Page 10 of 23
OP9.3 | Retinal Vascular Occlusions — SDL Guide (Part 2)
Classification and Differential Diagnosis
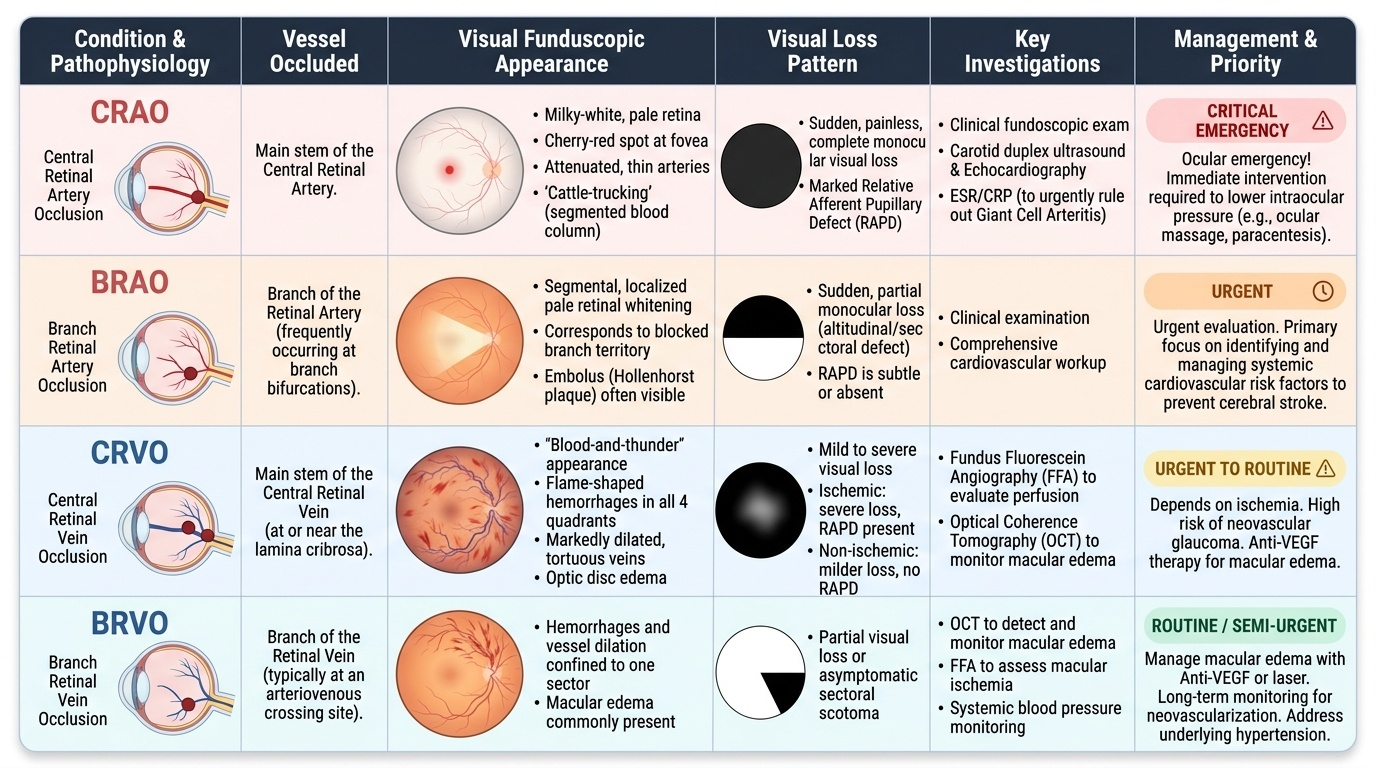
The four types of retinal vascular occlusion must be systematically distinguished from each other and from other causes of acute visual loss. The clinical pattern — particularly the character of visual loss, fundoscopic appearance, and RAPD — usually allows an immediate diagnosis.
Provided image
CRAO (Central Retinal Artery Occlusion): Sudden, complete monocular visual loss. Fundus: pale, milky-white, oedematous retina involving the posterior pole, with a cherry-red spot at the fovea (the one area where the choroidal supply prevents pallor). A Hollenhorst (cholesterol) plaque may be visible in a branch arteriole. Arteries are attenuated, veins may show 'cattle-trucking' (segmented column of blood). Marked RAPD. This is a true ocular emergency.
BRAO (Branch Retinal Artery Occlusion): Sudden, partial monocular visual loss — typically a quadratic or altitudinal field defect. Fundus: segmental pale retinal whitening corresponding to the territory of the blocked branch artery. The cherry-red spot may not be present if the macular artery is not occluded. RAPD may be absent or subtle.
CRVO (Central Retinal Vein Occlusion): Visual loss ranging from mild to severe. Fundus: the classic 'blood-and-thunder' appearance — flame haemorrhages scattered in all four quadrants, markedly dilated and tortuous veins, disc oedema, and cotton-wool spots. CRVO is further classified into:
- Non-ischaemic (partial) CRVO: better VA (often ≥6/18), milder haemorrhages, no RAPD, <10 disc areas of non-perfusion on FFA; better prognosis.
- Ischaemic CRVO: severe VA loss (often ≤6/60 or hand movements), dense haemorrhages in all quadrants, RAPD present, >10 disc areas of non-perfusion on FFA; high risk (~30%) of rubeosis iridis and neovascular glaucoma within 3 months.
BRVO (Branch Retinal Vein Occlusion): Partial monocular visual loss or asymptomatic scotoma. Fundus: flame haemorrhages confined to one sector (most commonly superotemporal quadrant), dilated tortuous veins in that sector, and possible macular oedema. History of hypertension is almost universal.
Differential diagnosis of acute monocular visual loss: giant cell arteritis (CRAO in elderly, with headache and elevated ESR — emergency: start IV steroids), ischaemic optic neuropathy (disc swelling, altitudinal field loss, no cherry-red spot), vitreous haemorrhage (no fundal view, red glow on illumination), retinal detachment (shadow in peripheral field, 'curtain' or 'flap'), anterior ischaemic optic neuropathy (AION).
SELF-CHECK
A 72-year-old woman presents with sudden complete loss of vision in her left eye that began 30 minutes ago. Fundoscopy shows a pale, milky-white retina with a bright red spot at the fovea. Her left pupil dilates when the light is swung from right to left (RAPD present). ESR is 105 mm/hour. What is the priority diagnosis to exclude, and what is the immediate action?
A. CRAO from carotid atherosclerosis — urgent ocular massage and anterior chamber paracentesis
B. Giant cell arteritis causing CRAO — immediate high-dose systemic corticosteroids and urgent ESR/CRP, temporal artery biopsy
C. Non-ischaemic CRVO — reassure and arrange ophthalmology review in 2 weeks
D. BRAO — no emergency treatment; investigate for carotid disease electively
Reveal Answer
Answer: B. Giant cell arteritis causing CRAO — immediate high-dose systemic corticosteroids and urgent ESR/CRP, temporal artery biopsy
An elderly woman with CRAO and a markedly elevated ESR (105 mm/hour) must be treated as giant cell arteritis (GCA) until proven otherwise — this is a systemic inflammatory vasculitis that can occlude the central retinal artery. GCA requires immediate high-dose corticosteroids (typically prednisolone 60-80 mg/day PO or IV methylprednisolone for threatened vision) to prevent involvement of the other eye, which can lose vision within 24-48 hours if untreated. Temporal artery biopsy should be arranged but must NOT delay steroid treatment. CRAO from atherosclerosis is also in the differential, but the elevated ESR makes GCA the priority. Non-ischaemic CRVO and BRAO are incorrect — the fundus shows CRAO features, and the urgency level is far greater.
Management of Arterial Occlusions
Management of retinal arterial occlusions is dominated by the extreme time-sensitivity of CRAO and the need to identify and treat the systemic embolic source to prevent stroke.
CRAO — Acute Management (within 90 minutes of onset, ideally sooner):
The inner retina tolerates only 90-100 minutes of ischaemia before irreversible infarction becomes complete. The following measures aim to dislodge or lyse the embolus and restore perfusion — their evidence base is modest, but the time window is short and the alternative is permanent blindness. The ophthalmologist must act immediately, and the physician referring the patient must communicate the time of onset clearly, since the window for meaningful intervention is far shorter than in stroke (where tPA is given within 4.5 hours). Every minute of continued occlusion means additional cone and ganglion cell death in the ischaemic inner retina.
- Ocular massage: firm digital pressure on the closed eyelid for 10-15 seconds, then sudden release, repeated for 10-15 minutes. The oscillating IOP changes may dislodge the embolus and shift it distally into a smaller arteriole.
- IOP lowering: instil topical timolol 0.5% and oral acetazolamide 500 mg stat to reduce IOP acutely, increasing the arterio-venous pressure gradient and improving arterial filling.
- Anterior chamber paracentesis (AC tap): performed by an ophthalmologist; sudden removal of a small volume of aqueous humour causes an acute drop in IOP, which may restore arterial perfusion if performed within the time window.
- Breathing into a paper bag (carbogen inhalation): the rationale is that hypercapnia causes vasodilatation of the retinal arterioles; the benefit is unproven but it carries minimal risk.
- Systemic thrombolysis (tPA): some centres have used intra-arterial tPA delivered by interventional radiology, particularly in young patients with recent onset and no embolic source identified. Evidence is limited; risk of stroke or haemorrhage must be weighed.
Systemic investigation for embolic source: treat CRAO as an ocular TIA. Investigate urgently: carotid Doppler (carotid stenosis), echocardiography (cardiac thrombus, vegetation, patent foramen ovale), cardiac monitoring for atrial fibrillation. Antiplatelet therapy (aspirin) should be started immediately in atherosclerotic CRAO.
Exclude giant cell arteritis (GCA): in any patient over 50 presenting with CRAO, measure ESR and CRP immediately. If GCA is suspected (headache, jaw claudication, temporal artery tenderness, elevated ESR/CRP), initiate high-dose corticosteroids without waiting for temporal artery biopsy — the fellow eye is at imminent risk.
BRAO: less acute than CRAO. Embolic workup is the same priority. Visual prognosis is better because the territory is smaller. Macular oedema (if present) may be treated with intravitreal anti-VEGF.
Management of Venous Occlusions
Venous occlusions are not emergencies in the same sense as CRAO, but they require timely investigation and treatment to prevent secondary complications — particularly macular oedema (reducing vision) and neovascular glaucoma (in ischaemic CRVO).
CRVO — Management:
The primary ocular complications of CRVO are (1) macular oedema causing vision loss and (2) neovascularisation (iris rubeosis → neovascular glaucoma) in ischaemic CRVO. These two complications are temporally distinct: macular oedema develops early, often within weeks of the occlusion, and is the dominant cause of initial visual acuity loss; neovascularisation is a delayed complication that develops over the ensuing 90 days (the '100-day glaucoma' of ischaemic CRVO) as ischaemia-driven VEGF upregulation triggers new vessel formation on the iris and angle. Treatment strategies therefore differ: the ophthalmologist treats macular oedema immediately with intravitreal agents, while monitoring the anterior segment monthly for the threat of neovascular glaucoma.
- Macular oedema in CRVO: intravitreal anti-VEGF injections (ranibizumab or aflibercept) are first-line treatment. The CRUISE trial demonstrated that ranibizumab significantly improved visual acuity in CRVO-related macular oedema. Intravitreal dexamethasone implant (Ozurdex) is an alternative, particularly in phakic patients who cannot attend for monthly injections, but carries risk of cataract and glaucoma. Monthly injections are typically required initially.
- Ischaemic CRVO: monitor closely (monthly) for rubeosis iridis (new vessels on the iris) over the first 3 months — approximately 30% of ischaemic CRVO develops this complication. When rubeosis or anterior chamber angle neovascularisation is detected, pan-retinal photocoagulation (PRP) is performed urgently to reduce VEGF and regress the new vessels, preventing progression to neovascular glaucoma (NVG) — a devastating, painful secondary glaucoma from angle closure by fibrovascular membrane.
BRVO — Management:
- Macular oedema: intravitreal anti-VEGF (ranibizumab — BRAVO trial) is first-line. Grid laser photocoagulation (treating leaking capillaries in the oedematous macular area) is an alternative if oedema persists beyond 3 months.
- Neovascularisation from BRVO: sector PRP to the ischaemic quadrant reduces the VEGF source.
Systemic management for all venous occlusions:
- Optimise BP (target <130/80 mmHg) — the most important modifiable risk factor for CRVO/BRVO
- Control diabetes, hyperlipidaemia
- Avoid dehydration and haemoconcentration
- In young patients without traditional risk factors: screen for thrombophilia (factor V Leiden, antiphospholipid antibodies, hyperhomocysteinaemia), hyperviscosity (polycythaemia, myeloma), and consider anticoagulation
CLINICAL PEARL
The cherry-red spot of CRAO and the blood-and-thunder fundus of CRVO are the two most visually distinctive fundoscopic findings in medicine — they are almost impossible to miss once you have seen them in a photograph. But there is a more subtle clinical pearl: the RAPD (relative afferent pupillary defect) is the bedside test that separates ischaemic from non-ischaemic CRVO even before FFA. If the affected eye shows a clear RAPD on swinging flashlight test, the retinal ischaemia is extensive — this is ischaemic CRVO, and you must watch closely for rubeosis iridis over the next 3 months. If no RAPD is detectable, the occlusion is more likely non-ischaemic, with a better prognosis. Always test RAPD in any monocular visual loss — it takes 10 seconds and costs nothing.
SELF-CHECK
Three weeks after a CRVO diagnosis, a 60-year-old hypertensive man reports that his left eye (the affected eye) has been painful and red. On examination, you see new vessels on the iris. What complication has developed, and what is the appropriate management?
A. Anterior uveitis — treat with topical steroids and cycloplegics
B. Rubeosis iridis leading to neovascular glaucoma — urgent pan-retinal photocoagulation and IOP-lowering treatment
C. CRVO recurrence — repeat anti-VEGF injection into the vitreous
D. Episcleritis — reassure and treat with topical NSAIDs
Reveal Answer
Answer: B. Rubeosis iridis leading to neovascular glaucoma — urgent pan-retinal photocoagulation and IOP-lowering treatment
New vessels on the iris (rubeosis iridis) in a patient with recent ischaemic CRVO represent the classic feared complication — occurring in approximately 30% of ischaemic CRVOs within 3 months of the initial event. The growing fibrovascular membrane closes the anterior chamber angle, producing neovascular glaucoma (NVG), which causes severe pain, raised IOP, and risk of permanent visual loss. Management: urgent pan-retinal photocoagulation (PRP) to ablate the ischaemic retina and reduce VEGF drive; intravitreal anti-VEGF to acutely suppress rubeosis; IOP-lowering medications (and eventually filtering surgery if medical treatment fails). This is not uveitis, episcleritis, or CRVO recurrence.
Self-Assessment
Apply your knowledge of retinal vascular occlusions to these structured questions.
Question 1. Why does central retinal artery occlusion (CRAO) produce a cherry-red spot at the fovea, while the surrounding retina is pale?
Answer: The surrounding retina becomes pale because the ischaemic inner retinal layers (ganglion cells, inner plexiform, inner nuclear) swell with intracellular oedema when deprived of their retinal arterial supply — this opaque swelling scatters light and obscures the underlying orange-red choroidal colour. The fovea is exempt from this pallor because it lacks inner retinal layers (it is only one cell thick — the cone layer), and its oxygen is supplied by the choroid (not the retinal artery). With the surrounding retina pale, the preserved red choroidal colour at the fovea stands out as the cherry-red spot.
Question 2. How do you distinguish a BRVO from diabetic retinopathy on fundoscopy in a patient who has both hypertension and diabetes?
Answer: The key distinguishing feature is the distribution of haemorrhages. In BRVO, haemorrhages are strictly confined to one sector — the territory drained by the occluded branch vein (most commonly the superotemporal quadrant) — and are flame-shaped (superficial, nerve fibre layer). The affected sector also shows dilated tortuous veins. In diabetic retinopathy, haemorrhages are bilateral, diffuse, dot-blot shaped (deep, intraretinal), without a sector boundary, and accompanied by microaneurysms and hard exudates. In a patient with both conditions, look for both patterns simultaneously.
Question 3. A 55-year-old woman with CRVO is found to have no RAPD on swinging flashlight test, visual acuity of 6/18, and relatively mild haemorrhages. How does this finding affect her prognosis and follow-up plan?
Answer: Absence of RAPD and better visual acuity (6/18) in CRVO indicates non-ischaemic (partial) CRVO — the less severe form, with fewer capillary non-perfusion areas and a better visual prognosis. Non-ischaemic CRVO has a significantly lower risk (~3-5%) of neovascular glaucoma (rubeosis) compared to ischaemic CRVO (~30%). Follow-up is still required (monthly for at least 3 months to ensure she does not convert to ischaemic CRVO, which can happen). The main treatment priority is macular oedema, if present — treat with intravitreal anti-VEGF. Systemic BP control is mandatory.