Page 10 of 26
OR1.3 | Soft Tissue Injury Assessment — SDL Guide (Part 2)
Traumatic Rhabdomyolysis: Assessment and Renal Protection
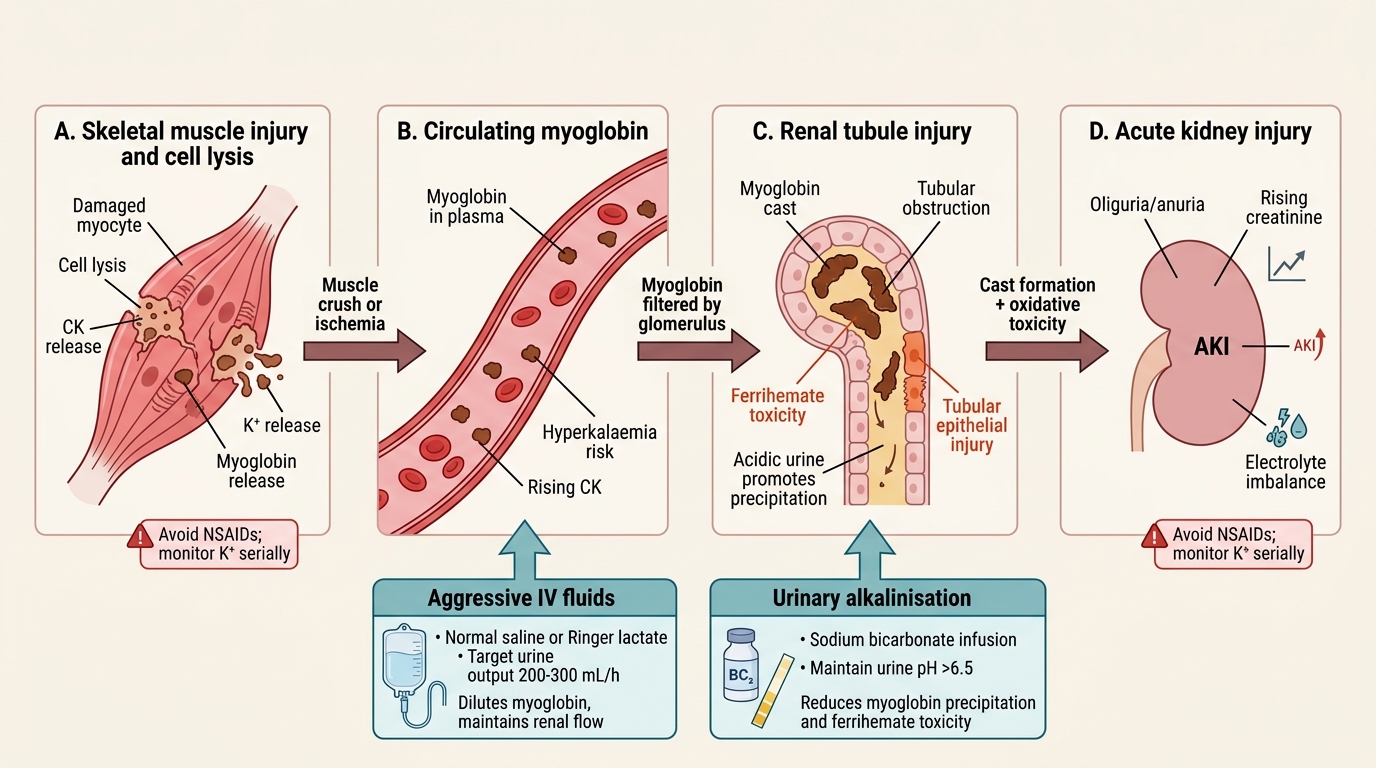
Rhabdomyolysis is the breakdown of striated muscle cells, releasing intracellular contents — primarily myoglobin, potassium, phosphate, creatine kinase (CK), and uric acid — into the bloodstream. In orthopaedic trauma, it occurs with crush injuries, prolonged compartment syndrome, electrical injuries, and severe soft tissue trauma. The clinical spectrum ranges from asymptomatic CK elevation to life-threatening acute kidney injury (AKI) and fatal hyperkalaemia.
Myoglobin is directly nephrotoxic in two ways: (1) it precipitates in acidic renal tubules, causing physical obstruction (myoglobin casts), and (2) it is converted to ferrihemate at acid pH, which directly injures tubular epithelial cells. Both mechanisms are worsened by dehydration, which concentrates myoglobin in the tubular lumen and worsens acidification. This explains the cornerstone of management: aggressive IV fluid therapy to maintain high urine flow and alkaline urine.
Rhabdomyolysis-Induced Acute Kidney Injury
Clinical features of rhabdomyolysis:
- Muscle swelling and tenderness at the injured site — tense, woody-hard muscles in affected compartments
- Dark brown or 'cola-coloured' urine — myoglobinuria; a urine dipstick tests positive for 'blood' (cross-reacts with myoglobin) but microscopy shows no red blood cells
- Systemic features: nausea, malaise, oliguria progressing to anuria
- Biochemical: CK markedly elevated (>1,000 U/L is abnormal; >10,000 U/L indicates severe injury); creatinine rising; hyperkalaemia; hyperphosphataemia; hypocalcaemia (calcium sequestered in damaged muscle)
Management principles:
1. Aggressive IV fluid therapy: Ringer's lactate or normal saline at rates sufficient to achieve urine output 200–300 mL/h (3 mL/kg/h) until urine clears and CK is trending down. This typically requires 6–10 L in the first 24 hours in severe cases.
2. Urinary alkalinisation: sodium bicarbonate infusion to maintain urine pH >6.5 reduces myoglobin precipitation and ferrihemate toxicity. Add 50–100 mEq sodium bicarbonate to each litre of IV fluid.
3. Monitor electrolytes serially: hyperkalaemia (K+ >6 mmol/L) is immediately life-threatening — treat with calcium gluconate (membrane stabilisation), insulin-dextrose, and sodium bicarbonate
4. Avoid NSAIDs and nephrotoxic agents: paracetamol for analgesia; avoid ibuprofen, ketorolac, gentamicin (additive nephrotoxicity)
5. Fasciotomy if compartment syndrome coexists — releasing the compartment reduces ongoing muscle necrosis and the myoglobin load
6. Renal replacement therapy (haemodialysis): if AKI is established and not responding to fluid therapy; removes potassium and fluid overload
| Severity | CK (U/L) | Urine | Management |
|---|---|---|---|
| Mild | 1,000–5,000 | Clear or slightly discoloured | Oral hydration + monitor |
| Moderate | 5,000–10,000 | Tea/brown coloured | IV fluids, urinary alkalinisation, serial K+ |
| Severe | >10,000 | Cola/maroon | Aggressive IV fluids (200–300 mL/h target), ICU, consider dialysis |
Self-Assessment: Soft Tissue Injury Clinical Scenarios
Apply the principles from this module to the following structured clinical scenarios. For each, work through a systematic assessment before reading the guidance. The scenarios are designed to test the three highest-yield examination areas: compartment syndrome recognition, open fracture management, and rhabdomyolysis identification.
Scenario 1 — Compartment Syndrome Recognition: A 16-year-old girl falls onto an outstretched hand and sustains a displaced supracondylar fracture of the humerus. After manipulation and backslab application, she rates her pain 8/10 and complains of tingling in her thumb and index finger. On examination: the forearm is tense and swollen, and passive finger extension markedly worsens the pain. The radial pulse is palpable but weak. What is the diagnosis? Which nerve's territory is the tingling in, and which compartment does that nerve traverse? What is the immediate management?
Scenario 2 — Open Fracture Management: A 45-year-old farmer is brought in with an open tibial fracture after his leg was trapped under a tractor. The wound is 12 cm long with visible bone, periosteal stripping, and heavy contamination with soil. X-ray shows a comminuted fracture. His pulse in the foot is palpable. What Gustilo-Anderson grade is this? List the management steps in order of priority for the first hour. What additional antibiotic is required for soil contamination?
Scenario 3 — Rhabdomyolysis: A 28-year-old is rescued from a car wreck after being trapped for 4 hours. His right leg is swollen and the muscles feel firm. Urine output has been minimal since arrival. The dipstick shows 3+ blood but no red cells on microscopy. CK returns at 18,000 U/L. Creatinine is 180 µmol/L. What is the diagnosis? What is the target urine output and what additive should be included in the IV fluid to protect the kidneys?
Review your answers against the preceding content sections. Identify any gaps in your understanding and return to the relevant heading before proceeding to the next SDL.
CLINICAL PEARL
The 'pain on passive stretch' sign is more reliable than pulse assessment in compartment syndrome. In a tibial compartment syndrome, passive dorsiflexion stretches the muscles of the anterior compartment over the inflamed, tense fascial envelope, reproducing ischaemic pain. This sign is positive BEFORE pulses are affected, BEFORE paraesthesia is established, and BEFORE paralysis occurs. A patient who screams when you passively dorsiflex their foot after a tibial fracture has compartment syndrome until proven otherwise — do not wait for pulse loss or a compartment pressure measurement if the clinical picture is obvious. Conversely, in an unconscious sedated patient, compartment pressure measurement (ΔP <30 mmHg = fasciotomy) is the objective gate when clinical signs cannot be elicited.