Page 4 of 13
OR12.1 | Congenital Malformation and Deformity Assessment — SDL Guide (Part 4)
CTEV: Assessment and the Ponseti Method
Provided image
Clinical assessment of clubfoot begins at birth and serves two purposes: to confirm the diagnosis, distinguish true CTEV from positional talipes (a flexible postural deformity that corrects fully with gentle manipulation), and to grade severity. The Pirani scoring system is the most widely used clinical severity grading tool, assigning 0, 0.5, or 1 point to six clinical parameters (three hindfoot: equinus, empty heel, and posterior crease; three midfoot: curvature of lateral border, medial crease, and coverage of talar head) for a maximum score of 6. A higher Pirani score indicates a more rigid and severe deformity, requiring more casting cycles. Baseline Pirani scoring guides treatment duration and identifies hips that may need more intensive correction.
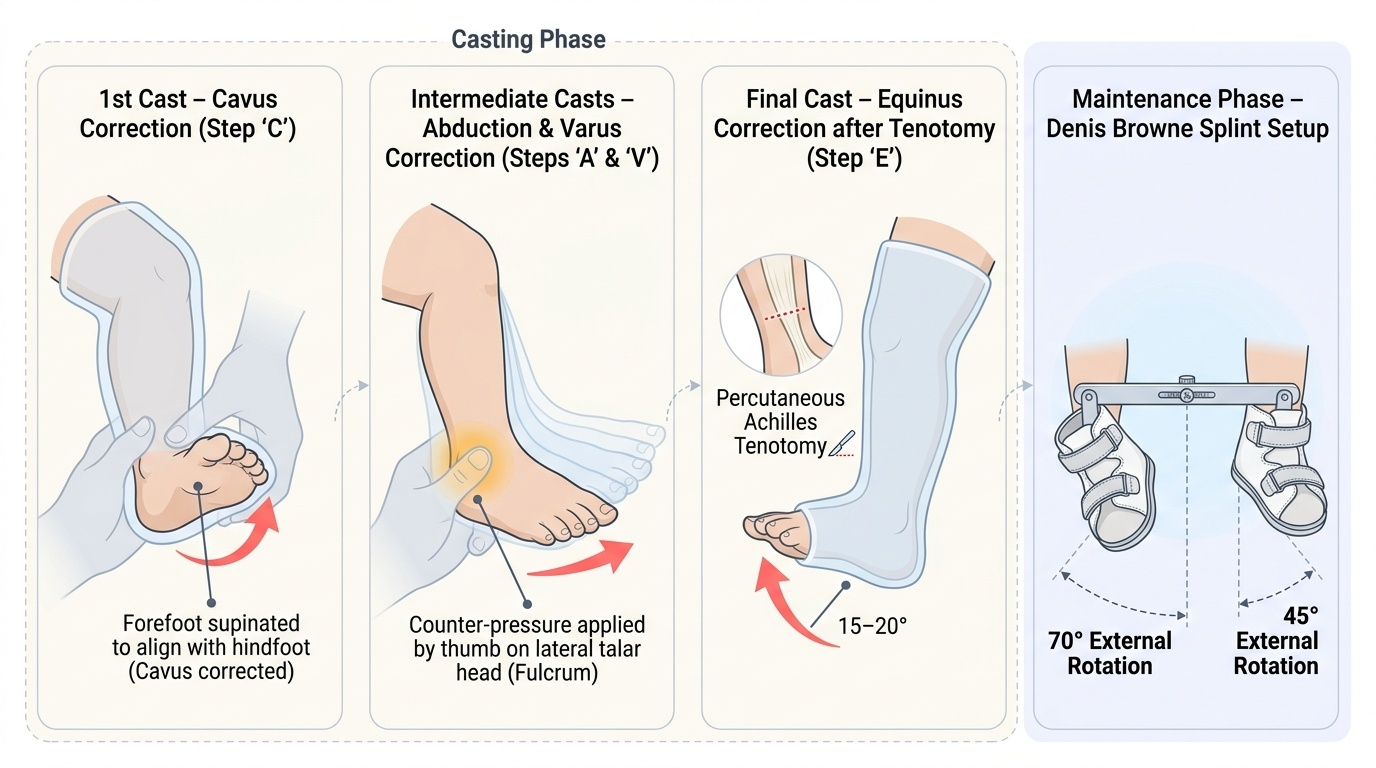
The Ponseti method is the internationally accepted gold standard for first-line treatment of idiopathic CTEV. It is based on an understanding of foot kinematics that recognises the talus as the keystone: correction must begin by correcting the supination and adduction before attempting to correct equinus. The sequence is systematic:
- Casting phase: Weekly or fortnightly manipulation followed by application of an above-knee plaster cast, sequentially correcting the deformity in the order C → A → V → E (Cavus corrected first by supinating the forefoot to bring it in line with the hindfoot; then Adductus and Varus corrected together by abducting the forefoot while maintaining supination with thumb pressure on the talar head). Equinus is corrected last, after achieving at least 70° of abduction. The average idiopathic clubfoot requires 5 to 7 casts over a period of 5–7 weeks.
- Percutaneous Achilles tenotomy: After maximal correction of C, A, and V, residual equinus is addressed by a percutaneous section of the tendo Achillis under local anaesthesia (in clinic or with sedation), followed by a final cast for 3 weeks to allow tendon healing.
- Foot abduction bracing (Dennis-Brown splint or Dobbs brace): This is the most critical phase for preventing relapse. A foot abduction orthosis (shoes mounted on a bar, held at 70° of external rotation on the affected side and 45° on the normal side) must be worn full-time for 3 months and then at night and naps until the age of 4 to 5 years. Brace non-compliance is the primary cause of relapse, which affects 30–40% of cases and requires repeat casting or tibialis anterior tendon transfer.
Surgical treatment (posteromedial soft tissue release) has largely been replaced by the Ponseti method in expert centres, as it was associated with a high rate of stiff, arthritis-prone feet in adult life. Surgery remains an option for failed Ponseti, late presentations, and associated neuromuscular conditions where the deformity is rigid.
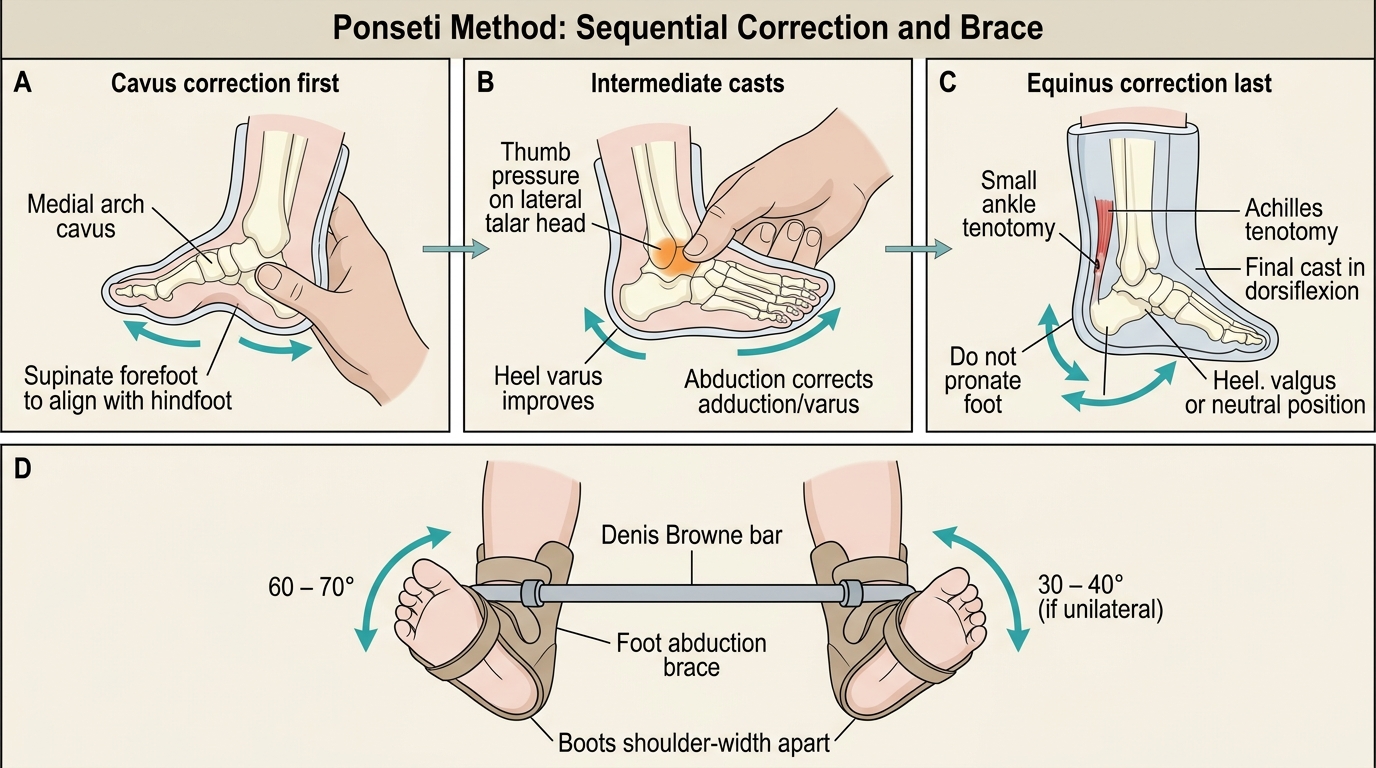
Ponseti Method: Sequential Correction and Brace
SELF-CHECK
A 6-week-old infant is referred with confirmed bilateral CTEV. The treating surgeon plans to use the Ponseti method. Regarding the correct sequence of correction, which sequence is accurate?
A. Equinus → Varus → Adductus → Cavus
B. Cavus → Adductus + Varus → Equinus (with Achilles tenotomy if needed)
C. Adductus → Equinus → Varus → Cavus
D. Varus → Cavus → Equinus → Adductus
Reveal Answer
Answer: B. Cavus → Adductus + Varus → Equinus (with Achilles tenotomy if needed)
The Ponseti method corrects the CAVE deformity in sequence: Cavus first (by supinating the forefoot to align it with the hindfoot), then Adductus and Varus together (by abducting the forefoot with the thumb pressing on the lateral talar head), and finally Equinus last. Premature attempts to correct equinus before abduction is achieved will produce a rocker-bottom deformity (calcaneocavus) rather than true equinus correction. Achilles tenotomy addresses residual equinus after maximal abduction is achieved — typically required in 80% of idiopathic cases.
Integrated Imaging and Investigation Strategy
For the final-year student, a systematic approach to investigation across all four congenital conditions consolidates the principles taught in each section. The key variables are the age of the child, the degree of skeletal ossification, and whether soft-tissue or bony detail is the primary diagnostic question.
For scoliosis, the standing PA and lateral full-spine radiograph (on a 36-inch cassette that includes the full spinal column and the pelvis) is the primary investigation, enabling Cobb angle measurement, Risser staging, and identification of congenital vertebral anomalies. MRI of the whole spine is mandatory in: congenital scoliosis (intraspinal anomalies), any scoliosis with pain or rapid progression, infantile/juvenile idiopathic scoliosis, and neurological signs. Bending films (right and left lateral bending) are used pre-operatively to assess curve flexibility.
For spina bifida, the maternal triple screen (AFP + βhCG + unconjugated estriol at 15–20 weeks) and the 18–20 week anomaly ultrasound are the first-line prenatal investigations. Postnatal MRI of the spine is mandatory for all cases of spinal dysraphism, both open and occult, to delineate the lesion, exclude tethered cord, and plan neurosurgical management.
For DDH, the age-based imaging algorithm is strict: ultrasound (Graf classification) under 4–6 months, AP pelvis radiograph over 4–6 months. In cases where reduction is being performed under anaesthesia, fluoroscopy and arthrography provide real-time guidance. MRI is used for pre-operative soft-tissue mapping.
For CTEV, plain radiography (AP and lateral weight-bearing-simulated views of the foot — the Kite angles: the talocalcaneal angle and the talus-first metatarsal angle) confirms the diagnosis and monitors correction. In normal feet, the talocalcaneal angle on AP is approximately 20–40° (the calcaneus diverges from the talus); in clubfoot it is reduced toward 0°, reflecting the parallel position of the talus and calcaneus. MRI is reserved for complex or syndromic cases requiring surgical planning.
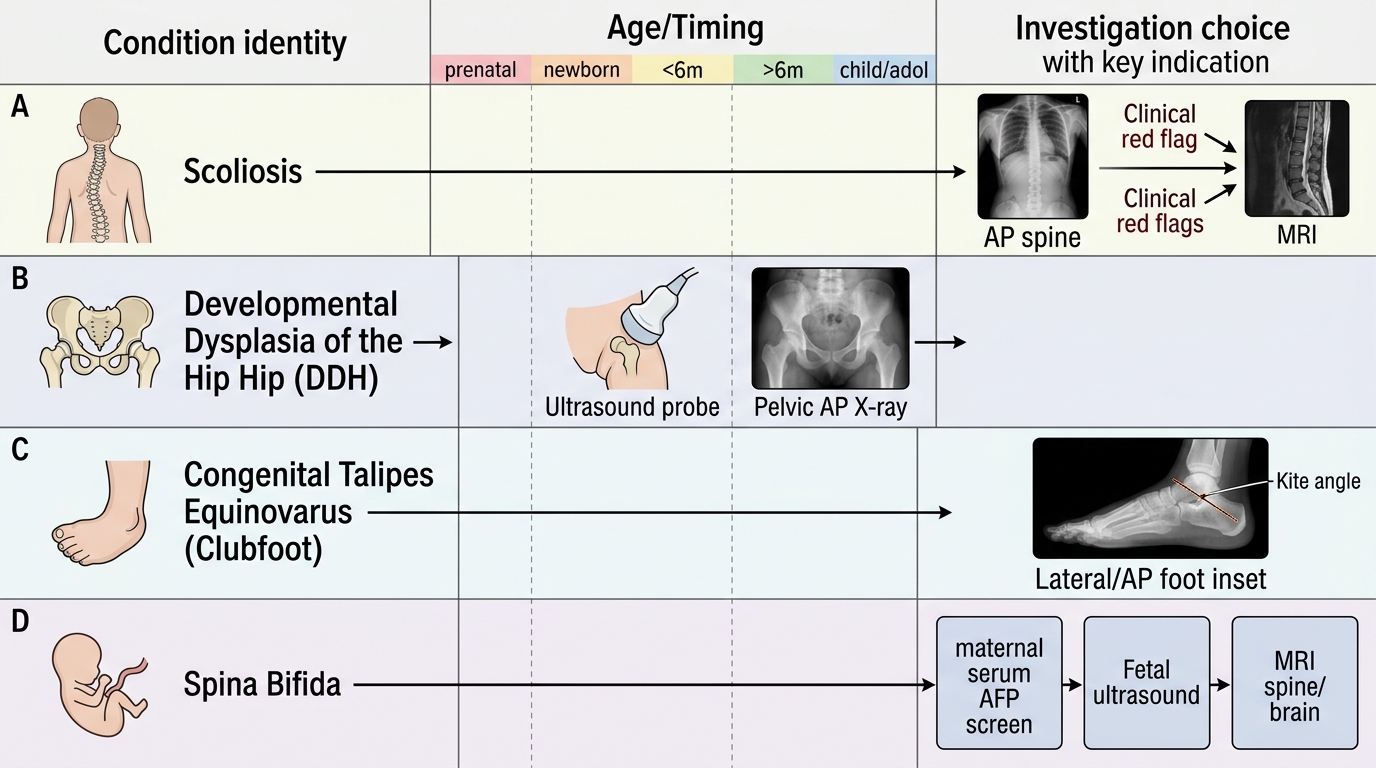
Investigation Choice in Congenital Orthopaedic Lesions
Management Principles Across Congenital Conditions
A unifying principle across all congenital musculoskeletal conditions is that the earlier treatment begins, the more biologically plastic the tissue response — and therefore the more effective and less invasive the treatment needed. Neonatal cartilage and fibrocartilage remodel in response to corrective mechanical forces; the same tissue in a 3-year-old is increasingly resistant. This underlies every age-stratified treatment algorithm described above.
For scoliosis, management is primarily surveillance and bracing in the growing child, with surgery reserved for large or rapidly progressive curves. Physiotherapy approaches (Schroth method) may supplement bracing in motivated adolescents but are not a substitute for it in curves >25°. Importantly, exercise alone does not halt curve progression.
For spina bifida, the management paradigm is multidisciplinary from birth: neurosurgery (meningocele/myelomeningocele closure, VP shunting), urology (neurogenic bladder — clean intermittent catheterisation, monitoring for upper tract damage), orthopaedics (deformity management, assistive devices), physiotherapy, and rehabilitation. The orthopaedic contribution includes management of hip dislocation (commonly associated with lumbar-level lesions), foot deformity, and scoliosis.
For DDH, the escalating treatment algorithm — Pavlik harness → closed reduction + spica cast → open reduction ± osteotomy — reflects the progressive stiffness and soft-tissue contracture that develops with age. The goal at every stage is concentric reduction of the femoral head within the acetabulum, which then drives normal acetabular remodelling.
For torticollis, early physiotherapy resolves >90% of cases; surgery is a well-defined salvage procedure for persistent cases and should not be delayed beyond 3 years of age.
For CTEV, Ponseti casting is successful in >90% of idiopathic cases, but the brace wear protocol must be rigorously maintained for the first 4–5 years of life. Parents must understand that relapse is common with poor compliance, and that relapse does not represent treatment failure — re-casting is highly effective for relapses.
Country-specific considerations for India include a significant number of late-presenting cases due to limited neonatal screening infrastructure in rural and semi-urban areas. DDH presenting at walking age, clubfeet presenting after 2 years of age, and scoliosis presenting at severe curve magnitudes are not uncommon in district hospital practice, and the student must be familiar with the surgical management algorithms for these late presentations.
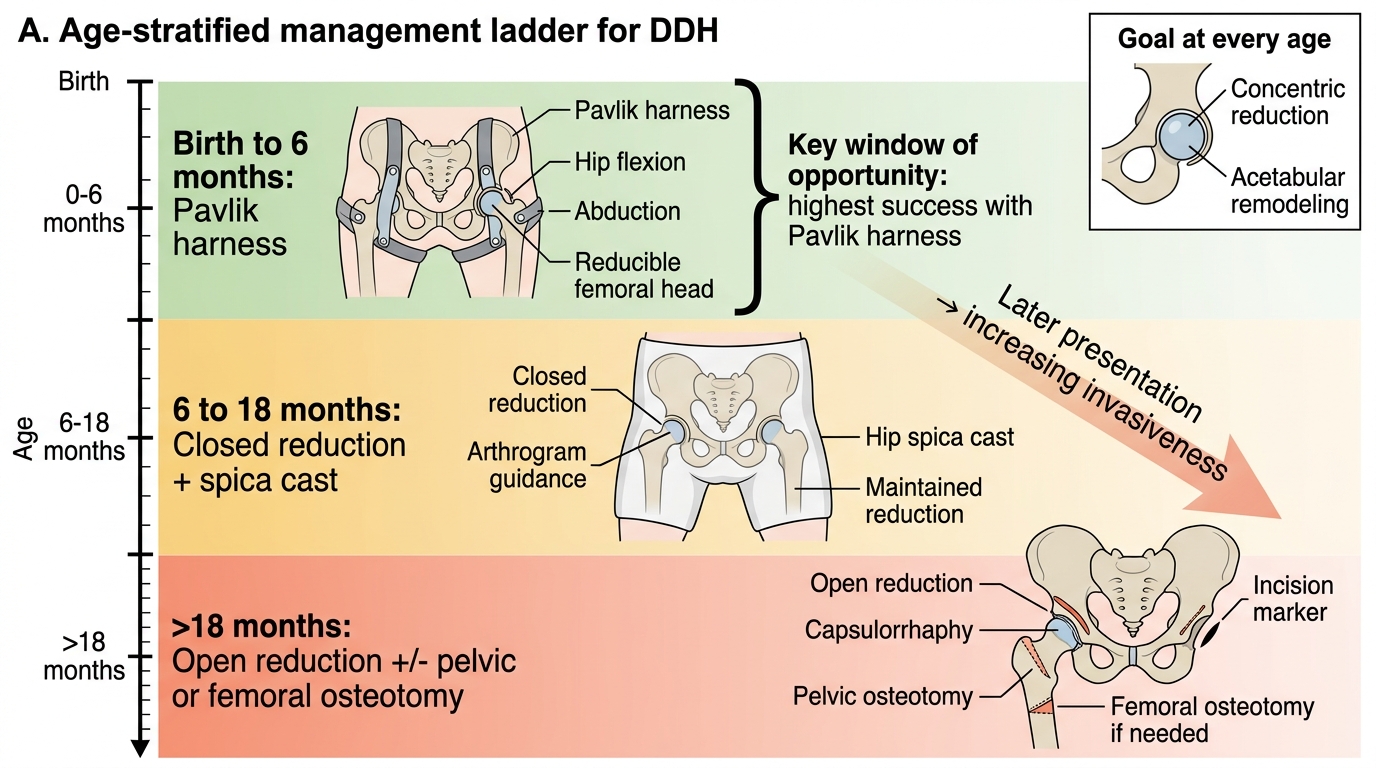
Age-Stratified Management Ladder for DDH
SELF-CHECK
A 4-month-old infant is diagnosed with left DDH. Ortolani and Barlow tests are positive. Which is the most appropriate initial treatment?
A. Observation — most cases of DDH resolve spontaneously by 4 months
B. Pavlik harness, worn 23 hours per day with fortnightly ultrasound review
C. Closed reduction under general anaesthesia and hip spica casting
D. Open reduction with femoral shortening osteotomy
Reveal Answer
Answer: B. Pavlik harness, worn 23 hours per day with fortnightly ultrasound review
At 4 months, the Pavlik harness is the standard of care for DDH with positive provocation tests. The harness maintains the hip in a position of flexion and abduction, stimulating acetabular development through concentric loading. Closed reduction under anaesthesia is appropriate if Pavlik harness fails (persistent dislocation after 3–4 weeks) or if presentation is between 6–18 months. Open reduction is reserved for children over 18 months or those in whom closed reduction fails. The window for Pavlik harness treatment generally extends to 6 months.