Page 9 of 26
OR1.3 | Soft Tissue Injury Assessment — SDL Guide
Learning Objectives
- Classify soft tissue injuries from contusion through crush injury and describe the pathophysiology of each
- Describe the aetiology, clinical features, and graded management of compartment syndrome
- Explain the Gustilo-Anderson classification of open fractures and the management priorities for each grade
- Outline the assessment and management of traumatic rhabdomyolysis including renal protection strategies
- Apply the principles of wound management including debridement timing, antibiotic choice, and closure options for open orthopaedic injuries
INSTRUCTIONS
Soft tissue injuries are the most commonly under-assessed component of musculoskeletal trauma. An orthopaedic surgeon who focuses exclusively on the bone and overlooks the surrounding muscle, fascia, nerves, and vessels will miss compartment syndrome, vascular injury, and degloving — all of which can cause limb loss or death. This module trains you to look beyond the fracture line and assess the soft tissue envelope systematically, using a structured clinical approach that is directly applicable to your casualty and orthopaedic postings.
References
- Maheshwari's Essential Orthopaedics, Chapter 3 — Injuries of Bones and Joints (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Chapter 22 — Principles of Fractures (textbook)
- Ebnezar's Textbook of Orthopaedics, Chapter 22 — Complications of Fractures and Dislocations (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 20-year-old motorcyclist is brought in after a collision. His X-ray shows a closed tibial shaft fracture. His bone looks straightforward on the film. But his leg is tense, shiny, and swollen. He rates his pain 9/10 and tells you it is made worse when you passively dorsiflex his foot. His pedal pulses are present and his capillary refill is 2 seconds. 'The pulses are fine,' the intern says. 'We can splint it and wait for the orthopaedic team in the morning.' You know that this patient has compartment syndrome — a surgical emergency — and that waiting until morning with a present pulse means waiting until the muscles are dead.
WHY THIS MATTERS
Soft tissue injury assessment is a core competency for any doctor working in a district hospital, emergency department, or primary care setting with limited specialist backup. Compartment syndrome missed for six hours causes irreversible Volkmann's ischaemic contracture. An open fracture inadequately cleaned and closed causes osteomyelitis and chronic non-union. A degloving injury misidentified as a bruise leads to skin necrosis, sepsis, and amputation. The skills in this module are not optional extras — they are threshold competencies that every MBBS graduate must possess before their first independent clinical shift.
RECALL
Before proceeding, briefly recall:
- The anatomy of the four compartments of the leg (anterior, lateral, deep posterior, superficial posterior) and the muscles within each
- The difference between arterial and venous pressure: arteries deliver oxygen under high pressure; compartment syndrome compresses veins first (reducing venous outflow), raising tissue pressure before arterial flow is affected
- The classification of fractures as closed versus open, and the significance of skin integrity
- Basic wound healing: primary (direct closure), secondary (granulation), and tertiary (delayed primary) intention
- The concept of rhabdomyolysis: muscle cell breakdown releasing myoglobin, which precipitates in renal tubules under acidic conditions
Classification and Pathophysiology of Soft Tissue Injuries
Soft tissue injuries in orthopaedic trauma encompass a spectrum from superficial contusion to full-thickness crush injury with muscle devitalisation. Understanding the pathophysiology of each type is essential for predicting complications, guiding investigation, and selecting management. The skin, subcutaneous fat, fascia, muscle, nerves, and vessels all have different vulnerabilities and healing capacities, and each may be involved to different degrees in the same injury.
Contusion (bruise): results from blunt force compressing soft tissue against underlying bone, rupturing small blood vessels without breaking the skin. The resulting haematoma causes swelling, tenderness, and discolouration. Simple contusions resolve with RICE (rest, ice, compression, elevation) within days to weeks. Large haematomas — particularly in the thigh — may organise into myositis ossificans (heterotopic bone formation within muscle), especially if repeatedly traumatised. A characteristic crescent of calcification on X-ray appearing 6–8 weeks after injury confirms the diagnosis.
Laceration: a wound in which the skin and underlying soft tissues are divided by sharp or blunt force. Sharp lacerations have clean edges and minimal surrounding tissue necrosis; blunt lacerations have irregular, crushed edges with surrounding devitalised tissue. The distinction matters for wound closure: clean sharp lacerations can be primarily sutured within 6–8 hours; irregular contaminated lacerations may require debridement and delayed closure.
Degloving injury: separation of skin and subcutaneous tissue from the underlying fascia, disrupting the perforating vessels that supply the skin. Two patterns are seen — open (skin is physically avulsed) and closed (Morel-Lavallée lesion: skin appears intact but has been detached from the deep fascia by shear forces, creating a haemolymphatic cavity). Closed degloving injuries are notoriously missed because the skin looks unbroken and bruised rather than avulsed. The overlying skin is at high risk of necrosis because its blood supply is disrupted.
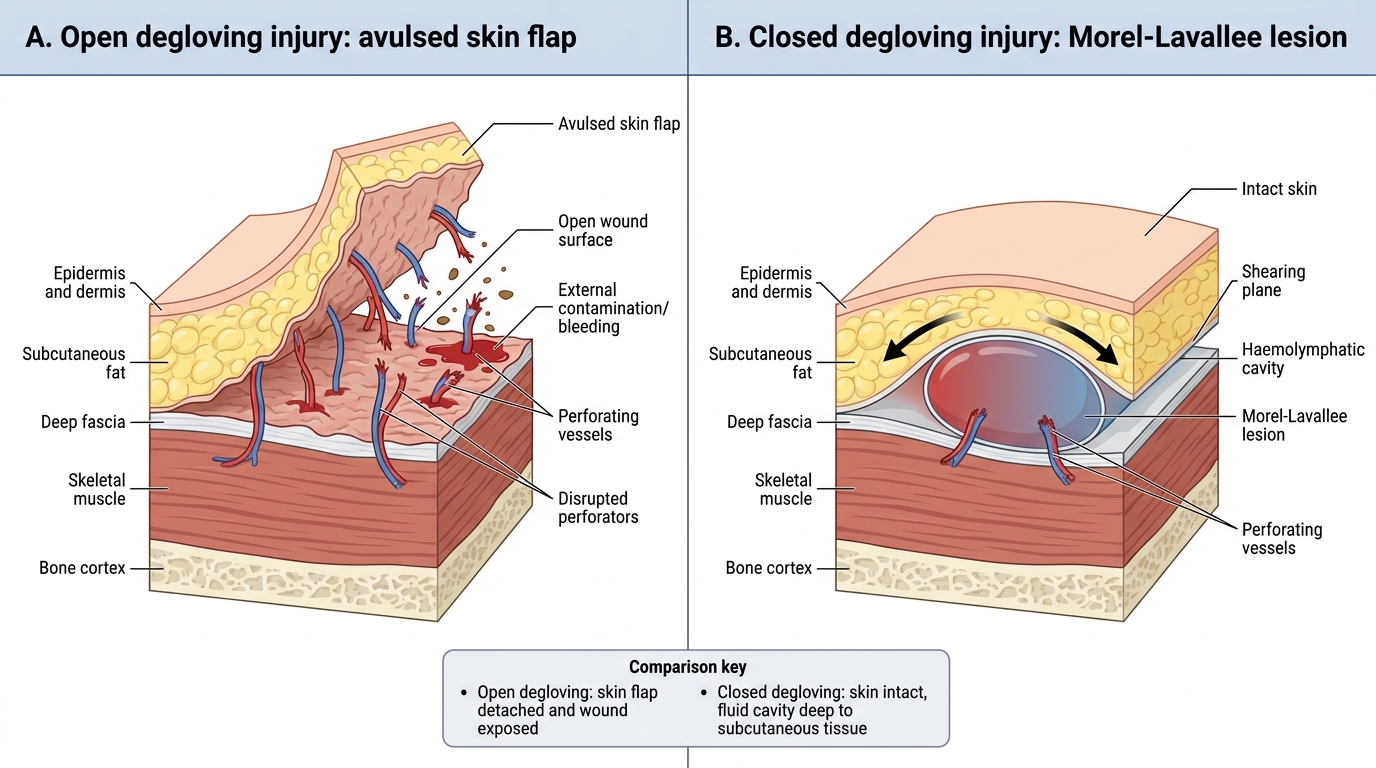
Open versus Closed Degloving Injury
Crush injury: prolonged compressive force causes ischaemia and direct destruction of muscle cells, releasing myoglobin, potassium, phosphate, and creatine kinase (CK) into the systemic circulation. The resulting rhabdomyolysis syndrome carries risks of acute kidney injury (myoglobin casts tubular necrosis), hyperkalaemia (from cell lysis, causing fatal arrhythmias), and metabolic acidosis. Clinically, the patient may have swollen, tense, dusky compartments with haemoglobinuria (dark 'cola-coloured' urine — actually myoglobinuria). CK >5,000 U/L indicates significant muscle injury; CK >10,000 U/L or myoglobinuria mandates aggressive IV fluid therapy and urinary alkalinisation.
Avulsion injury: a mechanism where muscle or tendon attached to bone pulls off a fragment of bone (bony avulsion) or separates from the musculotendinous junction (soft tissue avulsion). Common orthopaedic examples include avulsion of the anterior superior iliac spine (sartorius), anterior inferior iliac spine (rectus femoris), ischial tuberosity (hamstrings), and fifth metatarsal base (peroneus brevis — often confused with a lateral ankle sprain on X-ray).
Compartment Syndrome: Recognition and Emergency Management
Compartment syndrome is the single most important acute soft tissue complication in orthopaedic trauma. It occurs when pressure within an osteofascial compartment rises to a level that impairs capillary perfusion, causing ischaemia of the muscles and nerves within. If not decompressed within 6 hours, irreversible ischaemic contracture (Volkmann's in the forearm; similar sequelae in the leg) results. The key insight is that this is a clinical diagnosis, not a radiological one, and the treatment is surgical (fasciotomy) — not a scan or a specialist referral.
Most common sites: the four compartments of the leg (anterior compartment most vulnerable), the volar and dorsal compartments of the forearm (Volkmann's), the intrinsic compartments of the hand, the gluteal region, and the thigh.
Causes: fractures (especially tibial shaft, distal radius, supracondylar humerus), crush injuries, circumferential burns, tight plaster casts, reperfusion after vascular repair, snake envenomation, and bleeding disorders.
Clinical features — the 6 P's (in order of appearance):
1. Pain — out of proportion to the injury; this is the EARLIEST and most sensitive sign. The pain is severe, unrelenting, and not controlled by standard analgesia doses.
2. Pain on passive stretch — passive dorsiflexion of the foot (testing anterior and deep posterior compartments of the leg) or passive finger extension (testing forearm compartments) reproduces or worsens the compartment pain. This is the most reliable early clinical test.
3. Paraesthesia — tingling, numbness in the distribution of the nerves running through the affected compartment (e.g., first web space numbness in anterior compartment syndrome of the leg = deep peroneal nerve)
4. Pallor — late sign; the skin overlying a tight compartment may become pale or mottled
5. Paralysis — weakness or inability to move muscles within the compartment; a late sign indicating established ischaemia
6. Pulselessness — the LATEST sign; compartment syndrome compresses veins and capillaries first, well before arterial pressure is overcome. A present pulse does NOT exclude compartment syndrome. This is the most important trap in clinical practice.
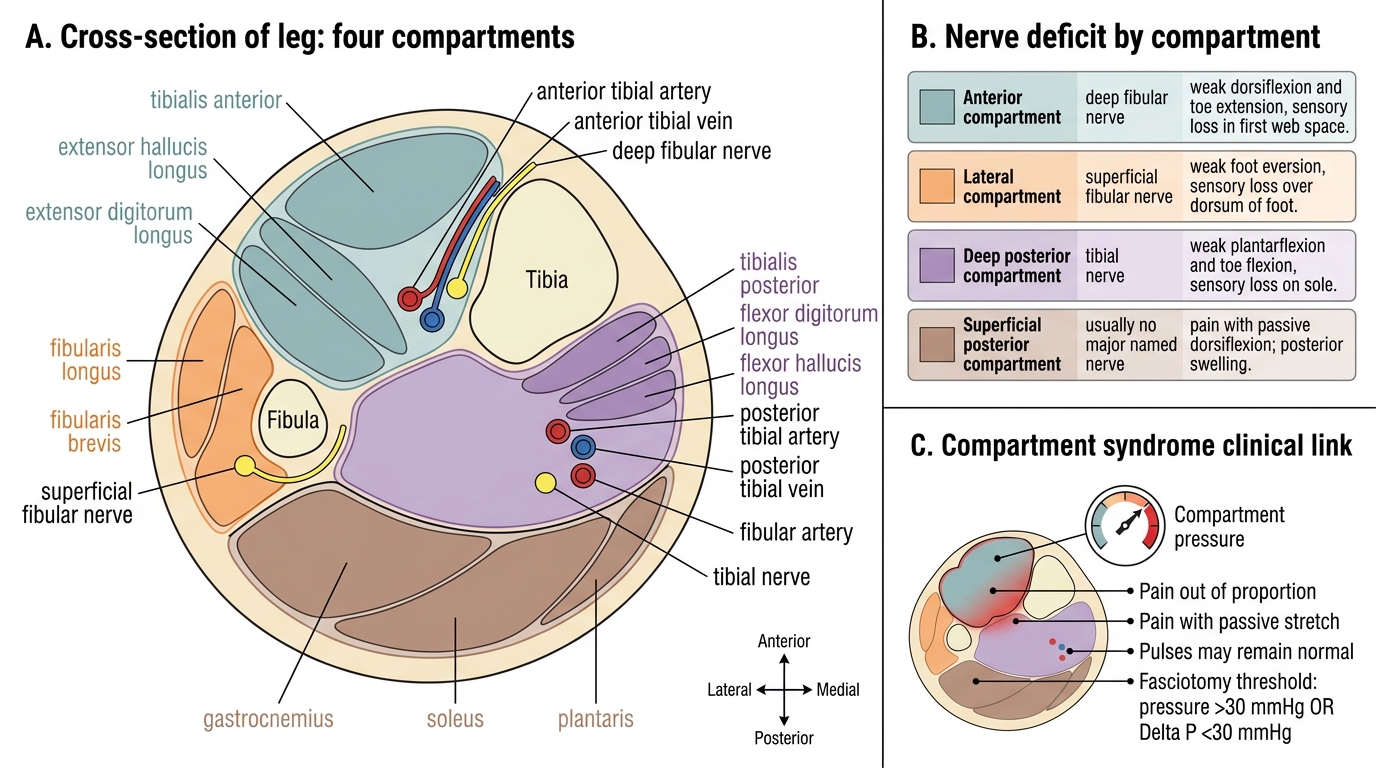
Leg Compartments and Nerve Deficits
Compartment pressure measurement:
When the clinical diagnosis is uncertain (e.g., unconscious patient, sedated, unreliable history), compartment pressure can be measured with a Stryker device, arterial line manometer, or slit catheter. The threshold for fasciotomy is:
- Absolute pressure >30 mmHg, OR
- Delta P (ΔP) <30 mmHg, where ΔP = diastolic BP minus compartment pressure. ΔP <30 mmHg means capillary perfusion pressure is critically reduced and fasciotomy is indicated regardless of the absolute number.
Emergency fasciotomy: the definitive treatment. All four compartments of the leg are released through two longitudinal incisions (lateral for anterior + lateral compartments; medial for superficial + deep posterior). The wounds are left open, dressed with moist dressings, and skin-grafted or closed secondarily at 48–72 hours after swelling resolves. Do NOT perform fasciotomy through stab incisions — the entire compartment length must be decompressed.
SELF-CHECK
A 24-year-old man has a tibial shaft fracture after a road traffic collision. He is in severe pain (9/10), and passive dorsiflexion of the ankle markedly worsens his pain. His pedal pulses are 2+ and capillary refill is 2 seconds. A nurse says 'the pulses are fine — it's probably just the fracture pain.' What is the correct action?
A. Reassure and observe — present pulses rule out compartment syndrome
B. Measure serum CK to confirm muscle injury before acting
C. Treat as compartment syndrome — request urgent fasciotomy based on clinical features, especially pain on passive stretch
D. Apply a tight compression bandage to reduce swelling
Reveal Answer
Answer: C. Treat as compartment syndrome — request urgent fasciotomy based on clinical features, especially pain on passive stretch
Present pulses do NOT exclude compartment syndrome. Arterial pressure is overcome only very late in the syndrome — by the time pulselessness appears, the muscles are irreversibly ischaemic. Pain on passive stretch is the earliest and most reliable clinical sign, and combined with pain out of proportion to the injury, it constitutes a clinical diagnosis requiring immediate fasciotomy. Waiting for CK results or observing while the pulse is present is a dangerous error that will lead to permanent disability.
Open Fractures: Gustilo-Anderson Classification and Management
An open fracture (compound fracture) is one in which the bone communicates with the external environment through a break in the overlying skin. Even a small puncture wound over a fracture represents direct communication between bone and the environment, creating a high risk of infection, osteomyelitis, and non-union if not managed correctly. Open fractures represent orthopaedic emergencies — every hour of delay in antibiotic administration and debridement increases the infection risk. The historical distinction between 'compound' and 'complicated' fractures is now replaced by the Gustilo-Anderson grading, which directly links wound severity to management pathway and expected outcomes, making it a practical clinical decision tool rather than a descriptive label.
The Gustilo-Anderson classification is the standard system for grading open fractures based on wound size, contamination, and soft tissue involvement. Each grade carries a different infection risk and management pathway:
| Grade | Wound | Contamination | Soft tissue | Infection risk | Key feature |
|---|---|---|---|---|---|
| I | <1 cm | Minimal | Adequate coverage | ~2% | Low-energy mechanism; wound from within |
| II | 1–10 cm | Moderate | Adequate coverage | ~5–10% | Higher energy; some muscle damage |
| IIIA | >10 cm | Extensive | Adequate coverage possible | ~10–20% | High energy; soft tissue can cover bone |
| IIIB | >10 cm | Extensive | Inadequate; periosteal stripping | ~20–50% | Needs flap reconstruction |
| IIIC | Any | Extensive | Arterial injury requiring repair | ~25–50%+ | Vascular repair in addition to bone/soft tissue |
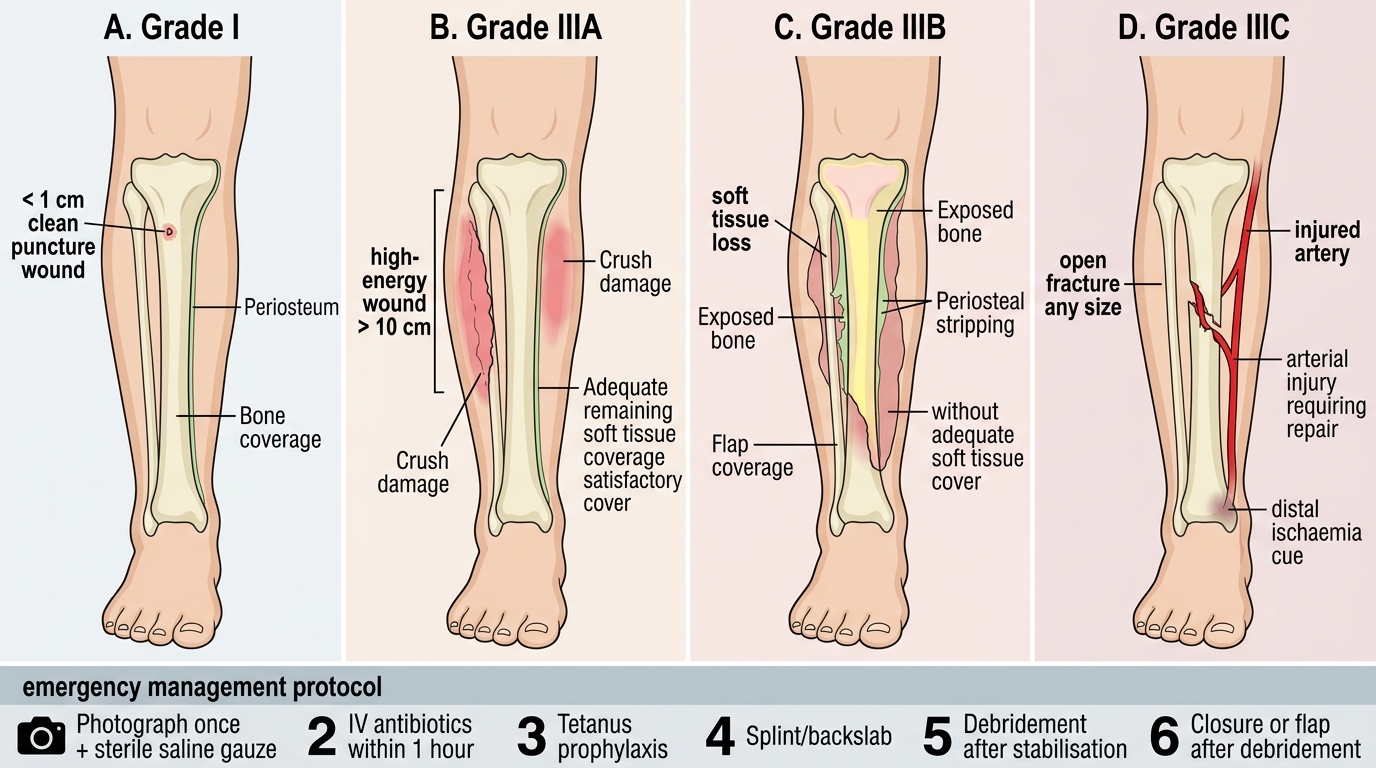
Gustilo-Anderson Open Fracture Grades I, IIIA, IIIB, and IIIC
Emergency management protocol for all open fractures:
1. Photograph the wound once, then apply a saline-soaked sterile gauze dressing — do NOT repeatedly undress the wound to 'inspect' it (each undressing introduces new organisms)
2. Intravenous antibiotics within 1 hour of injury — this is the most time-critical intervention, more so than the timing of surgery. Recommended regimens:
- Grade I and II: co-amoxiclav 1.2 g IV 8-hourly, or cephalosporin (cefazolin 1 g IV 8-hourly)
- Grade III: add gentamicin 5 mg/kg IV daily for gram-negative cover
- Farm/soil/faecal contamination: add metronidazole 500 mg IV 8-hourly for anaerobic cover
- Penicillin allergy: clindamycin + gentamicin
3. Tetanus prophylaxis: toxoid (if not up to date) and immunoglobulin (if unimmunised)
4. Splinting: immobilise the fracture with a backslab; reduces pain, haemorrhage, and further soft tissue injury
5. Surgical debridement: the old '6-hour rule' (mandatory debridement within 6 hours) is now superseded — the current evidence supports debridement 'as soon as feasible after haemodynamic stabilisation,' typically within 12–24 hours for Grade I/II and as early as possible for Grade III. Antibiotics bridge the delay.
6. Wound management after debridement:
- Grade I/II: may be primarily closed at time of debridement if clean after washout
- Grade IIIA: delayed primary closure at 48–72 hours
- Grade IIIB: requires plastic surgery flap reconstruction (local or free flap)
- Grade IIIC: vascular surgery for arterial repair before or simultaneous with orthopaedic fixation
Definitive fracture fixation follows the principles of damage control orthopaedics: temporary external fixation for initial stabilisation, with conversion to intramedullary nail or internal fixation once soft tissue healing is underway and infection risk is controlled.