Page 12 of 26
OR1.4-5 | Common Joint Dislocation Recognition and Reduction Assistance — SDL Guide
Learning Objectives
- Describe the etiopathogenesis and clinical features of dislocation of the shoulder, hip, knee, and finger joints
- Identify specific neurovascular complications associated with each common dislocation
- Outline the principles and sequence of closed reduction for shoulder, hip, knee, and finger dislocations
- Recognise the indications for open reduction versus closed reduction in joint dislocations
- Describe the role of a team member in assisting with closed reduction of common joint dislocations under supervision
INSTRUCTIONS
Joint dislocations are painful, distressing injuries that require prompt recognition and timely reduction to prevent neurovascular complications and avascular necrosis. As a final-year student and future house officer, you will be expected to recognise dislocations on clinical examination and plain radiograph, understand which nerve or vessel is at risk with each injury, and assist in the reduction procedure. This module covers the four most clinically important sites: shoulder (the commonest dislocation in adults), hip (the highest-stakes due to avascular necrosis risk), knee (the highest neurovascular risk), and finger joints (the most frequent in sport and casualty).
References
- Maheshwari's Essential Orthopaedics, Chapter 7 — Dislocations of the Upper Limb; Chapter 8 — Dislocations of the Lower Limb (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Chapter 11 — Shoulder and Upper Arm; Chapter 19 — Hip (textbook)
- Ebnezar's Textbook of Orthopaedics, Chapter 24 — Dislocations and Ligamentous Injuries (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 25-year-old footballer is brought into casualty holding his right arm in slight abduction and external rotation, supported by his left hand. He cannot bring the arm to his side. His shoulder contour is flattened, with a visible hollow beneath the acromion. He is in severe pain. The X-ray confirms an anterior dislocation of the glenohumeral joint. Before you attempt reduction, you need to know: which nerve lies directly against the surgical neck of the humerus and is at risk? What does that nerve supply? And how will you test it BEFORE and AFTER reduction? Getting these three answers right takes ninety seconds and is the difference between a correctly managed case and an unnoticed neurological injury.
WHY THIS MATTERS
Joint dislocations are among the most common reasons for casualty attendance in orthopaedics. Shoulder dislocations affect young active adults and the elderly (from falls). Hip dislocations occur in road traffic accidents and have a narrow time window for reduction — avascular necrosis of the femoral head risk rises steeply beyond 6 hours. Knee dislocations are limb-threatening emergencies with popliteal artery injury in up to 30–40% of cases. Finger dislocations are the most common sports injury presenting to any doctor. In all cases, neurovascular assessment before and after reduction is a non-negotiable standard of care.
RECALL
Before proceeding, recall:
- The anatomy of the glenohumeral joint: glenoid (shallow, pear-shaped), reinforced by the glenoid labrum, rotator cuff, and capsule; the axillary nerve wraps around the surgical neck of the humerus
- The anatomy of the hip joint: deep ball-and-socket joint; the sciatic nerve runs posterior to the hip joint and is at risk in posterior dislocation
- The two basic types of dislocation (anterior/posterior) and how the mechanism of injury determines direction
- The key principle: a dislocation must have neurovascular assessment BEFORE and AFTER reduction — before because the injury may have caused a deficit; after because the reduction manoeuvre itself can trap a nerve
- The concept of avascular necrosis (AVN): disruption of blood supply to the femoral head after hip dislocation; risk rises sharply if reduction is delayed beyond 6 hours
Clinical Indication and Relevance of Common Joint Dislocations
Shoulder dislocation is the most common major joint dislocation in adults, accounting for approximately 50% of all large joint dislocations. The glenohumeral joint sacrifices stability for mobility — its wide range of motion is achieved at the cost of a shallow glenoid with minimal bony constraint. The shoulder relies primarily on soft tissue structures (rotator cuff, glenoid labrum, capsule, ligaments) for stability, making it inherently vulnerable to dislocation under high-energy or repetitive loading conditions. Understanding the mechanism and direction of each dislocation directly determines the neurovascular structure at risk, the imaging views required, and the reduction technique selected.
Hip dislocation requires high-energy trauma in young adults — classically the 'dashboard injury' in road traffic collisions, where an axial force is transmitted through a flexed, adducted hip. It is an orthopaedic emergency because the femoral head's blood supply is disrupted from the moment of dislocation, and every minute of delay increases the risk of avascular necrosis. Knee dislocation involves multi-ligamentous disruption and threatens the limb through popliteal artery injury. Finger dislocations — particularly of the proximal interphalangeal joint — are the most frequent joint injuries seen in casualty and sports medicine.
Clinical relevance of each dislocation:
- Shoulder: 95% anterior; recurrence very common in young patients (>90% if age <20); axillary nerve at risk
- Hip: posterior (90%) from dashboard mechanism; AVN risk if reduction delayed beyond 6 hours; sciatic/peroneal nerve at risk
- Knee: multi-ligamentous; popliteal artery injury 30–40%; common peroneal nerve injury 25%; ABI must be measured
- Finger PIP: commonest joint dislocation in sport; volar plate avulsion; digital block + traction reduction
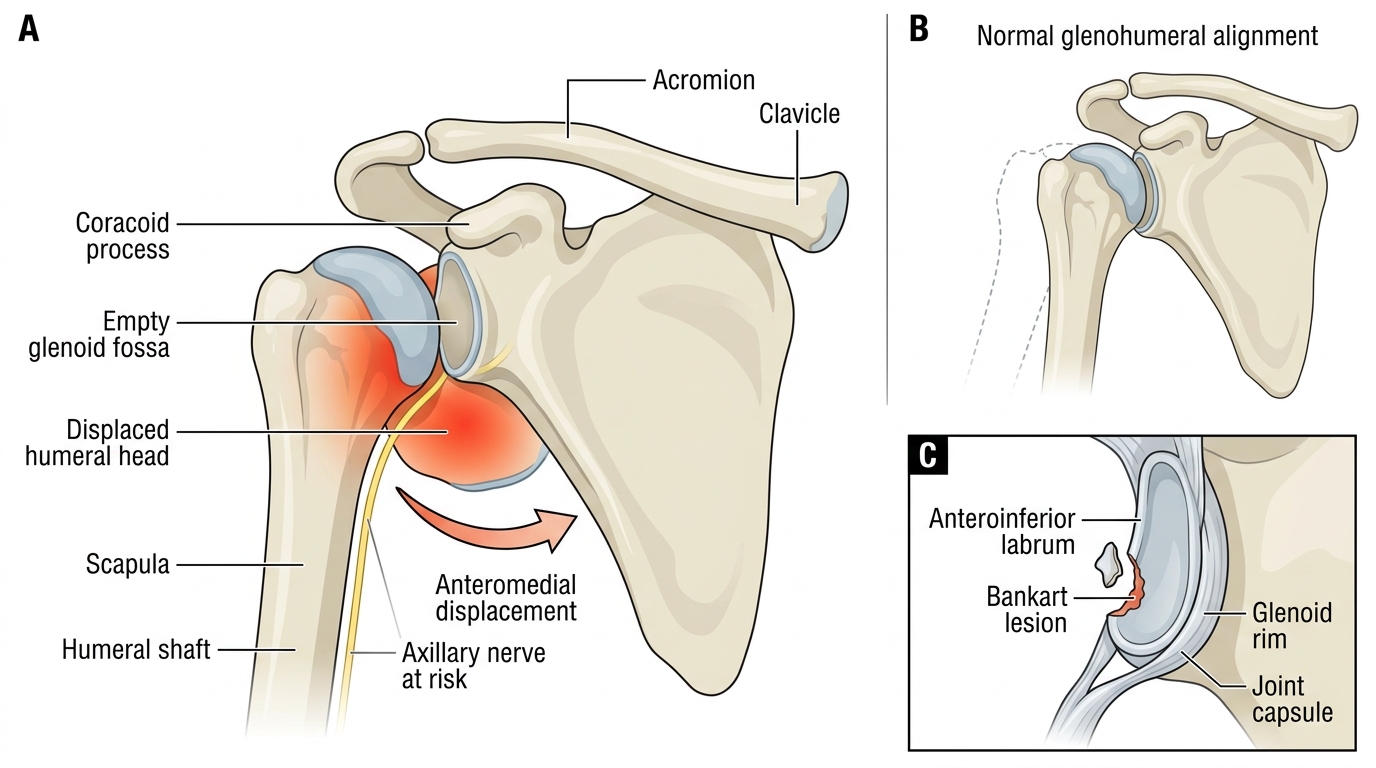
Anterior Glenohumeral Dislocation with Bankart Lesion
Anatomy and Governing Principles: Nerve–Joint Pairings
Each commonly dislocated joint has a specific nerve and vascular structure at risk, determined by the anatomical relationship between that structure and the joint capsule. Memorising these pairings is not mere factual recall — it is the foundation for the pre-reduction and post-reduction neurovascular assessment that constitutes the clinical standard of care. The examination is quick (under two minutes per joint) but legally and clinically critical: a deficit missed before reduction may be attributed to the reduction manoeuvre, and a new deficit after reduction may represent nerve entrapment requiring urgent surgery.
Shoulder — axillary nerve (C5, C6): the axillary nerve exits the posterior cord of the brachial plexus and wraps directly around the surgical neck of the humerus in the quadrilateral space. In anterior dislocation, the humeral head displaces inferoanteriorly, tenting the axillary nerve. Motor supply: deltoid (shoulder abduction). Sensory supply: lateral deltoid skin (the 'regimental badge area'). Test: light touch on the lateral deltoid + attempt at deltoid contraction against resistance.
Hip — sciatic nerve, common peroneal division: the sciatic nerve runs posterior to the hip capsule and is stretched or compressed in 10–14% of posterior dislocations. The common peroneal division (more tightly tethered) is most vulnerable. Motor deficit: foot drop (weakness of dorsiflexion and eversion). Sensory deficit: dorsum of foot and first web space.
Knee — popliteal artery and common peroneal nerve: the popliteal artery is tethered at the adductor hiatus proximally and the soleal arch distally, making it susceptible to stretch injury with knee dislocation. The common peroneal nerve wraps around the fibular neck and is stretched in lateral displacement. ABI must be measured — ABI <0.9 mandates CT angiography regardless of palpable pulse.
Finger PIP — digital nerves and vascular bundle: radial and ulnar digital nerves and arteries run on either side of the phalanx and may be compressed by dislocated bone. Test: two-point discrimination on each side of the fingertip.
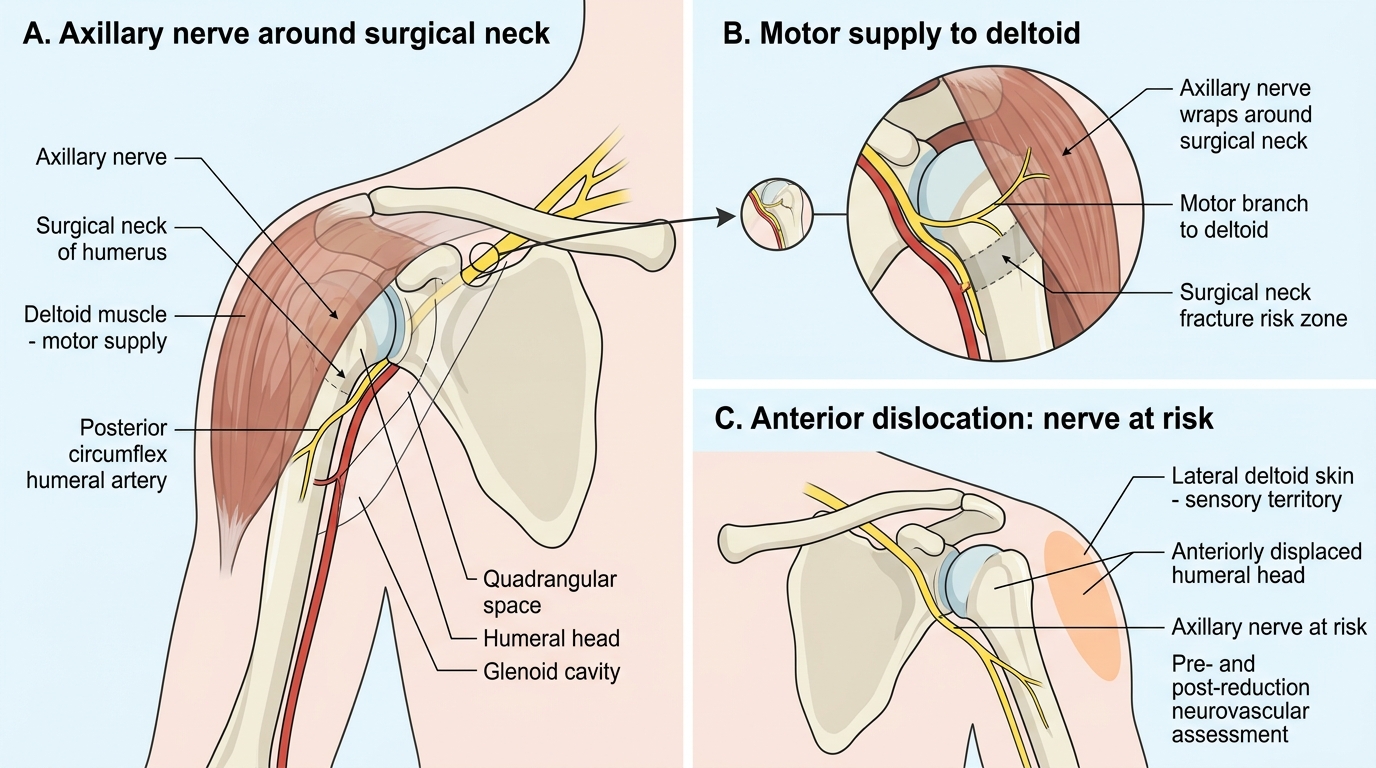
Axillary Nerve at the Surgical Neck of Humerus
Reduction Techniques: Shoulder, Hip, Knee, and Finger
Provided image
Closed reduction of joint dislocations should be performed as promptly as feasible after adequate analgesia and muscle relaxation. Pain and muscle spasm are the two physical barriers to reduction — attempts without adequate analgesia are more painful, risk iatrogenic fracture, and are less likely to succeed. The selection of technique is determined by the joint involved, the direction of dislocation, the patient's body habitus, and the available personnel and anaesthetic support. The general sequence for any reduction is: consent and explanation → analgesia/sedation → pre-reduction neurovascular assessment → reduction → post-reduction neurovascular assessment → confirmatory X-ray. This sequence must never be abbreviated regardless of urgency; a missed pre-reduction neurological deficit is a medicolegal hazard that cannot be retrospectively attributed to the injury rather than the procedure.
Shoulder reduction techniques (anterior dislocation):
1. Stimson's gravity technique: patient prone, arm hanging over table edge, 5–10 kg weight at wrist; shoulder muscles fatigue over 20–30 minutes allowing gradual reduction. Gentlest technique; no assistant needed.
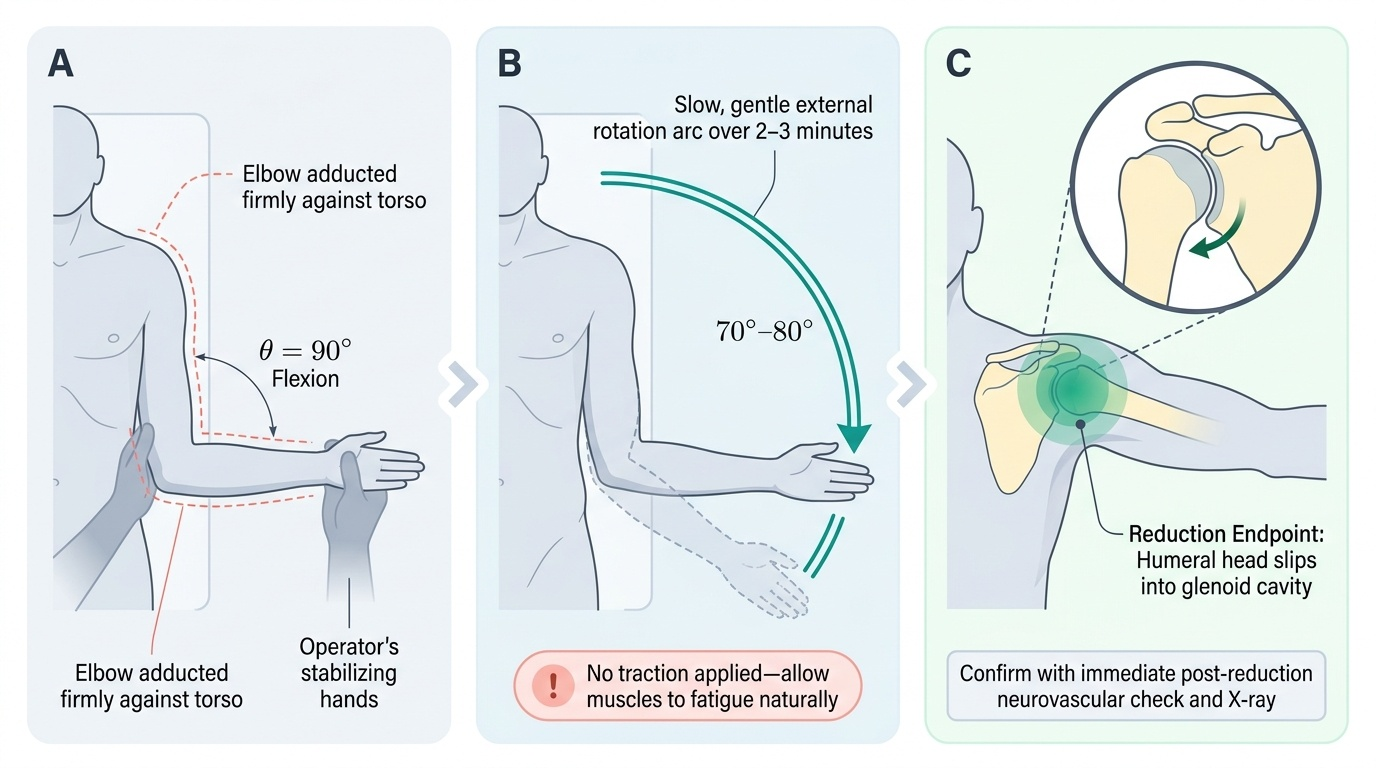
2. External rotation technique: patient seated or supine, elbow at 90° flexion; arm gently and slowly externally rotated with the elbow against the side until the head reduces with internal rotation and adduction. Very gentle; preferred in the elderly.
3. Hippocratic (traction-countertraction): sheet around the thorax (held by assistant as countertraction); operator applies steady longitudinal traction in slight abduction and external rotation. Effective but requires trained assistant.
4. Kocher's technique (levering): now largely avoided due to iatrogenic fracture risk in osteoporotic patients.
Hip reduction (posterior dislocation — requires general or spinal anaesthesia):
- Stimson's technique (hip): patient prone, hip at table edge, knee flexed 90°; assistant stabilises pelvis; operator applies downward traction on the knee with gentle internal/external rotation.
- Allis technique (supine): operator applies upward longitudinal traction on the flexed hip and knee while assistant presses down on iliac crests to stabilise the pelvis; hip is adducted then abducted to guide the head over the posterior rim.
Knee dislocation: longitudinal traction with correction of displacement under anaesthesia; avoid hyperextension during reduction.
Finger PIP dislocation: digital block (ring block at base or web-space block with 1% lignocaine); longitudinal traction with initial hyperextension to disengage the volar plate, then flexion to reduce.
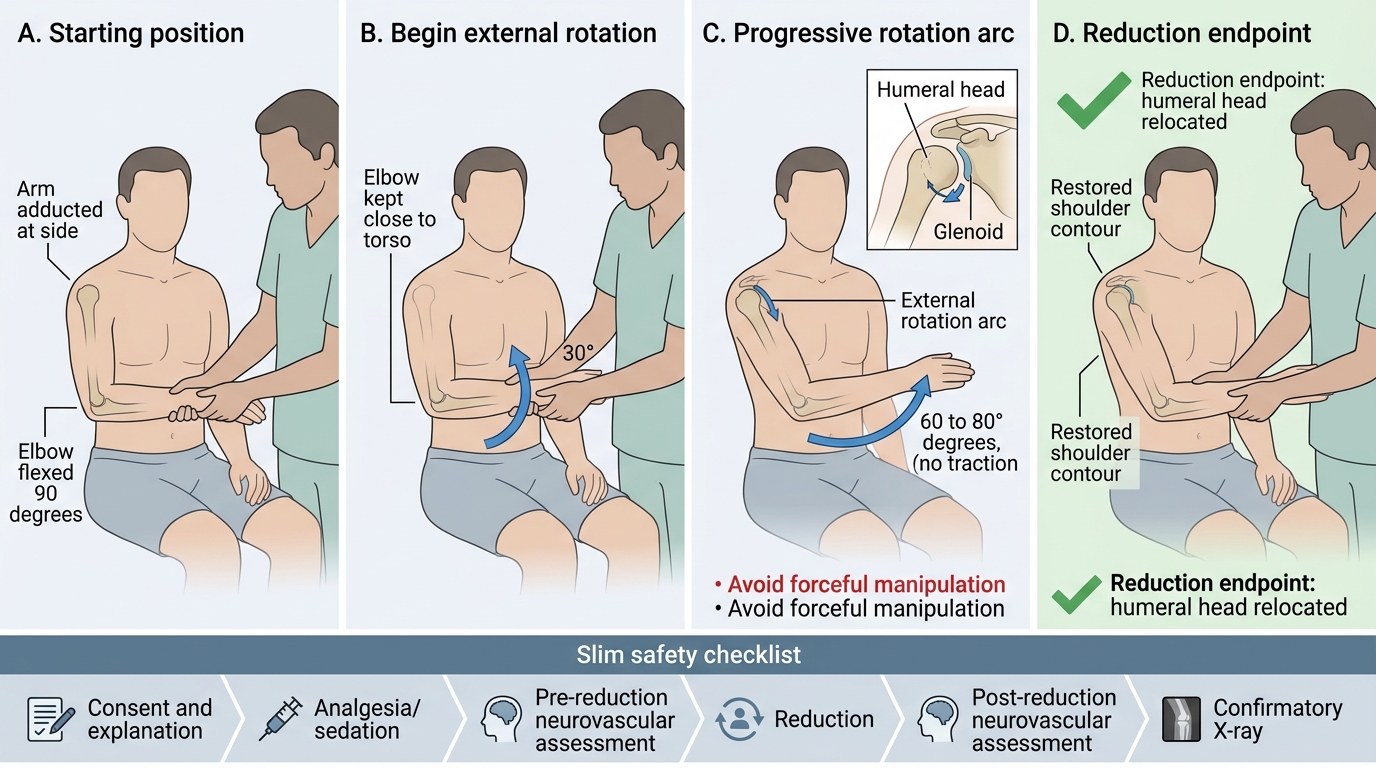
External Rotation Method for Anterior Shoulder Reduction
SELF-CHECK
After a successful closed reduction of an anterior shoulder dislocation, the patient complains of numbness over the lateral deltoid skin. Which nerve is affected, and what clinical test confirms its motor function?
A. Radial nerve — check wrist extension
B. Axillary nerve — check deltoid contraction (abduction against resistance) and sensation over the lateral deltoid (regimental badge area)
C. Musculocutaneous nerve — check elbow flexion strength
D. Suprascapular nerve — check external rotation strength
Reveal Answer
Answer: B. Axillary nerve — check deltoid contraction (abduction against resistance) and sensation over the lateral deltoid (regimental badge area)
The axillary nerve (C5, C6) runs around the surgical neck of the humerus and is the nerve most commonly injured in shoulder dislocation. Its motor supply is the deltoid (shoulder abduction) and its sensory territory is the lateral deltoid skin (regimental badge area). Numbness here after reduction confirms axillary neuropraxia. The radial nerve supplies wrist extension; the musculocutaneous supplies elbow flexion; the suprascapular supplies external rotation. Axillary neuropraxia after reduction usually recovers within 3–6 months.