Page 13 of 26
OR1.4-5 | Common Joint Dislocation Recognition and Reduction Assistance — SDL Guide (Part 2)
Interpretation of Post-Reduction Findings
The post-reduction assessment is as important as the pre-reduction baseline, and its three components — radiological confirmation, neurovascular re-examination, and functional assessment — must each be formally documented. A clinician who confirms reduction only radiologically but does not re-examine the neurovascular status has completed only part of the clinical duty. Each component may reveal complications that require further intervention, and the documentation of the pre-reduction baseline is what allows attribution: was this deficit present before the reduction, or did it arise during the manoeuvre? The practical implication of this is that a new post-reduction deficit with a blank pre-reduction record cannot be attributed to the dislocation itself; it becomes legally and clinically ambiguous. Thorough documentation before the procedure protects both patient and clinician.
Radiological confirmation post-reduction:
- Shoulder: AP and axillary views; confirm concentric glenohumeral reduction, symmetric joint space, no new fracture; Hill-Sachs lesion and bony Bankart noted for follow-up planning
- Hip: AP pelvis and lateral hip views; confirm concentric femoral head position; CT pelvis mandated to detect intra-articular loose fragments and posterior acetabular wall fractures; Shenton's line should be restored
- Finger: AP and lateral views; confirm anatomical reduction, measure volar plate avulsion fragment size (>30–40% articular surface = surgical referral)
Neurovascular re-examination after reduction:
Any NEW deficit after reduction that was ABSENT before is a sign of nerve entrapment in the joint — the femoral head or humeral head may have trapped the nerve between bone and the acetabular/glenoid rim during the manoeuvre. This is an urgent indication for surgical exploration. A pre-existing deficit (present before reduction) is followed with serial neurological assessments — axillary neuropraxia recovers over 3–6 months; peroneal nerve injury after hip or knee dislocation has a more variable prognosis.
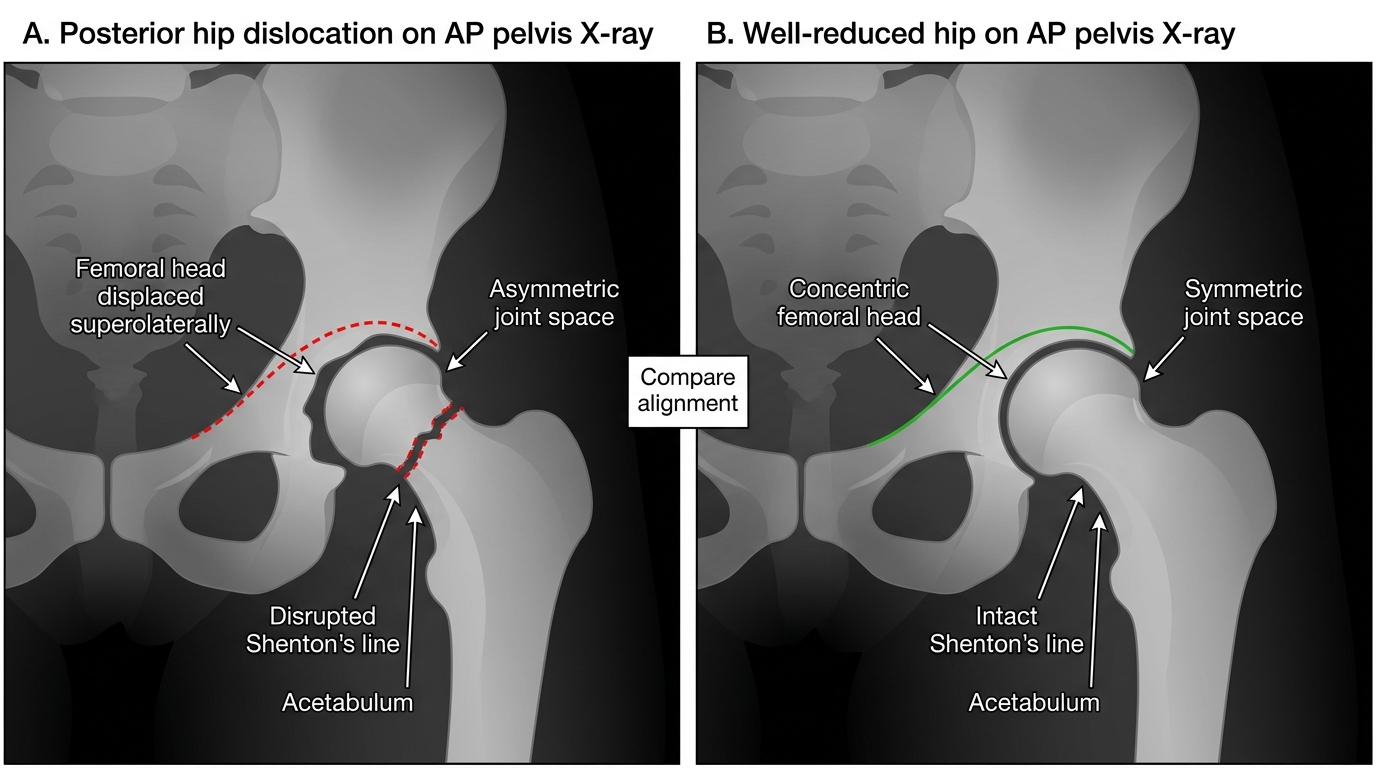
AP Pelvis: Posterior Hip Dislocation Versus Reduced Hip
Hip dislocation — additional post-reduction assessment:
- Arrange CT pelvis to detect posterior acetabular wall fractures (>40% wall involvement requires surgical fixation) and intra-articular loose bodies
- Persistent severe pain despite confirmed radiological reduction: suspect intra-articular fragment or early AVN — urgent MRI
- Inability to bear weight at 6 weeks: AVN surveillance with MRI (X-ray changes in AVN appear late, at 3–6 months)
Functional assessment: the patient should report partial pain relief after successful reduction. A patient in the same severe pain after confirmed radiological reduction may have an undetected intra-articular fracture or residual subluxation and requires further imaging.
Applied and Supervised Practice: Team Member Role in Reduction
As a final-year student and future house officer, the NMC 2024 curriculum requires participation as a team member in closed reduction of common joint dislocations (OR1.5). This supervised participation involves specific defined roles that contribute directly to patient safety — it is not passive observation. Understanding these roles, and the rationale behind each step, allows you to contribute meaningfully and to recognise when a step is being missed. The skills practised here — neurovascular documentation, countertraction, procedural monitoring, and post-procedure note writing — are directly transferable to surgical and emergency medicine postings. A team member who has internalised this framework can also serve as a safety check: if the operator is about to proceed without a pre-reduction neurovascular assessment, the team member who knows this step is mandatory can prompt for it without hesitation.
Role during shoulder dislocation reduction:
- Assist with patient positioning (prone for Stimson's gravity technique; supine for traction-countertraction; seated for external rotation technique)
- During Hippocratic technique: hold the countertraction sheet firmly around the thorax; maintain steady firm resistance while the operator applies traction — do NOT jerk or suddenly release; the reduction should be a smooth, gradual process
- Monitor vital signs and consciousness level during procedural sedation (observe for apnoea, hypotension, or loss of protective airway reflexes)
- Document the pre-reduction neurovascular assessment in the clinical notes before the procedure begins — this protects both patient and doctor
- After reduction: prepare post-reduction X-ray request, label it with clinical indication and which views are needed
Role during hip dislocation reduction (performed under general or spinal anaesthesia in theatre):
- Stabilise the pelvis: stand on the same side as the operator and place both hands firmly on the ipsilateral iliac crest, pressing downward with your full body weight to counteract the operator's upward traction on the hip
- Maintain spinal precautions: hip dislocations in RTA patients may have associated spinal injuries — do not allow uncontrolled axial loading of the spine during positioning or transfer
- Post-reduction: arrange CT pelvis request urgently; monitor for haemodynamic changes (rare vagal response during hip reduction)
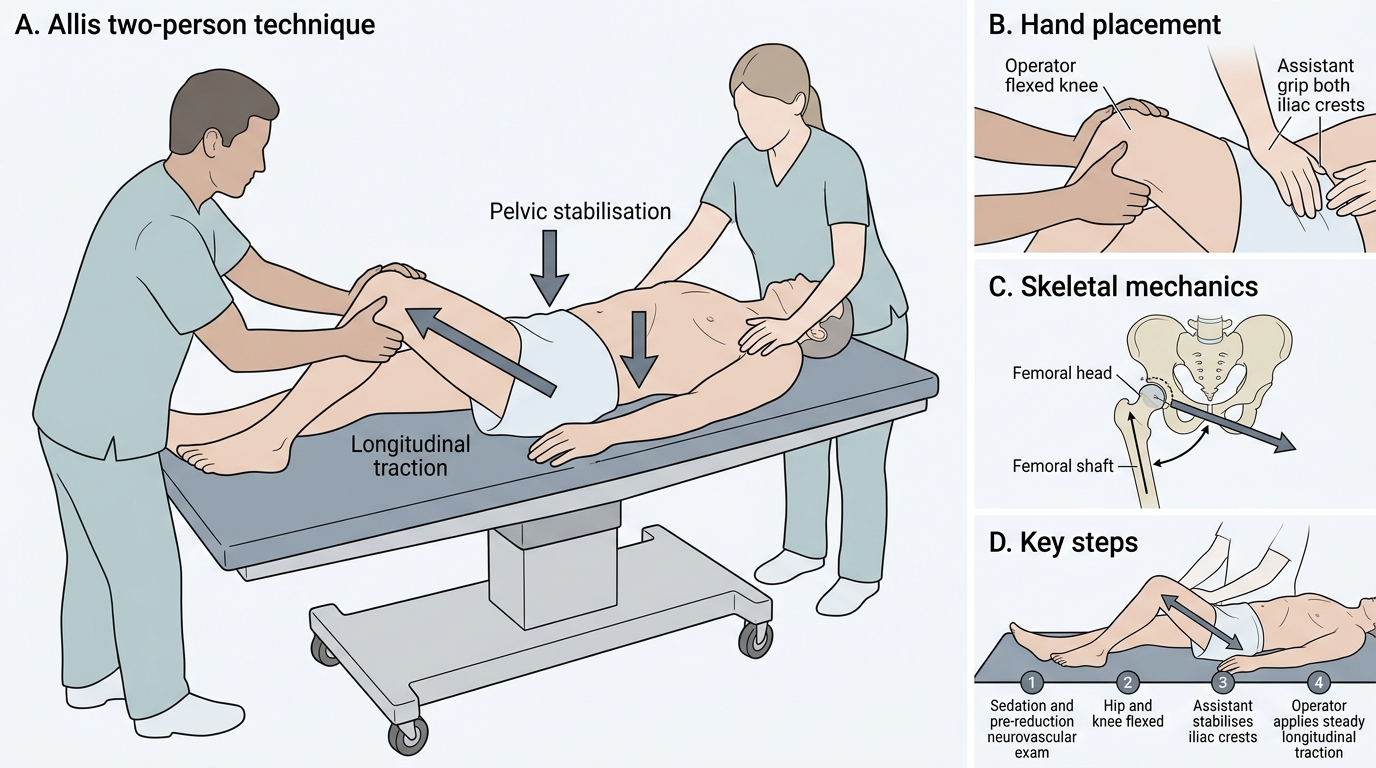
Allis Two-Person Closed Hip Reduction Technique
Universal documentation standard (ALL reductions):
1. Indication and mechanism of injury
2. Consent obtained (document patient's understanding)
3. Allergy status confirmed
4. Pre-reduction neurovascular status (written findings, not 'NVS intact')
5. Technique used, sedation agent and dose, number of attempts
6. Outcome (reduced/not reduced)
7. Post-reduction neurovascular status (written findings)
8. Post-reduction imaging review (state whether you personally viewed the X-ray and what it showed)
9. Disposition and follow-up plan
SELF-CHECK
A 35-year-old is brought in after a road traffic collision. The left hip is held in flexion, adduction, and internal rotation. Pre-reduction exam shows normal dorsiflexion and normal peroneal sensation. After reduction under general anaesthesia, the patient has new-onset foot drop and numbness over the dorsum of the foot. What is the most likely explanation and the immediate action?
A. Expected neuropraxia from the dislocation itself — observe and reassure
B. The common peroneal nerve was entrapped in the joint during reduction — urgent surgical exploration is indicated
C. The sciatic nerve was already injured before reduction and the deficit was missed
D. General anaesthesia has temporarily weakened the muscles — recheck in 4 hours
Reveal Answer
Answer: B. The common peroneal nerve was entrapped in the joint during reduction — urgent surgical exploration is indicated
A NEW neurological deficit appearing AFTER reduction that was NOT present on the documented pre-reduction assessment is a sign of nerve entrapment in the joint. The common peroneal division of the sciatic nerve may have been trapped between the femoral head and the acetabular rim during reduction. This is an urgent indication for surgical exploration before permanent damage occurs. Pre-reduction documentation (confirming normal dorsiflexion) is what establishes that this deficit is new — demonstrating exactly why pre-reduction neurovascular documentation is non-negotiable.
Self-Assessment: Dislocation Recognition and Management
Use these structured clinical scenarios to consolidate the four key domains of this module: recognition, nerve pairing, reduction technique selection, and post-reduction assessment. For each scenario, work through your response systematically before reading the guidance notes. The scenarios mirror the OSCE and viva format used in final examinations and should prepare you for real-time clinical decision-making during your surgical posting.
Scenario A — Shoulder: A 60-year-old woman falls on an outstretched hand and presents with a painful, swollen right shoulder held in slight internal rotation and forward flexion. There is a fullness posteriorly. The AP X-ray shows a 'lightbulb sign' — the humerus appears abnormally rounded. What type of dislocation is this, and what is the classic mechanism in an elderly patient? What additional X-ray view must you request? What nerve and vessel are at risk, and which demographic risk factor predisposes this patient to vascular injury?
Scenario B — Hip: A 40-year-old driver is brought in after a head-on collision. His right hip is held in 30° of flexion, adduction, and internal rotation. He has right foot drop. The X-ray shows posterior hip dislocation without acetabular fracture. How urgently must you reduce this hip and why? What does the foot drop tell you about the nerve involved and its territory? What is the post-reduction imaging protocol, and what structural complication does CT specifically seek?
Scenario C — Knee: A 25-year-old rugby player is tackled and sustains a high-energy knee injury. On arrival the knee is grossly swollen and lax in all planes. He is neurovascularly intact on first assessment. The ABI on the injured side is 0.78. What is the diagnosis, what is the significance of the ABI, and what is the mandatory next investigation? What is the timing imperative for this investigation?
After working through these scenarios, identify the one fact about each joint dislocation that you feel least confident about and return to the relevant section in this SDL before your next clinical session.
CLINICAL PEARL
The limb position is the diagnosis: in hip dislocation, the direction of dislocation determines limb posture and the nerve at risk — one glance tells you the anatomy. Posterior dislocation (90%): limb is flexed, adducted, internally rotated (head slipped out the back) → sciatic/peroneal nerve at risk posteriorly. Anterior dislocation: limb is abducted and externally rotated (head slipped out the front) → femoral nerve/vessels at risk. The same anatomical pattern-matching applies to shoulder dislocation: anterior displacement puts the axillary nerve (wrapping around the surgical neck) under tension — explaining why lateral deltoid numbness is so characteristic and why the regimental badge area is the sensory test target. These associations are not mnemonics — they reflect the physical anatomy of the nerve's path relative to the joint.