Page 9 of 23
OP9.3 | Retinal Vascular Occlusions — SDL Guide
Learning Objectives
- Classify retinal vascular occlusions into arterial (CRAO, BRAO) and venous (CRVO, BRVO) types with their characteristic clinical and fundoscopic features
- Explain the pathophysiology of retinal artery and vein occlusions including the role of emboli, thrombosis, and arteriovenous compression
- Recognise CRAO as an ocular emergency requiring management within 90 minutes and initiate appropriate emergency workup
- Distinguish ischaemic from non-ischaemic CRVO and describe the risk of neovascular glaucoma
- Describe the management of venous occlusions including anti-VEGF therapy, laser photocoagulation, and systemic risk factor control
INSTRUCTIONS
Retinal vascular occlusions are the retinal equivalent of strokes — sudden, dramatic, and potentially irreversible events that deprive the retina of blood supply. Central retinal artery occlusion is a true emergency where the treatment window may be as short as 90 minutes. Understanding the four types of retinal vascular occlusion — their presentations, mechanisms, fundoscopic appearances, and management — prepares you to act decisively when a patient presents with sudden monocular visual loss.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Chapter on Retinal Vascular Disorders (textbook)
- Parsons' Diseases of the Eye, 22nd ed. Chapter on Vascular Diseases of the Retina (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old hypertensive man presents to your outpatient clinic at 10 AM reporting that he suddenly lost vision in his right eye at approximately 9:20 AM — 40 minutes ago. He describes 'everything going black, like someone switched off a light.' The eye is white and quiet, no pain. Fundoscopy reveals a pale, milky-white retina with a striking cherry-red spot at the fovea. His left eye is normal. This is central retinal artery occlusion (CRAO) — the visual equivalent of a stroke. The window for any meaningful intervention is within 90 minutes of onset. It is now 10 AM. You have approximately 50 minutes to act.
WHY THIS MATTERS
Retinal vascular occlusions — whether arterial or venous — represent vascular emergencies or urgent conditions that a general physician may encounter before an ophthalmologist does. A patient presenting with sudden monocular visual loss has retinal artery occlusion until proven otherwise, and your initial response in the first 90 minutes can determine whether any vision is salvaged. Beyond the acute event, these conditions are windows into systemic vascular disease: CRAO demands a stroke-equivalent investigation (carotid Doppler, echocardiogram, cardiac monitoring) because the embolus that occluded the retinal artery could equally have gone to the brain. Venous occlusions signal hypertension, hyperviscosity, and glaucoma risk. Every physician needs to recognise these conditions and act.
RECALL
Recall the vascular supply of the retina: the central retinal artery (CRA) is a branch of the ophthalmic artery (from the internal carotid artery), and enters the eye through the optic nerve alongside the central retinal vein (CRV). At the disc, both vessels branch into superior and inferior arcades. The inner two-thirds of the retina is supplied by the retinal circulation; the outer third (photoreceptors) is supplied by the choroidal circulation — a separate system. This dual supply is critical to understanding why CRAO produces a cherry-red spot: the fovea, being thin and lacking inner retinal layers, receives its oxygen from the choroid and therefore remains red when the surrounding retina becomes pale from ischaemia. Also recall that atherosclerosis and thrombosis underlie arterial occlusions, while venous hypertension and stasis underlie venous occlusions — both driven by systemic vascular risk factors.
The Emergency Presentation: Sudden Painless Visual Loss
The cardinal symptom of retinal vascular occlusion is sudden, painless, monocular visual loss. The word 'sudden' is critical — patients typically describe an instantaneous event, as if a light was switched off (arterial) or a curtain was drawn (either type). 'Painless' distinguishes it from acute angle-closure glaucoma (which causes a painful, red eye with nausea and haloes). 'Monocular' distinguishes it from cortical visual loss (which produces a homonymous hemianopia, affecting the same visual field in both eyes).
The specific character of the visual loss varies by which vessel is occluded. In CRAO (central retinal artery occlusion), the visual loss is total or near-total in the affected eye — the patient may retain only light perception or hand movements, because the entire inner retina is ischaemic. The onset is instantaneous. In BRAO (branch retinal artery occlusion), the visual loss is partial — a scotoma or an altitudinal field defect corresponding to the territory of the occluded branch artery. The patient may describe a 'dark patch' in part of their vision.
In CRVO (central retinal vein occlusion), visual loss is typically less sudden and less severe than CRAO, ranging from mild blurring to severe loss depending on the degree of ischaemia. In BRVO (branch retinal vein occlusion), the loss is segmental (affecting one quadrant or sector of vision) and may be noticed as a blurred area in part of the visual field.
Key principle: any patient presenting with sudden monocular visual loss must have their fundus examined immediately. Do not reassure them, do not attribute it to 'migraine' without fundoscopy, and do not delay examination. In CRAO, every minute of delay is more retinal cells dying.
Anatomy and Pathophysiology of Retinal Vascular Occlusion
The retinal vascular occlusions are a pathologically and anatomically coherent group: all four arise from interruption of flow in specific retinal vessels, and the clinical picture follows directly from the anatomy of the occluded vessel and the territory it supplies.
Arterial occlusions most commonly arise from embolism. In CRAO, an embolus — most often a calcific plaque from the carotid artery, a cholesterol (Hollenhorst) plaque, or a cardiac thrombus — lodges at the central retinal artery or its origin at the ophthalmic artery. The embolic origin explains why CRAO investigations follow the stroke workup pathway: carotid imaging, echocardiography, cardiac rhythm monitoring. Less commonly, CRAO results from thrombosis in situ (in the context of giant cell arteritis — a critical diagnosis to exclude, especially in patients over 50 with headache, jaw claudication, or temporal artery tenderness). In BRAO, the embolus lodges in a branch artery, causing ischaemia in the corresponding retinal sector.
The retina is among the most metabolically demanding tissues in the body. The inner two-thirds of the retina depends entirely on the retinal circulation; ischaemia causes irreversible damage within minutes. The fovea is an exception: it has no inner retinal layers and is nourished by the choroid. In CRAO, when the surrounding retina swells and becomes pale from ischaemia, the intact choroidal supply beneath the thin fovea produces the pathognomonic cherry-red spot — the choroid shows through as a red disc against the white ischaemic background.
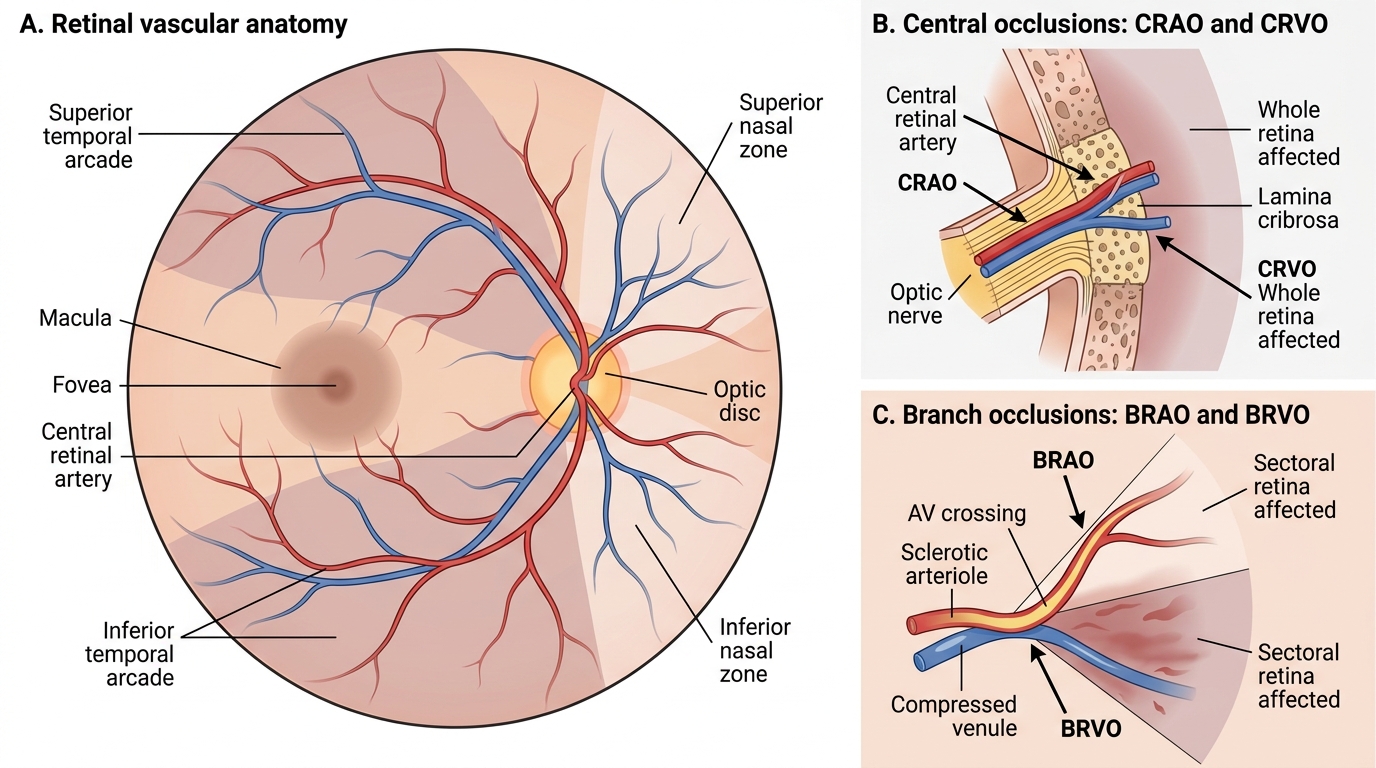
Retinal Vascular Anatomy and Sites of Occlusion
Venous occlusions arise from thrombosis within the vein, at specific anatomical points. In CRVO, thrombosis occurs at or behind the lamina cribrosa (where the central retinal vein shares an adventitial sheath with the central retinal artery), and arterial wall disease from hypertension compresses the vein from outside. In BRVO, thrombosis occurs at arteriovenous crossing points where a sclerotic retinal arteriole crosses over and compresses an underlying venule — this is why BRVO is most commonly superotemporal (the most frequent AV crossing site). The increase in venous pressure proximal to the block drives haemorrhages, oedema, and ischaemia in the territory drained by that vein.
Systemic risk factors common to all four types: hypertension (most important, especially for venous occlusions), hyperlipidaemia, diabetes, smoking, hyperviscosity (polycythaemia, myeloma, antiphospholipid syndrome), and for arterial occlusions specifically: carotid artery disease, atrial fibrillation, cardiac valvular disease.
Ocular Examination and Investigation
The examination of a patient with retinal vascular occlusion combines urgent fundoscopy with specific additional tests that grade severity and guide management.
Visual acuity: measure immediately — both eyes. In CRAO, VA may be reduced to perception of light or hand movements in the affected eye. In CRVO, VA ranges from 6/9 to hand movements depending on ischaemic severity. Retained good VA in the acute setting suggests non-ischaemic CRVO or BRAO.
Relative afferent pupillary defect (RAPD): a swinging light test finding where the affected pupil dilates when the light swings to it (indicating reduced afferent input from the ischaemic retina). RAPD is present in CRAO and ischaemic CRVO, but absent or minimal in non-ischaemic CRVO. Detection of RAPD in a CRVO patient is an important marker that the occlusion is ischaemic.
Dilated fundoscopy: the primary diagnostic tool. See 'Classification' heading below for specific fundoscopic appearances. Key to look for: retinal pallor, cherry-red spot (CRAO), flame haemorrhages (venous occlusions), disc swelling, venous tortuosity.
Optical coherence tomography (OCT): detects macular oedema (a complication of both CRVO and BRVO) and guides anti-VEGF treatment decisions.
Fluorescein fundus angiography (FFA): shows extent of non-perfusion (capillary drop-out), confirms arterial vs venous occlusion, grades ischaemic vs non-ischaemic CRVO (ischaemic CRVO = >10 disc areas of capillary non-perfusion). Also used to confirm CRAO (absent or delayed arterial filling).
Systemic investigation (especially for CRAO and CRVO):
- BP measurement (both arms)
- Fasting glucose and HbA1c
- Full blood count and ESR/CRP (ESR markedly elevated in giant cell arteritis)
- Lipid profile
- Carotid Doppler ultrasonography (for CRAO/BRAO — arterial source)
- Echocardiogram (cardiac embolus source)
- ECG and cardiac rhythm monitoring (atrial fibrillation)
- Clotting screen and antiphospholipid antibodies (in younger patients without obvious risk factors)
- Plasma protein electrophoresis (if hyperviscosity suspected)