Page 16 of 23
OP9.5 | Optic Nerve and Visual Pathway Disorders — SDL Guide
Learning Objectives
- Describe the anatomy of the visual pathway from the retina to the occipital cortex and correlate specific lesion sites with their characteristic visual field defects
- Distinguish papilloedema from optic neuritis and anterior ischaemic optic neuropathy on the basis of clinical features, fundoscopy, and RAPD
- Recognise arteritic AION from giant cell arteritis as a bilateral visual emergency requiring immediate corticosteroid treatment
- Describe the management of optic neuritis (IV methylprednisolone) and its relationship to multiple sclerosis
- Identify the characteristic visual field defect of chiasmal compression (bitemporal hemianopia) and retrochiasmal lesions (homonymous hemianopia)
INSTRUCTIONS
Diseases of the optic nerve and visual pathway produce some of the most diagnostically rich findings in clinical medicine — a precisely mapped visual field defect can localise a lesion anywhere from the optic nerve to the occipital cortex with great precision. This module teaches you the anatomy that makes this localisation possible, the key conditions at each level, and the critical clinical distinctions (especially between papilloedema and optic neuritis, and the arteritic emergency of giant cell arteritis) that determine urgent vs elective management.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Chapters on Optic Nerve and Neuro-ophthalmology (textbook)
- Parsons' Diseases of the Eye, 22nd ed. Chapter on Diseases of the Optic Nerve and Visual Pathway (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman presents with a 3-day history of pain in her right eye when she moves it, and progressive blurring of vision in the same eye. She saw a GP who told her she had 'conjunctivitis' and prescribed antibiotic drops. Two days later she returns to your clinic because the drops have not helped and her vision is now 6/60 in the right eye. RAPD is present in the right eye. Fundoscopy shows a normal-looking fundus with a slightly swollen right disc. ESR is normal. This is acute optic neuritis — and the finding of RAPD with painful eye movement and normal-appearing fundus in a young woman is the opposite of conjunctivitis. The misdiagnosis delayed investigation for multiple sclerosis and appropriate treatment. Understanding this condition, and the ability to test RAPD at the bedside, is what separates this diagnosis from a missed one.
WHY THIS MATTERS
The optic nerve and visual pathway are the conduit between the eye and the brain. Diseases at any point along this 40-cm path — from the nerve fibre layer at the retina to the primary visual cortex in the occipital pole — can cause characteristic patterns of visual loss that, when correctly interpreted, locate the lesion with the precision of a CT scan. Papilloedema tells you the ICP is raised before the patient has a headache. Optic neuritis may be the first clinical presentation of multiple sclerosis — diagnosing it correctly sets in motion the neurology workup that can change the patient's life with early MS disease-modifying therapy. Giant cell arteritis causing anterior ischaemic optic neuropathy is a bilateral ocular emergency. A bitemporal hemianopia on visual field testing leads you directly to a pituitary macroadenoma pressing on the chiasm. As a physician — not just an ophthalmologist — you will be the first clinician to examine these patients, and your ability to test visual fields at the bedside, check RAPD, and look at the disc will determine whether timely action is taken.
RECALL
Recall from anatomy: the optic nerve (CN II) begins at the optic disc, passes through the optic canal in the sphenoid, and meets its fellow at the optic chiasm — just anterior to the pituitary gland. At the chiasm, fibres from the nasal (medial) half of each retina cross to the contralateral optic tract, while temporal (lateral) fibres remain ipsilateral. This partial decussation is the anatomical basis for all the visual field defects you will learn in this module. Beyond the chiasm, the optic tracts pass to the lateral geniculate nuclei (LGN), then as optic radiations through the temporal (inferior fibres = Meyer's loop) and parietal lobes to the primary visual cortex (V1) in the medial occipital lobe. Also recall: the RAPD (relative afferent pupillary defect) tests the afferent limb of the pupillary light reflex — approximately 80% of the optic nerve fibres subserve the pupillary pathway — so any disease reducing the total number of functional optic nerve fibres (unilaterally) produces a detectable RAPD on swinging flashlight test.
Presentation: Visual Field Defects and Disc Changes as the Clinical Clues
Optic nerve and visual pathway diseases present through a limited repertoire of symptoms — visual field loss, visual acuity reduction, disc changes on fundoscopy, and occasionally pain. The pattern of these findings is the clinical key to anatomical localisation.
Visual acuity is affected by lesions involving the central visual pathway (optic nerve, macula, occipital cortex at the calcarine fissure representing the central field). Central scotoma (a blind spot in the centre of vision) is the classic presentation of optic nerve disease, particularly optic neuritis. Peripheral field loss (tunnel vision) suggests widespread retinal disease or glaucoma. Altitudinal field defects (loss of the upper or lower half of vision in one eye) suggest anterior ischaemic optic neuropathy.
Visual field defects that respect the vertical midline (hemianopia) indicate retrochiasmal or chiasmal disease. A bitemporal hemianopia (loss of both temporal fields) is the classic sign of chiasmal compression (most commonly from a pituitary macroadenoma pressing upward from below). A homonymous hemianopia (loss of the same side of the visual field in both eyes) indicates a retrochiasmal lesion — optic tract, LGN, optic radiation, or visual cortex.
Pain is a critical discriminator at the optic nerve level. Optic neuritis characteristically causes pain on eye movement, worsened by lateral and upward gaze — a highly specific symptom that points to inflammation of the optic nerve sheath. Papilloedema and ischaemic optic neuropathy are typically painless in the eye itself (though papilloedema is associated with headache from raised ICP).
On fundoscopy, the disc may appear: (1) swollen (papilloedema, papillitis, AION), (2) pale (optic atrophy), or (3) normal ('retrobulbar' optic neuritis where the inflammation is posterior to the disc, which looks normal but the patient loses vision — 'the patient sees nothing and the doctor sees nothing'). RAPD is present whenever there is asymmetric optic nerve function loss.
Anatomy of the Visual Pathway: The Map That Decodes Field Defects
A thorough understanding of the visual pathway's anatomy converts an abstract visual field defect into a precise anatomical diagnosis. Every clinician should be able to name the lesion site from the field pattern.
The visual pathway can be divided into five levels — each producing a distinct field defect:
Level 1 — Optic nerve (prechiasmal): a lesion here affects only the ipsilateral eye (monocular). A complete optic nerve lesion causes total monocular blindness in that eye; a partial lesion causes a central scotoma (most commonly), an altitudinal defect, or an arcuate field defect. The RAPD is present in the affected eye. Causes: optic neuritis, AION, glaucoma, compression (tumour), toxic optic neuropathy.
Level 2 — Optic chiasm: at the chiasm, the crossing nasal fibres (representing the temporal field of each eye) are the most vulnerable to central inferior compression (e.g. pituitary adenoma growing superiorly). Compression of these crossing fibres produces the characteristic bitemporal hemianopia — loss of both temporal (lateral) fields, one from each eye. The vertical midline is respected.
Level 3 — Optic tract: an optic tract lesion produces a homonymous hemianopia (same side of the visual field lost in both eyes) but with incongruous defects (the two eyes' hemifields do not match exactly in size and shape) because the fibres from the two eyes are not yet fully integrated.
Level 4 — Optic radiation: fibres pass through the temporal lobe (Meyer's loop, inferior fibres representing the superior visual field) and the parietal lobe (superior fibres representing the inferior visual field). A temporal lobe lesion affects Meyer's loop and produces a superior homonymous quadrantanopia ('pie in the sky'). A parietal lobe lesion affects superior fibres and produces an inferior homonymous quadrantanopia ('pie in the floor').
Level 5 — Occipital cortex (V1): lesions here produce a homonymous hemianopia with macular sparing — the central (macular) vision is preserved because the large macular representation at the occipital pole has a dual blood supply (from MCA and PCA collaterals) and is partially redundant. Cortical blindness (bilateral occipital infarction) produces total blindness with preserved pupillary reflexes (the pupillary pathway leaves the optic tract before reaching the cortex).
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
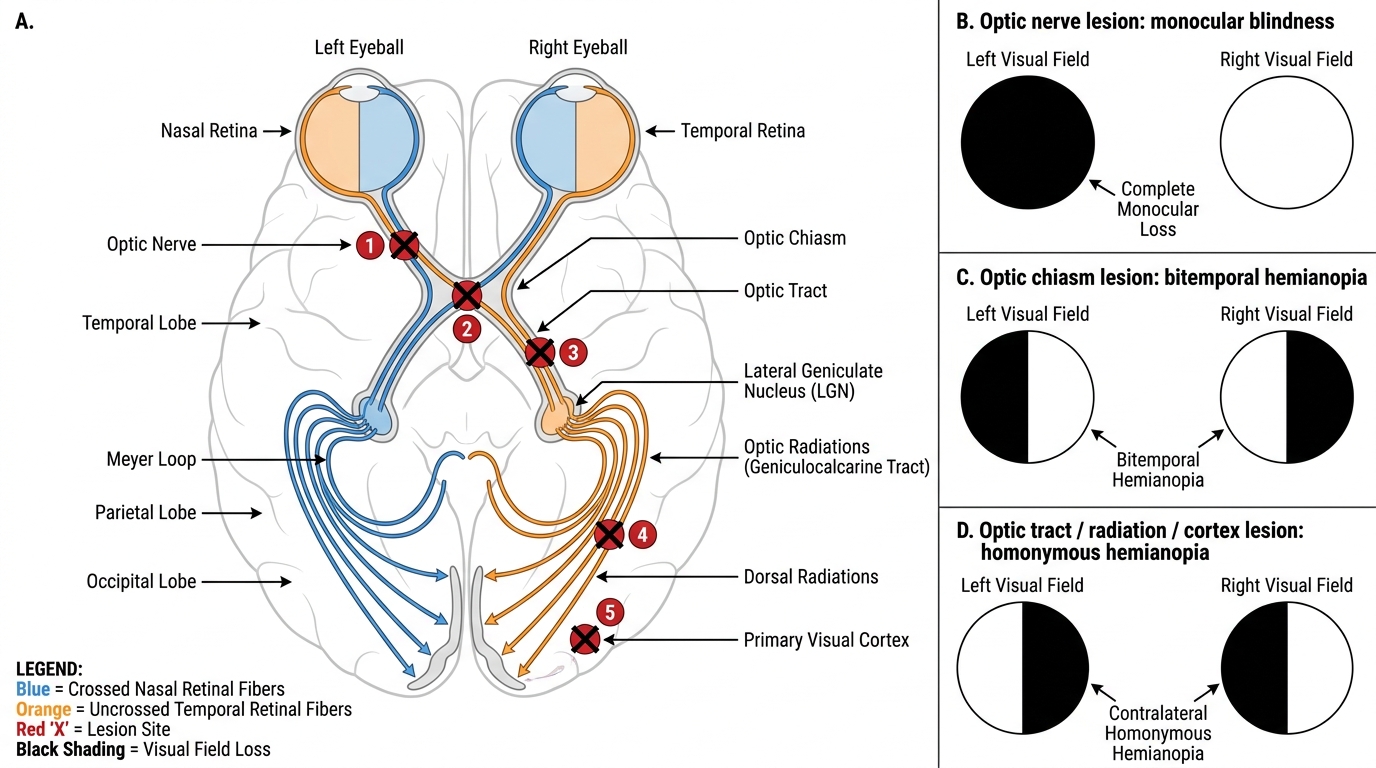
Visual Pathway and Lesion-Associated Field Defects
Ocular and Neurological Examination and Investigation
The clinical examination of a patient with suspected optic nerve or visual pathway disease integrates ophthalmic and neurological assessment tools. No single test is sufficient — the diagnosis emerges from the convergence of multiple findings.
Visual acuity (BCVA): baseline and affected eye compared. Reduced acuity in one eye with normal VA in the other points to a prechiasmal lesion.
Colour vision (Ishihara plates): exquisitely sensitive to optic nerve disease. Even when VA is near-normal, optic neuritis and compressive optic neuropathy cause profound acquired red-green dyschromatopsia (impaired colour discrimination, particularly red saturation). Patients describe reds as appearing 'washed out' or 'pink' in the affected eye.
Relative afferent pupillary defect (RAPD) — swinging flashlight test: the single most valuable bedside test for unilateral optic nerve disease. When the light swings to the affected eye, both pupils dilate (the afferent input from the affected nerve is insufficient to drive constriction). RAPD requires asymmetric optic nerve disease — it will not be present in bilateral symmetric disease.
Visual field testing: confrontation fields (bedside — each eye tested separately against the examiner's fingers in the four quadrants and centrally) provide a rapid screen. Formal automated perimetry (Humphrey visual field analysis) is required for accurate field mapping, monitoring, and medico-legal documentation. Both eyes must always be tested separately and simultaneously compared.
Fundoscopy: assess the optic disc (swollen vs pale vs normal), the retinal nerve fibre layer (RNFL thinning in glaucoma/atrophy), and the macula. In retrobulbar optic neuritis, the disc looks normal.
Visual evoked potentials (VEP): an electrophysiological test that measures the latency of the cortical response to a visual stimulus. Prolonged P100 latency is diagnostic of demyelinating optic neuritis (even in the subclinical fellow eye) and is a key MS diagnostic criterion.
MRI brain and orbits (fat-suppressed, gadolinium-enhanced): MRI is the imaging of choice for optic neuritis (enhancement of the optic nerve with gadolinium confirms inflammation), chiasmal compression (pituitary mass, craniopharyngioma), and MS white matter plaques (periventricular lesions — McDonald criteria).
Lumbar puncture: elevated opening pressure confirms raised ICP in papilloedema; CSF analysis for inflammatory cells in suspected optic neuritis or MS.
Blood tests: ESR, CRP, and temporal artery biopsy for suspected GCA; anti-AQP4 (aquaporin-4) antibodies for neuromyelitis optica (NMO) spectrum disorder — an important MS mimic in Indian patients.