Page 3 of 13
OR12.1 | Congenital Malformation and Deformity Assessment — SDL Guide (Part 3)
DDH: Management
Management of DDH is entirely age-stratified: the earlier treatment begins, the more conservative and effective it is, and the more reliably normal acetabular development can be achieved without surgery.
Birth to 6 months — conservative management with the Pavlik harness is the standard of care. The harness is a dynamic splint that holds the hip in flexion (approximately 100°) and abduction, maintaining the femoral head concentrically within the acetabulum and stimulating acetabular remodelling. It is NOT a rigid immobiliser; the infant can kick freely, which promotes the mechanical stimulus for acetabular development. The harness is worn continuously (23 hours per day) and is typically required for 6–12 weeks for a stable, reducible hip. Treatment success rates with Pavlik harness for neonatal cases approach 90–95%. Failure of harness treatment (typically defined as persistent dislocation after 3–4 weeks of harness wear) warrants escalation to surgical or manipulation approaches; continued harness use in a persistently dislocated hip risks avascular necrosis of the femoral head (Pavlik harness disease) by maintaining inappropriate pressure on the posteriorly displaced head.
6 months to 18 months — if DDH is diagnosed in this age window (increasingly fixed dislocation), closed reduction under general anaesthesia is attempted, with the hip being brought to an acceptable position that is then maintained in a hip spica cast for 3–6 months. A pre-operative period of skin traction (2–3 weeks) is used in some centres to gradually bring the femoral head closer to the acetabulum, reducing the risk of avascular necrosis (AVN) of the femoral head from a forced reduction. Arthrography under anaesthesia confirms concentric reduction before the spica is applied.
After 18 months — established dislocation with soft-tissue contracture requires open reduction to clear intra-articular obstacles (inverted labrum, hypertrophied ligamentum teres, psoas impingement) combined with femoral shortening osteotomy (to prevent AVN by reducing the pressure of reduction) and, if acetabular dysplasia is severe, a Salter's innominate osteotomy or other pelvic osteotomy to redirect the acetabulum. Outcomes worsen progressively with increasing age at diagnosis, underlining the importance of neonatal screening.
Long-term complications of treated DDH include avascular necrosis of the femoral head (the most feared complication, affecting 5–15% even with optimal treatment), residual acetabular dysplasia with subsequent osteoarthritis in adult life, and leg-length discrepancy.
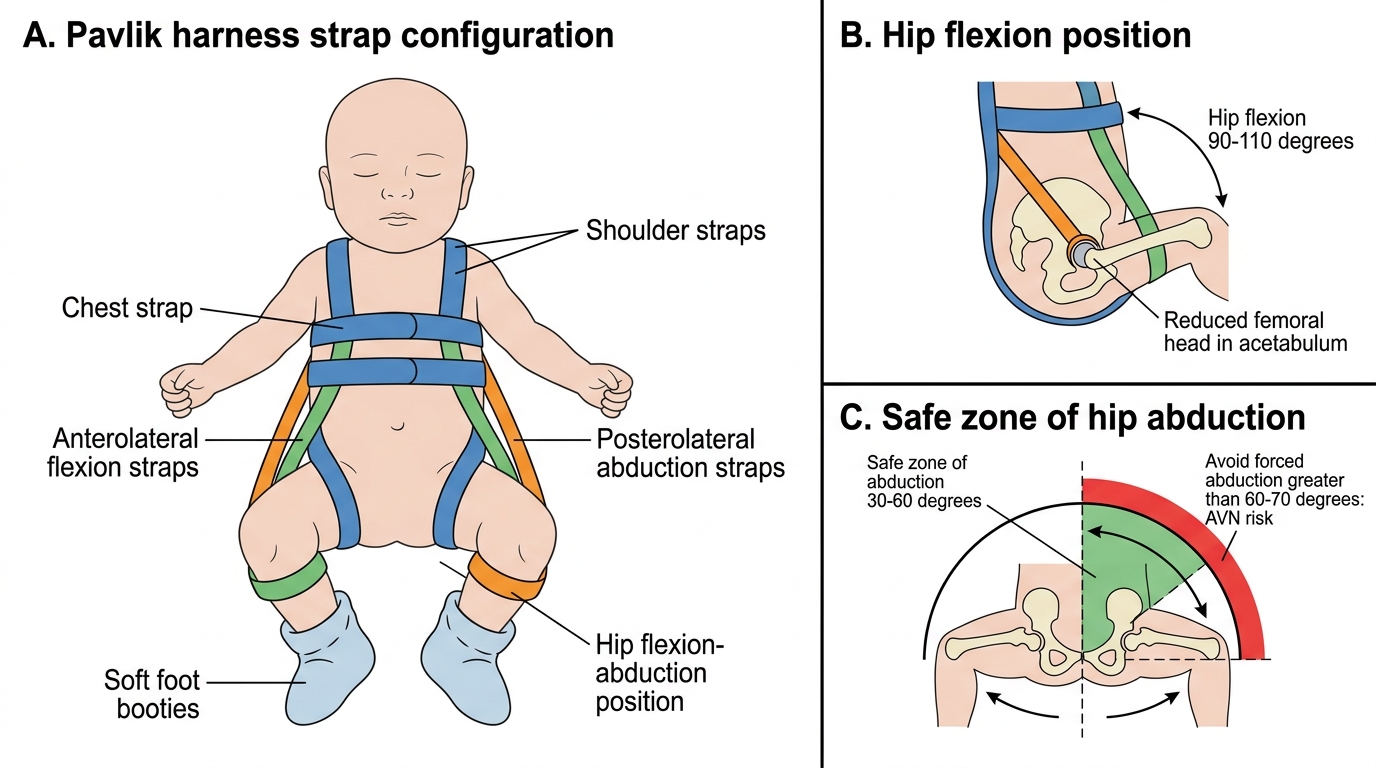
Pavlik Harness Positioning and Safe Hip Abduction
Congenital Muscular Torticollis: Pathology, Presentation, and Management
Congenital muscular torticollis (CMT, also called wry neck or sternomastoid tumour of infancy) is a postural deformity of the neck characterised by tilting of the head toward the affected side and rotation of the chin toward the contralateral side — reflecting unilateral contracture of the sternocleidomastoid (SCM) muscle. It is the third most common musculoskeletal birth defect after clubfoot and DDH, affecting approximately 0.4–2% of live births.
The pathological basis involves fibrosis within the SCM muscle, typically presenting as a palpable fibrotic mass (sternomastoid tumour) in the body of the muscle in the first few weeks of life. This mass is not a true neoplasm; it represents haemorrhage within the muscle during birth (stretch injury in difficult deliveries, particularly those involving forceps or vacuum) or intrauterine compartment syndrome from a restricted fetal position, followed by fibrous replacement of the damaged muscle fibres. The fibrotic SCM fails to elongate at the same rate as the growing contralateral SCM, producing progressive tilt and rotation deformity if untreated.
Clinically the infant is noted to hold the head tilted to the affected side with the chin rotated to the opposite side. On palpation a non-tender firm mass is felt in the body of the SCM in the first few weeks; this mass typically resolves by 4–8 months, leaving a fibrotic contracted muscle. Restricted passive rotation of the neck (inability to rotate the chin to the ipsilateral side) is the cardinal finding. Plagiocephaly (asymmetric flattening of the skull) develops if the deformity is untreated, as the infant preferentially rests on one side of the occiput.
Associated conditions must be actively sought: DDH is present in 2–8% of cases (reflecting shared intrauterine positional mechanisms), and cervical spine anomalies — particularly atlanto-axial instability and Klippel-Feil syndrome (congenital fusion of cervical vertebrae) — must be excluded before physiotherapy is prescribed.
Management follows a stepwise approach. Physiotherapy — passive stretching exercises performed by the parent under therapist supervision — is effective in over 90% of cases when commenced before 3 months of age and practised consistently. By the first year, spontaneous resolution occurs in the majority with physiotherapy alone. Surgical release (unipolar or bipolar sternocleidomastoid release) is reserved for the minority with persistent contracture beyond 12–18 months or significant plagiocephaly; outcomes are excellent if undertaken before 3 years of age, and acceptable up to 12 years.
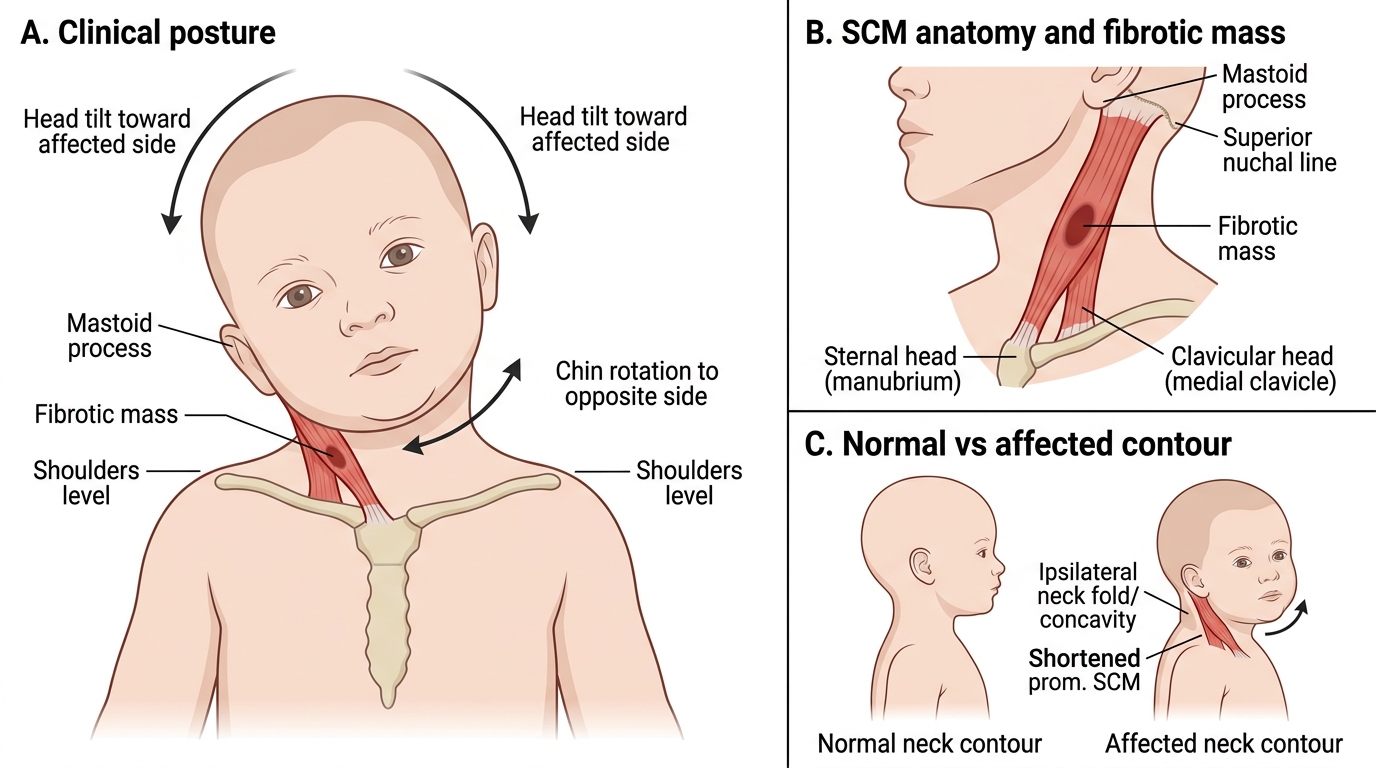
Congenital Muscular Torticollis: Posture, SCM Anatomy, and Neck Contour
Congenital Talipes Equinovarus (CTEV): Anatomy and Components
Congenital talipes equinovarus (CTEV), commonly known as clubfoot, is one of the most prevalent congenital musculoskeletal anomalies worldwide, affecting approximately 1–2 per 1,000 live births with a 2:1 male predominance and bilateral involvement in approximately 50% of cases. Despite its striking appearance at birth — the foot turned inward, downward, and supinated — the deformity is fully correctable with early conservative treatment in the vast majority of idiopathic cases. The term 'talipes equinovarus' is descriptive: 'talipes' refers to the foot (talus + pes), 'equinus' describes the plantarflexed position (resembling a horse's hoof), and 'varus' indicates the inversion of the hindfoot. Four anatomical components define the deformity, memorably encoded in the mnemonic CAVE, and understanding each component individually is essential to understanding both the mechanism of the deformity and the logic of the Ponseti correction sequence.
The aetiology of CTEV is multifactorial. Genetic factors play a significant role: the recurrence risk to a sibling is approximately 2–5%, and concordance in monozygotic twins is approximately 33%, suggesting combined genetic and environmental contributions rather than a purely single-gene or purely environmental cause. Intrauterine positional factors, neuromuscular abnormalities (CTEV associated with spina bifida, arthrogryposis, or cerebral palsy tends to be stiffer and less responsive to conservative treatment), and developmental arrest during the 8th–12th week of embryonic foot development have all been proposed as contributing mechanisms. The distinction between idiopathic CTEV and syndromic/neuromuscular CTEV is clinically important because it directly affects the prognosis and the likely number of treatment interventions required.
The four components of clubfoot, systematically described:
- Cavus — an abnormally high medial longitudinal arch, resulting from plantarflexion of the forefoot relative to the hindfoot; the navicular is displaced medially, and the plantar fascia is contracted.
- Adductus (forefoot adduction) — medial deviation of the forefoot and midfoot; the navicular dislocates medially relative to the talar head.
- Varus — hindfoot inversion; the calcaneus is rotated inward (supinated) under the talus.
- Equinus — plantarflexion of the entire foot; the calcaneus is held in equinus by a tight tendo Achillis and posterior ankle and subtalar joint capsule. The talus itself is plantarflexed and internally rotated within the ankle mortise.
These four components are not independent deformities but aspects of a single, integrated positional malalignment of the foot skeleton. The talus occupies an abnormal position of plantarflexion and internal rotation within the ankle mortise, and every other bone in the foot is displaced relative to this talar mal-position. The medial structures (tibialis posterior tendon, medial ligaments, plantar fascia, and plantar intrinsic muscles) are short and contracted; the lateral structures are stretched. Understanding this integrated talar mechanism is the conceptual basis of the Ponseti method of sequential correction.
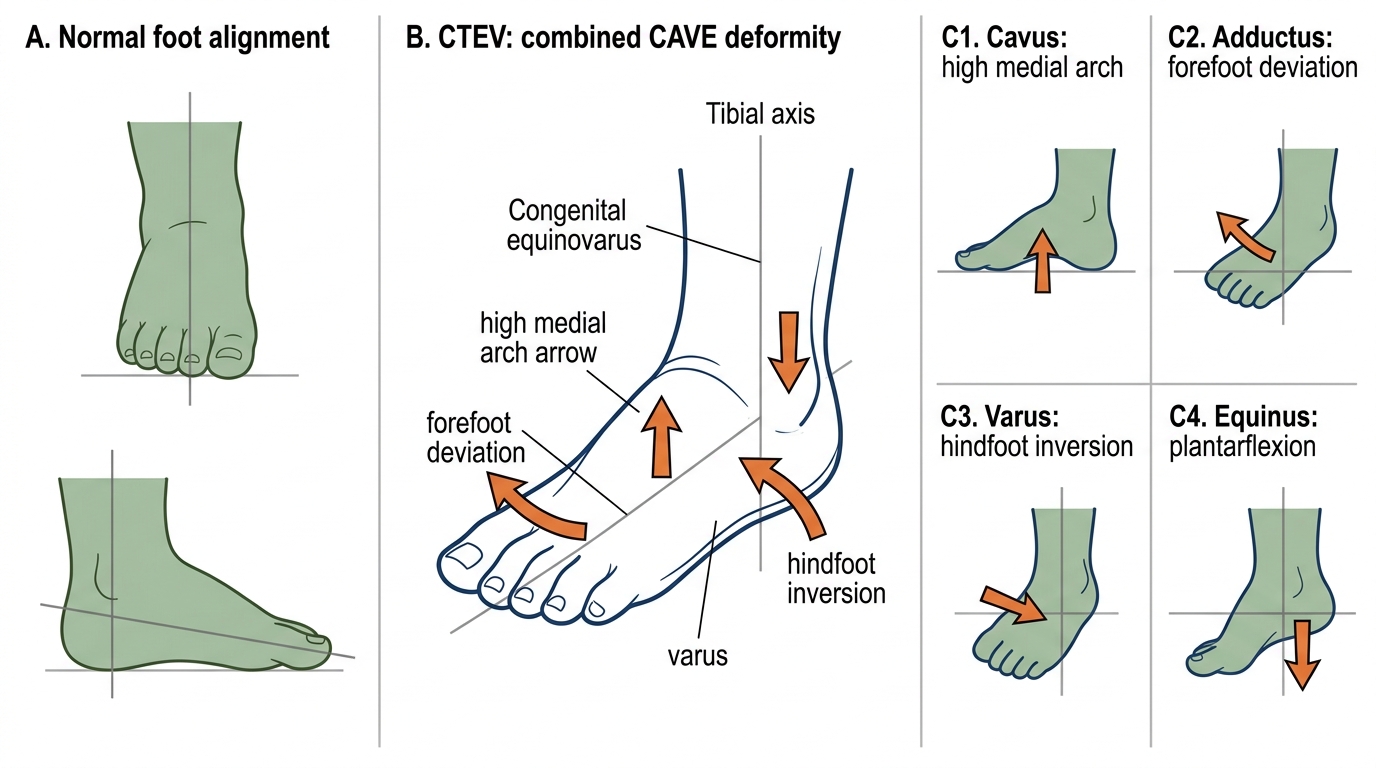
CTEV Foot: CAVE Components