Page 17 of 23
OP9.5 | Optic Nerve and Visual Pathway Disorders — SDL Guide (Part 2)
Optic Disc Disorders: Papilloedema, Optic Neuritis, AION, and Optic Atrophy
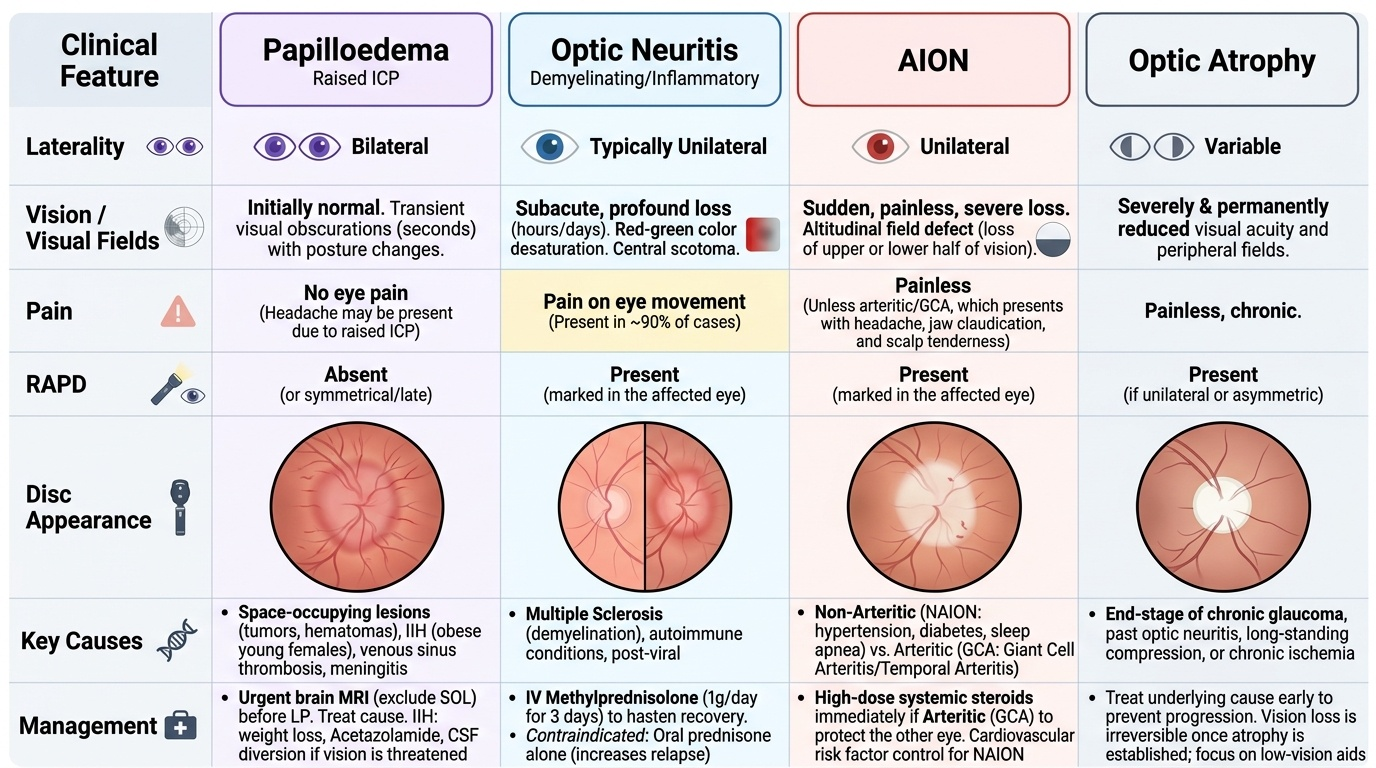
These four conditions all produce disc changes but differ fundamentally in their mechanism, laterality, symptoms, and urgency. The ability to distinguish them at the bedside is a core clinical skill.
Provided image
Papilloedema is bilateral optic disc swelling caused by raised intracranial pressure (ICP) transmitted through the subarachnoid CSF space around the optic nerve. The raised pressure passively impedes axoplasmic transport at the disc, causing disc swelling. Causes: space-occupying lesions (brain tumour, subdural/extradural haematoma), cerebral venous sinus thrombosis, meningitis, and idiopathic intracranial hypertension (IIH — obese young women, often on tetracyclines or vitamin A). Fundoscopy: bilateral blurred disc margins (especially superior and inferior), disc hyperaemia, loss of spontaneous venous pulsations, peripapillary flame haemorrhages in advanced cases. Vision is initially normal (this distinguishes it from papillitis) — transient visual obscurations lasting seconds are characteristic of IIH. Management: MRI to exclude SOL before LP; treat the cause; IIH: acetazolamide (carbonic anhydrase inhibitor reducing CSF production), weight loss, and optic nerve sheath fenestration or CSF diversion if vision is threatened.
Optic neuritis is inflammation of the optic nerve, most commonly demyelinating (in the context of multiple sclerosis). It is typically unilateral, affecting young adults (especially women). The characteristic features: subacute painless or painful visual loss over hours to days, pain on eye movement (present in ~90%), reduced colour vision (red desaturation), central scotoma, RAPD in the affected eye. The disc may be swollen (papillitis, if the inflammation is at the disc head) or normal (retrobulbar optic neuritis, more common — 'the patient sees nothing and the doctor sees nothing on fundoscopy'). Recovery typically occurs over 4-12 weeks. The ONTT trial demonstrated that IV methylprednisolone (1 g/day for 3 days) hastens recovery by approximately 2 weeks but does NOT improve visual acuity at 1 year compared to placebo. Oral prednisone alone was associated with increased relapse rate and should NOT be used. Approximately 50% of patients with isolated optic neuritis will develop MS within 15 years (higher risk with MRI white matter lesions at onset).
Anterior Ischaemic Optic Neuropathy (AION): ischaemia of the anterior portion of the optic nerve (supplied by the posterior ciliary arteries). Two types:
- Arteritic AION (A-AION) from giant cell arteritis (GCA): sudden, often profound visual loss (frequently total, or near-total), painless in the eye itself but associated with headache and GCA symptoms. Disc: chalky white, swollen. ESR and CRP are markedly elevated. This is a bilateral ocular emergency — the fellow eye is at risk within 24-48 hours without treatment. Immediate high-dose IV methylprednisolone (1 g/day for 3 days, then oral prednisolone) must be given before temporal artery biopsy — do NOT delay treatment to wait for biopsy results.
- Non-arteritic AION (NA-AION): more common; associated with atherosclerotic risk factors (HTN, DM, hyperlipidaemia), small optic disc anatomy ('disc at risk' — small crowded disc with small cup). Visual loss is typically altitudinal (inferior or superior half of field) and less severe than A-AION. Disc: pale oedema (less hyperaemic than arteritic). No proven effective treatment.
Optic atrophy is the common end stage of any process that destroys optic nerve axons. Primary optic atrophy (direct damage without prior swelling) produces a chalk-white disc with sharp margins — seen in glaucoma, compressive optic neuropathy, toxic/nutritional optic neuropathy, and Leber hereditary optic neuropathy. Secondary optic atrophy (follows papilloedema) produces a pale disc with blurred margins initially. The disc is pale, vision is reduced, and RAPD is present in unilateral cases.
SELF-CHECK
A 70-year-old man with a 2-week history of severe temporal headache and jaw claudication presents with sudden profound visual loss in his left eye this morning. The left disc is pale and swollen. ESR is 92 mm/hour. What is the diagnosis and the most urgent immediate action?
A. Non-arteritic AION — arrange MRI orbit and refer to ophthalmology within 1 week
B. Arteritic AION from giant cell arteritis — immediate high-dose IV methylprednisolone to protect the fellow eye
C. Optic neuritis from MS — IV methylprednisolone 1g for 3 days; arrange MRI brain
D. Papilloedema from raised ICP — urgent MRI brain to exclude SOL, then LP
Reveal Answer
Answer: B. Arteritic AION from giant cell arteritis — immediate high-dose IV methylprednisolone to protect the fellow eye
This is arteritic AION from giant cell arteritis (GCA): an elderly patient with temporal headache, jaw claudication, markedly elevated ESR (92 mm/hour), and sudden profound visual loss with a pale swollen disc. This is a bilateral ocular emergency — without immediate treatment, the fellow eye loses vision in 24-48 hours in up to 50% of untreated patients. Treatment: immediate IV methylprednisolone 1 g/day for 3 days, then transition to high-dose oral prednisolone. Temporal artery biopsy should be arranged within 7-14 days but must NOT delay treatment. Non-arteritic AION has no GCA features; optic neuritis affects young adults with painful eye movement and a different clinical profile; papilloedema is bilateral with preserved vision initially.
Visual Pathway Lesions: Chiasm, Tract, Radiation, and Cortex
Lesions beyond the optic nerve — at the chiasm, tract, radiation, and cortex — produce bilateral visual field defects because both visual fields share representation at these levels. The pattern of the field defect is a direct anatomical clue.
Chiasmal lesions: the most common cause of chiasmal compression is a pituitary macroadenoma (a non-functioning or hormone-secreting pituitary tumour) growing superiorly and pressing on the inferior surface of the chiasm. The crossing nasal fibres (representing the temporal field of each eye) are damaged first, producing the classic bitemporal hemianopia: both temporal fields are lost, nasal fields are preserved. On formal perimetry, the defect respects the vertical midline. Other chiasmal lesions: craniopharyngioma (most common in children; calcified suprasellar cyst from Rathke's pouch remnant), meningioma of the tuberculum sellae, and rarely optic glioma.
Note that pituitary tumours cause additional features beyond visual fields: hypopituitarism (failure of pituitary hormones — remember the mnemonic FSH/LH → GH → TSH → ACTH order of failure), and acromegaly or Cushing's disease if the tumour is secretory. Bitemporal hemianopia in a patient with headaches and endocrine features should prompt urgent MRI pituitary and endocrinology review.
Optic tract lesions: produce incongruous homonymous hemianopia (defects in the two eyes are not identical — the upper and lower halves of the hemifield affected in each eye may not match exactly). Optic tract lesions are uncommon in isolation; most causes are internal carotid aneurysm, craniopharyngioma, or demyelination.
Optic radiation lesions — temporal lobe (Meyer's loop): the inferior fibres of the optic radiation loop forward through the temporal lobe (Meyer's loop). Temporal lobe pathology (tumour, infarct, herpes encephalitis, epilepsy surgery) damages these inferior fibres, which represent the contralateral superior visual field, producing a superior homonymous quadrantanopia ('pie in the sky'). This can be the presenting visual field finding of a temporal lobe tumour or infarct.
Optic radiation lesions — parietal lobe: the superior fibres of the optic radiation pass through the parietal lobe, representing the contralateral inferior visual field. Parietal lobe lesions produce inferior homonymous quadrantanopia ('pie in the floor').
Occipital cortex lesions: a posterior cerebral artery (PCA) infarct — the most common cause of homonymous hemianopia — produces a congruous homonymous hemianopia with macular sparing (the macular representation at the occipital tip is spared because of collateral MCA supply). Bilateral PCA infarction causes cortical blindness — the patient is completely blind but both pupils react normally to light (because the pupillary pathway leaves the optic tract before reaching the cortex).
Management of Optic Nerve and Visual Pathway Disorders
Management is determined by the underlying cause, anatomical level, and urgency of the condition. Several principles apply broadly.
Papilloedema — treat the cause first:
MRI brain (or CT if MRI unavailable) to exclude space-occupying lesion before any lumbar puncture. Treat the primary cause (drain SOL, treat meningitis, anticoagulate venous sinus thrombosis). For IIH (idiopathic intracranial hypertension): acetazolamide (500 mg–2 g/day) reduces CSF production and is first-line medical treatment; weight loss (most effective long-term for obese patients); optic nerve sheath fenestration (creates a slit in the dural sheath to decompress the nerve) for rapidly progressive visual loss; CSF diversion surgery (lumboperitoneal or ventriculoperitoneal shunt) for intractable cases.
Optic neuritis:
The ONTT trial evidence: IV methylprednisolone 1 g/day for 3 days, followed by oral prednisolone taper, hastens visual recovery by ~2 weeks but does not improve VA at 1 year. Oral prednisone alone (without IV pre-treatment) was associated with increased relapse rate in the original ONTT study — it should not be used as monotherapy. MRI brain at first episode: periventricular T2/FLAIR white matter lesions at presentation predict higher conversion risk to MS — neurological referral is mandatory. Disease-modifying therapy for MS (beta-interferons, natalizumab, fingolimod) reduces relapse rate and should be started under neurology supervision.
Giant cell arteritis (GCA) — arteritic AION:
Emergency management: immediate IV methylprednisolone 1 g/day for 3 days (some centres start with oral prednisolone 80 mg/day if IV is unavailable), then transition to high-dose oral prednisolone (1 mg/kg/day), slow taper over 12-24 months guided by ESR/CRP. Temporal artery biopsy should be arranged within 7-14 days of steroid initiation (steroids do not cause false-negative biopsy immediately, though sensitivity declines after 2-4 weeks). Aspirin is added for its additional protective effect against vascular events in GCA. Monitor for steroid side effects (osteoporosis prophylaxis, blood sugar monitoring).
Chiasmal compression:
Most pituitary macroadenomas causing bitemporal hemianopia require transsphenoidal surgery (endoscopic or microscopic, through the nasal/sphenoidal approach) to decompress the chiasm. Visual field defects often improve significantly after decompression if the compression is not long-standing. Prolactinomas are treated medically first (dopamine agonists — cabergoline, bromocriptine) and may not require surgery. Post-operative visual field monitoring is performed regularly.
Non-arteritic AION:
No proven effective treatment. Optimise vascular risk factors (BP, diabetes, dyslipidaemia, smoking). Low-dose aspirin is often prescribed empirically (uncertain benefit but low risk). Visual outcome varies — some patients have partial recovery, others retain the field loss.
CLINICAL PEARL
Three 'can't miss' rules in neuro-ophthalmology: (1) Bilateral disc swelling is papilloedema until proven otherwise — do MRI brain before LP. (2) Painful visual loss in a young person with RAPD and red desaturation = optic neuritis — do not miss this as the first presentation of MS. (3) Any visual field defect that respects the vertical midline is chiasmal or retrochiasmal — test both eyes' fields and image the brain. These three rules cover most of the catastrophic misdiagnoses in this field. A related practical point: always test colour vision with Ishihara plates in a patient with suspected optic nerve disease — colour desaturation may be the only sign when VA is still near normal.
SELF-CHECK
A 26-year-old woman presents with a 5-day history of right eye pain on movement and progressive blurring of right-sided vision. RAPD is present in the right eye. Fundoscopy is normal bilaterally. Ishihara testing shows impaired colour discrimination in the right eye. MRI brain shows three periventricular T2 white matter lesions. What is the diagnosis, and what does the MRI finding imply?
A. Right optic neuritis with MRI findings suggesting high risk of conversion to multiple sclerosis
B. Right papilloedema from raised ICP — the T2 lesions confirm venous sinus thrombosis
C. Right arteritic AION from GCA — check ESR immediately and start steroids
D. Right CRAO — normal fundoscopy excludes retinal disease
Reveal Answer
Answer: A. Right optic neuritis with MRI findings suggesting high risk of conversion to multiple sclerosis
Painful eye movement, progressive unilateral visual loss, RAPD, impaired colour vision, and a normal-looking fundus (retrobulbar optic neuritis) is the classic presentation of acute optic neuritis. The MRI finding of periventricular T2 white matter lesions (greater than two lesions in a young person presenting with optic neuritis) strongly predicts conversion to multiple sclerosis (in the ONTT trial, patients with ≥1 T2 lesion on MRI at onset had ~72% conversion to MS at 15 years). This patient needs urgent neurological referral for MS diagnosis (McDonald criteria) and assessment for disease-modifying therapy. GCA affects patients over 50 with systemic inflammatory symptoms; CRAO produces pale retinal ischaemia on fundoscopy; papilloedema is bilateral and does not present with colour loss or painful eye movement.
Self-Assessment
Apply your knowledge of the visual pathway and optic nerve disorders to these structured questions.
Question 1. A 45-year-old man is found to have a bitemporal hemianopia on Humphrey visual field analysis performed during a routine eye examination. He has no headache or visual complaints. What anatomical structure is most likely to be compressing the visual pathway at this level, and what imaging should be arranged?
Answer: Bitemporal hemianopia indicates compression of the crossing nasal fibres at the optic chiasm. The most common cause is a pituitary macroadenoma growing superiorly from the sella turcica. In the absence of symptoms, this may be a 'silent' non-functioning adenoma detected incidentally. Arrange MRI brain with gadolinium, pituitary protocol (thin cuts through the pituitary region). Also arrange endocrine assessment (pituitary hormone panel: FSH, LH, GH, TSH, ACTH, prolactin) — non-functioning tumours may still compress the pituitary stalk and cause hyperpituitarism or hypopituitarism.
Question 2. Explain why IV methylprednisolone for optic neuritis hastens recovery but does not change the final outcome at 1 year. Why is oral prednisone alone not recommended?
Answer: IV methylprednisolone accelerates the rate of remyelination and reduction of inflammation, producing earlier visual improvement (approximately 2 weeks faster than spontaneous recovery). However, the final visual acuity at 1 year is determined by the extent of axonal damage — once axons are damaged during the attack, no amount of anti-inflammatory treatment restores them after the fact; myelin repair takes the same time with or without treatment in the long run. Oral prednisone alone (without the high-dose IV component) was associated with an increased rate of relapse of optic neuritis in the ONTT trial — the mechanism is debated, but it may be related to incomplete suppression of immune activation with lower peak steroid levels. For this reason, it is not recommended.
Question 3. A 65-year-old woman has cortical blindness following bilateral PCA infarction. When you examine her pupils with a flashlight, both pupils react normally. Why?
Answer: The pupillary light reflex pathway branches off from the optic tract before reaching the lateral geniculate nucleus (LGN) — it diverges to the pretectal nucleus and Edinger-Westphal nucleus in the midbrain. The visual cortex is NOT required for the pupillary reflex. Therefore, even when the entire cortical visual system is destroyed (bilateral occipital infarction), the pupillary reflex pathway is intact and both pupils react normally. This is the clinical diagnostic point that distinguishes cortical blindness from bilateral optic nerve disease (where the RAPD would be absent but pupils might be sluggish or afferent defect might be detectable).