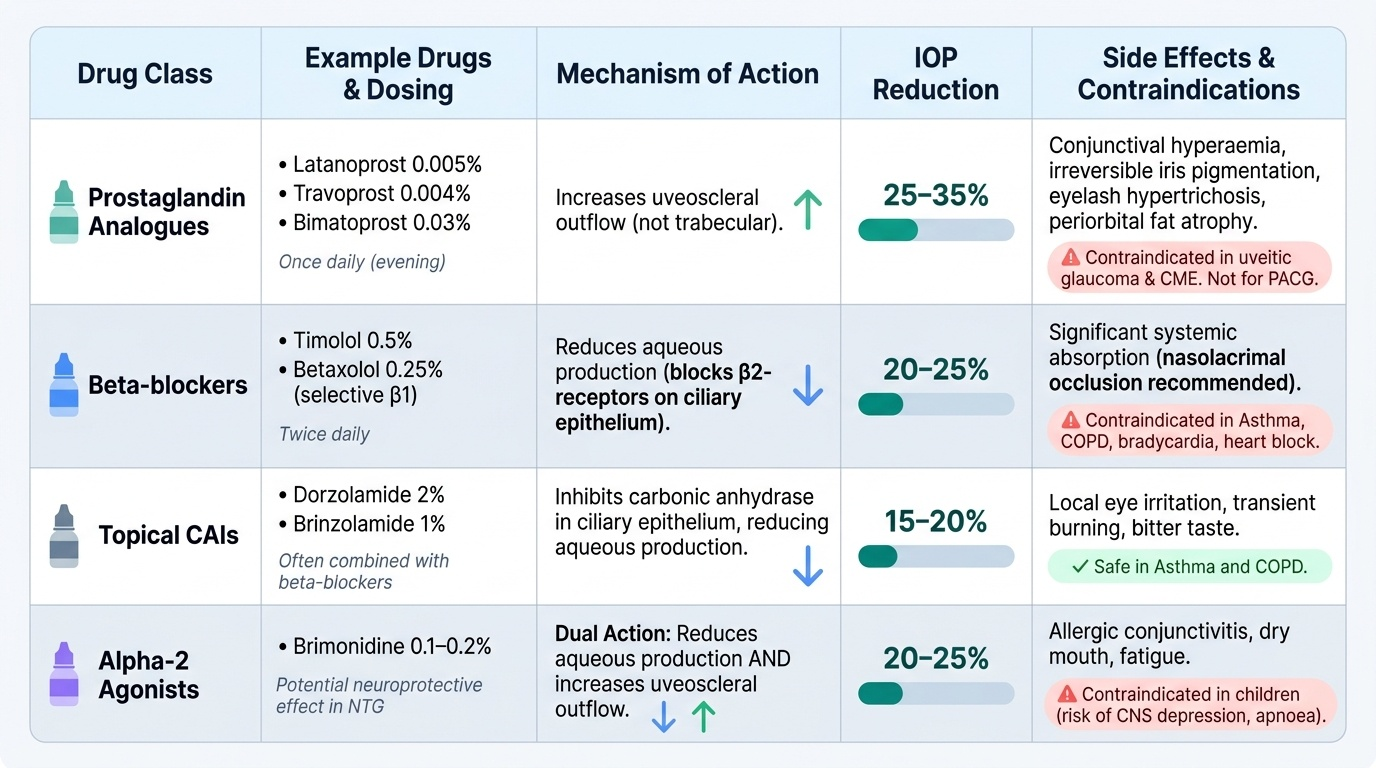
Prostaglandin analogues (latanoprost 0.005%, travoprost 0.004%, bimatoprost 0.03%) are the preferred first-line agents in current guidelines (Asia-Pacific Glaucoma Guidelines, EGS Guidelines). They lower IOP by 25–35% — the highest efficacy of any single agent. Mechanism: increase uveoscleral outflow (not trabecular). Administered ONCE daily (evening). Side effects: conjunctival hyperaemia, increased iris pigmentation (irreversible in hazel eyes), eyelash hypertrichosis (increased length/thickness), periorbital fat atrophy, prostaglandin-associated periorbitopathy. Relatively contraindicated in uveitic glaucoma and cystoid macular oedema. These are NOT appropriate for angle-closure contexts (PACG) as a definitive treatment.
Step 2 — Second-line / adjunct agents:
- Beta-blockers (timolol 0.5%, betaxolol 0.25%): Reduce aqueous production by blocking β2-receptors on ciliary epithelium; lower IOP by 20–25%. Applied twice daily. Contraindications: bronchial asthma, COPD, bradycardia, heart block, myasthenia gravis. Betaxolol (selective β1-blocker) has less bronchospasm risk. Systemic absorption is significant — nasolacrimal occlusion after instillation reduces it.
- Topical carbonic anhydrase inhibitors (CAIs) (dorzolamide 2%, brinzolamide 1%): Inhibit carbonic anhydrase in ciliary epithelium, reducing aqueous production; lower IOP by 15–20%. Safe in asthma/COPD. Combined with beta-blockers (Cosopt = timolol + dorzolamide).
- Alpha-2 agonists (brimonidine 0.1–0.2%): Reduce aqueous production and increase uveoscleral outflow; lower IOP by 20–25%. Avoid in children (CNS depression — sedation, apnoea risk). Useful in NTG for possible neuroprotective effect.
Step 3 — Systemic CAI:
Oral acetazolamide (250 mg QID or SR 500 mg BD) is reserved for acute IOP control (acute PACG attack primarily) or pre-operatively when topical therapy is insufficient. Systemic side effects limit long-term use: paraesthesiae (tingling fingers and toes — the commonest complaint), hypokalaemia, urinary frequency, renal stones, aplastic anaemia (rare).
Step 4 — Laser:
Selective laser trabeculoplasty (SLT) uses a 532 nm Nd:YAG laser to selectively target pigmented trabecular meshwork cells, improving trabecular outflow. LiGHT trial (2019) demonstrated SLT as a cost-effective FIRST-LINE alternative to drops in newly diagnosed POAG/OHT — IOP reduction of ~30%, maintained over 3 years, with high treatment-free disease control. SLT is now considered a first-line option, particularly for patients with compliance issues.
Step 5 — Surgical:
Trabeculectomy (guarded filtration surgery) creates a controlled fistula from the anterior chamber to a subconjunctival bleb, bypassing the trabecular meshwork. It achieves the greatest IOP reduction of any intervention. Antimetabolites (mitomycin C or 5-fluorouracil) are applied intraoperatively to prevent bleb scarring. Complications: blebitis, hypotony, cataract formation. Modern alternatives include minimally invasive glaucoma surgery (MIGS) devices (iStent, Hydrus) for mild-moderate disease.
Key management principles:
- Target IOP = 20–30% below baseline for early disease; lower for advanced/NTG
- Prostaglandin analogues = first-line topical therapy (NOT beta-blockers)
- SLT = effective first-line alternative, especially for compliance-challenged patients
- Medical + laser before surgery; surgery reserved for inadequate IOP control
- Lifelong follow-up: POAG is not cured — IOP control is maintained indefinitely
SELF-CHECK
A 58-year-old woman with newly diagnosed POAG (IOP 26 mmHg, open angle, early arcuate scotoma) is started on topical therapy. She has well-controlled asthma. Which of the following is the most appropriate first-line treatment?
A. Timolol 0.5% eye drops twice daily
B. Latanoprost 0.005% eye drops once daily (evening)
C. Oral acetazolamide 250 mg four times daily
D. Pilocarpine 2% eye drops three times daily
Reveal Answer
Answer: B. Latanoprost 0.005% eye drops once daily (evening)
Latanoprost (a prostaglandin analogue) is the first-line topical therapy for POAG — highest IOP-lowering efficacy (25–35%), once-daily dosing, good systemic safety profile. Timolol is contraindicated in asthma (beta-blocker causes bronchospasm). Oral acetazolamide is reserved for acute IOP crises or pre-operative use, not maintenance therapy. Pilocarpine (a miotic) is used in angle-closure glaucoma (PACG), not POAG — it can worsen visual quality and is inappropriate here.
Self-Assessment: Clinical Reasoning in POAG
Having built the clinical framework for POAG from presentation through pathophysiology, investigation, diagnosis, and management, you are now ready to test your integrated reasoning across the key decision points this condition demands in clinical practice.
A 48-year-old man with a family history of glaucoma (his father lost vision from it) attends for a routine eye check. His IOP is 23 mmHg bilaterally. Gonioscopy shows an open angle with no angle anomaly. His optic discs show C:D ratios of 0.6 bilaterally with symmetric neuroretinal rims and no notching. OCT RNFL is within normal limits. Automated perimetry is normal. How should you manage him? This is ocular hypertension (OHT) — raised IOP with no disc or field evidence of glaucomatous damage. He is not yet POAG. However, his family history and borderline IOP place him at higher risk of conversion. The Ocular Hypertension Treatment Study (OHTS) identified CCT, IOP level, C:D ratio, and field variability as the key conversion risk factors. Measure his central corneal thickness: if thin (<555 µm), his true IOP may be higher than measured and his risk is elevated. Shared decision-making about commencing prophylactic drops versus monitoring is appropriate here.
A 65-year-old woman with known POAG on latanoprost once nightly returns for her 6-month review. Her IOP is 18 mmHg (target 15 mmHg was set given moderate field loss). Her Humphrey field shows a new small paracentral scotoma on pattern deviation. Her RNFL OCT shows 8 µm thinning in the inferotemporal sector compared with 18 months ago. What do you do? This is disease progression despite treatment. She needs intensification: either addition of a second agent (timolol, dorzolamide, or brimonidine), or discussion of SLT, or early referral for trabeculectomy discussion. The clinical skill is recognising progression from serial OCT and field data — not a single test, but a trajectory. Each 1 mmHg further reduction in IOP reduces progression risk by approximately 10% over 5 years.
A 70-year-old with POAG asks: 'Doctor, will I go blind?' The answer depends on disease stage at detection, rate of progression, and adherence to treatment. Early POAG with good IOP control has an excellent prognosis — most patients retain useful central vision throughout their lives. Advanced POAG at presentation carries a higher risk of significant field loss affecting daily activities. Communicating prognosis honestly — separating what is already lost (irreversible) from what remains protectable (with good IOP control) — is a core clinical communication skill in chronic glaucoma care.