Page 5 of 14
OR13.2 | Polytrauma Resuscitation Team Skills — SDL Guide
Learning Objectives
- Describe the ATLS ABCDE framework and explain the rationale for its fixed sequential order in polytrauma resuscitation
- Identify the indications and contraindications for bladder catheterisation in a trauma patient, including the significance of blood at the urethral meatus
- Describe the technique and anatomical landmarks for peripheral intravenous access and recognise when central venous access is required
- State the indications for endotracheal intubation in a trauma victim and describe the pre-oxygenation and laryngoscopy sequence
- Explain the role of a junior team member during polytrauma resuscitation and demonstrate appropriate splintage as part of the team response
INSTRUCTIONS
Polytrauma — injury involving two or more body regions with at least one life-threatening injury — is the leading cause of death in Indians aged 15–45. The first hour of resuscitation ('the golden hour') determines survival. The Advanced Trauma Life Support (ATLS) framework provides a standardised, evidence-based approach that every doctor in India is expected to know and apply. As a Phase III MBBS graduate, you will not lead a trauma team from day one, but you will be called upon to perform specific procedural tasks as a team member: establishing intravenous access, catheterising the bladder, assisting with intubation, and applying splints. This SDL prepares you for that precise, high-stakes role.
References
- ATLS Advanced Trauma Life Support — Student Course Manual, 10th ed (textbook)
- Maheshwari's Essential Orthopaedics, 5th ed, Ch 8 (Polytrauma Management) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 22 (Emergency Management of Skeletal Trauma) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old motorcyclist is brought to your casualty following a high-speed road traffic accident. He is unconscious, his airway is gurgling with blood, his blood pressure is 80/50 mmHg, his pelvis is grossly unstable on compression, and his right thigh is deformed and swollen. Four doctors are in the room. One is shouting 'get me an X-ray!', another is trying to insert an IV line in the antecubital fossa without gloves, a third is attempting to catheterise without checking the perineum, and a fourth is on the phone requesting an orthopaedic surgeon. No one has secured the airway. The patient dies of hypoxic cardiac arrest 12 minutes after arrival. He was salvageable.
This scenario is not invented — it is a composite of real preventable deaths in Indian casualty departments. The ATLS ABCDE framework exists precisely to prevent this sequence of simultaneous uncoordinated actions from replacing the correct sequential, priority-driven approach. Today you will learn your role as a team member in that framework.
WHY THIS MATTERS
Road traffic accidents in India kill over 150,000 people annually; blunt trauma and penetrating injuries together make polytrauma the single most important acute clinical scenario you will encounter as an intern and junior resident. Unlike most clinical conditions, polytrauma demands simultaneous assessment and treatment, team coordination, and prioritised procedures — skills that cannot be improvised in the moment. The specific procedural competencies in OR13.2 (IV access, bladder catheterisation, endotracheal intubation, splintage) are performed hundreds of times in every district hospital every year. Knowing when and how to perform them, and knowing when NOT to (e.g. catheter contraindicated if urethral injury), directly determines patient outcome.
RECALL
Before proceeding, activate your prior knowledge:
- What does ATLS stand for, and what does the acronym ABCDE represent in the trauma survey?
- What anatomical structure separates the retroperitoneal space from the pelvis, and why does a pelvic fracture cause massive haemorrhage?
- What is the anatomical landmark for locating the internal jugular vein for central venous access?
- What is the difference between the trachea and the oesophagus in terms of their relationship to the larynx — and why does this matter for intubation?
- Name the three tests of urethral integrity before bladder catheterisation.
If you are uncertain about any of these, revisit your basic surgical anatomy before continuing.
Clinical Indication and the ATLS ABCDE Framework
Polytrauma resuscitation is the systematic, team-based management of a patient with multiple injuries, in which life-threatening conditions are identified and treated simultaneously in order of priority. The clinical indication for activating a full trauma resuscitation team is a high-energy mechanism (high-speed road crash, fall from >3 metres, penetrating torso injury) combined with any haemodynamic instability or altered consciousness. The ATLS framework, developed by the American College of Surgeons and now adopted globally including in India's emergency training, provides the sequential ABCDE approach that ensures the most immediately life-threatening problem is addressed before moving to the next — because an unsecured airway kills in minutes, while a missed forearm fracture does not. Understanding why the steps are ordered as they are — rather than merely memorising their labels — is the intellectual foundation of competent trauma care. Each letter in the acronym corresponds to a physiological threat ranked by the speed at which it kills: airway obstruction causes death within 3–5 minutes from hypoxic arrest; uncontrolled haemorrhage kills in 10–30 minutes; undetected tension pneumothorax kills within minutes of development; a raised intracranial pressure kills over hours. ABCDE therefore encodes a survival-probability hierarchy that must never be reordered by clinical urgency-blindness or the pressure of a crowded trauma bay.
The ATLS primary survey follows the fixed sequence:
- A — Airway with cervical spine control: open and maintain the airway while protecting the cervical spine with manual in-line stabilisation. Look for blood, vomit, foreign body, or soft-tissue swelling obstructing the upper airway.
- B — Breathing and ventilation: assess for tension pneumothorax (absent breath sounds + tracheal deviation + haemodynamic collapse), open chest wound, massive haemothorax, flail chest. Administer high-flow oxygen.
- C — Circulation with haemorrhage control: assess pulse rate, blood pressure, capillary refill. Identify external haemorrhage and apply direct pressure. Establish IV access and begin fluid resuscitation. Identify the source of internal haemorrhage (chest, abdomen, pelvis, long bones).
- D — Disability (neurological status): assess level of consciousness using the AVPU scale (Alert/Verbal/Pain/Unresponsive) or Glasgow Coma Scale. Assess pupils.
- E — Exposure with environment control: fully expose the patient for complete assessment; then cover to prevent hypothermia.
The secondary survey (head-to-toe examination, AMPLE history) follows ONLY after the primary survey is complete and the patient is haemodynamically stable.
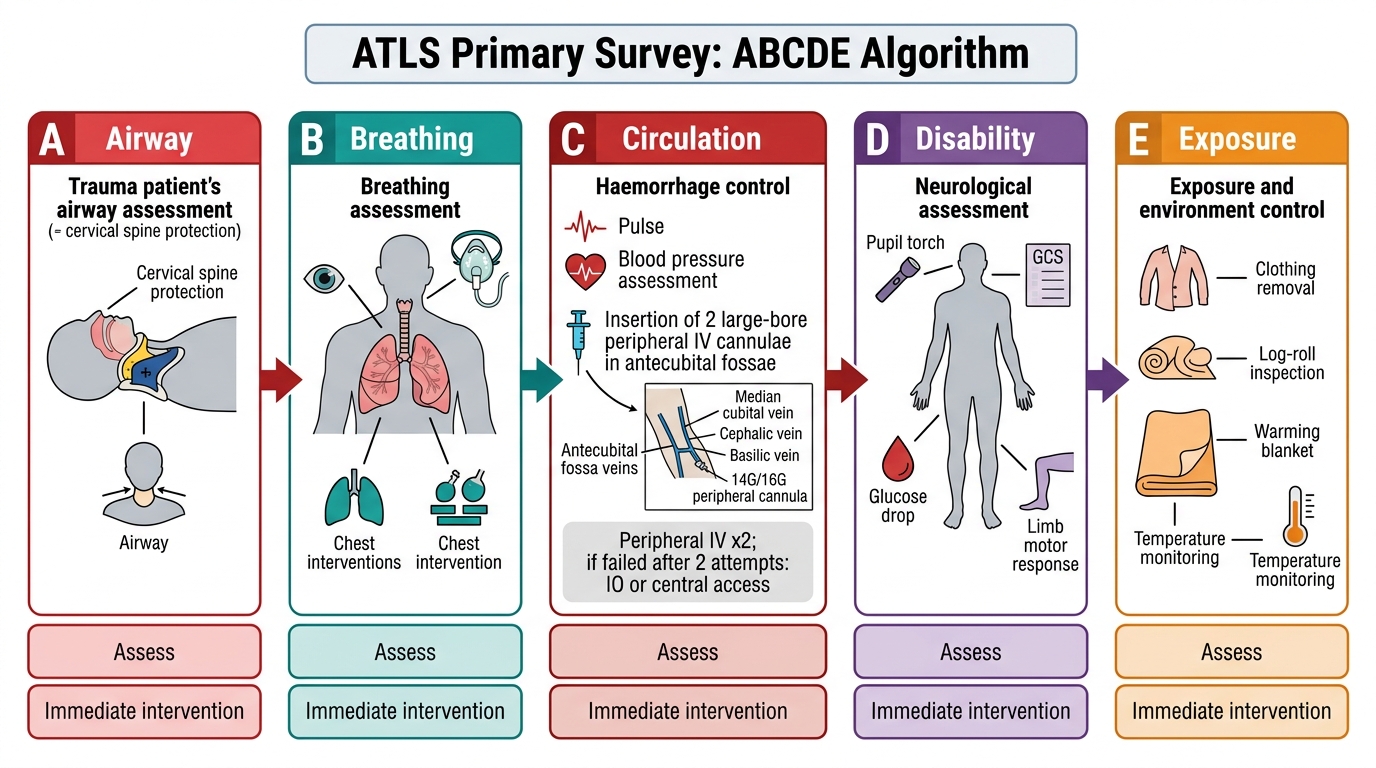
ATLS ABCDE Primary Survey Algorithm
Anatomy and Governing Principles: IV Access
Provided image
Establishing intravenous access is the first procedural step in the C (Circulation) limb of the ATLS primary survey, performed immediately after identifying haemodynamic compromise. The governing principle is to establish the largest-bore access in the shortest time, starting with peripheral venous access, and escalating to central or intra-osseous access if peripheral cannulation fails after two attempts.
Peripheral IV access: the standard trauma cannula is a 14G or 16G short cannula placed in a large peripheral vein — preferably the antecubital fossa veins (median cubital, cephalic, or basilic) or the forearm. Short, large-bore cannulae deliver a higher flow rate than long, narrow lines: flow rate is proportional to the fourth power of the radius and inversely proportional to length (Hagen-Poiseuille). A 14G peripheral cannula delivers fluid faster than a 16G central venous catheter. In trauma, the target is two large-bore peripheral cannulae before central access is considered.
Anatomy of the antecubital fossa: the median cubital vein crosses the superficial fascia of the antecubital fossa diagonally from the cephalic (lateral) to the basilic (medial) system. It is the most commonly cannulated vein for phlebotomy and IV access because it is large, relatively fixed, and superficial. Deep to the bicipital aponeurosis lie the brachial artery (medial) and the median nerve — a cannula placed too deep or too medially risks inadvertent arterial puncture.
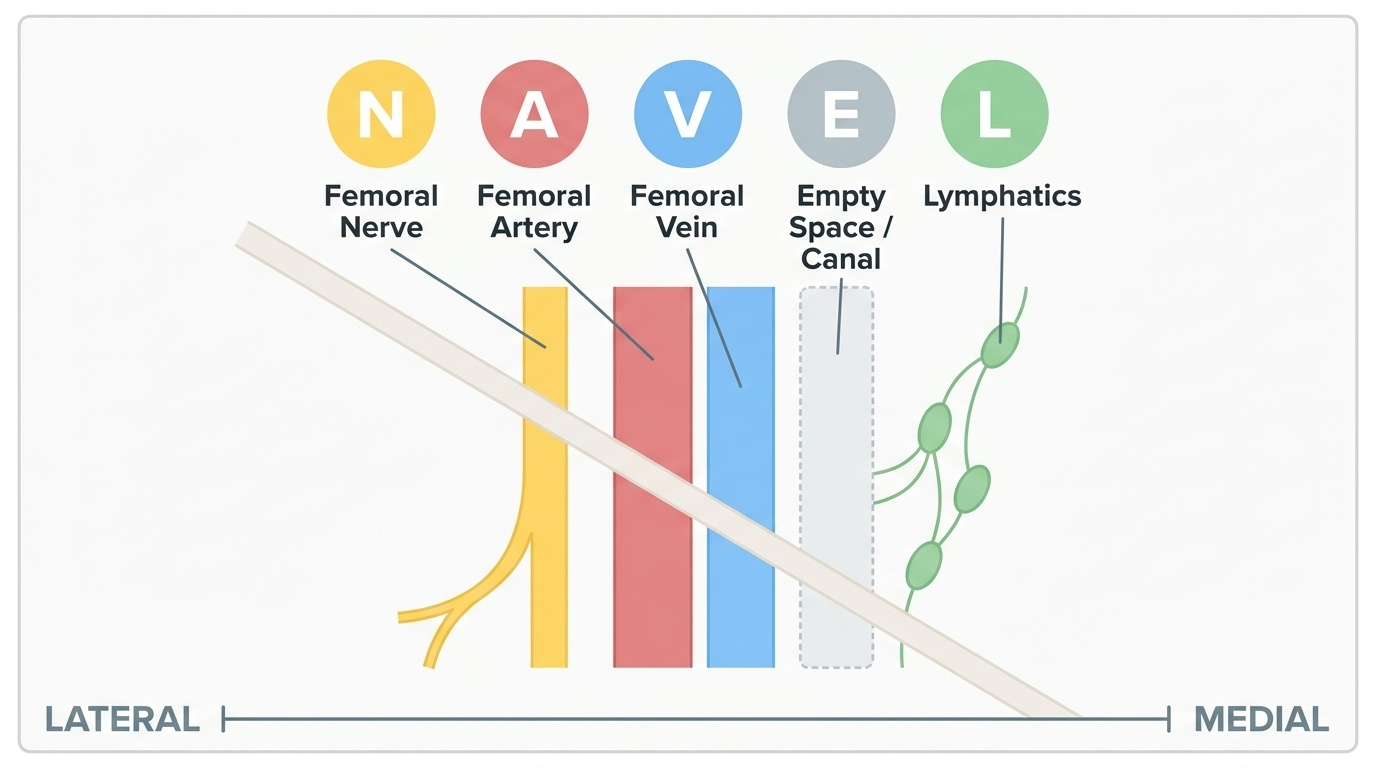
Central venous access is indicated when: (a) peripheral access is impossible (collapsed veins, severe hypovolaemia), (b) central venous pressure monitoring is required, or (c) vasoactive drugs must be infused. In trauma, the femoral vein is the preferred central access site because it is remote from the airway (which may be simultaneously being secured) and carries a lower risk of pneumothorax than subclavian or internal jugular approaches. The anatomical landmark for femoral vein access is 1–2 cm medial to the femoral artery pulse, below the inguinal ligament (NAVEL: Nerve-Artery-Vein-Empty space-Lymphatics, medial to lateral). The Seldinger technique (needle → guidewire → dilator → catheter) is used for central access.
Intra-osseous (IO) access: if vascular access fails in an emergency, IO access via the proximal tibia (2 cm below the tibial tuberosity, anteromedial surface) or distal femur can deliver fluids and drugs rapidly. IO needles provide access to the non-collapsible medullary venous sinusoids.
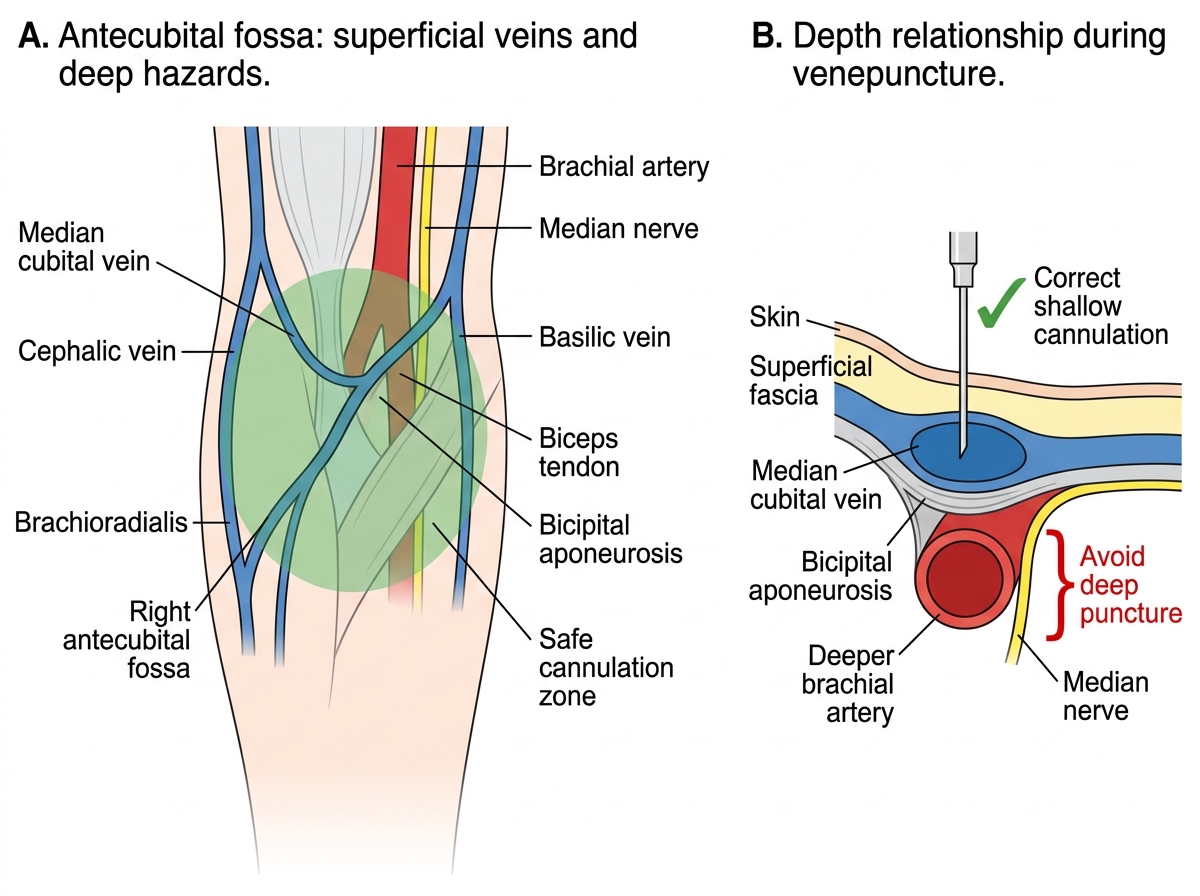
Safe Cannulation Anatomy of the Antecubital Fossa
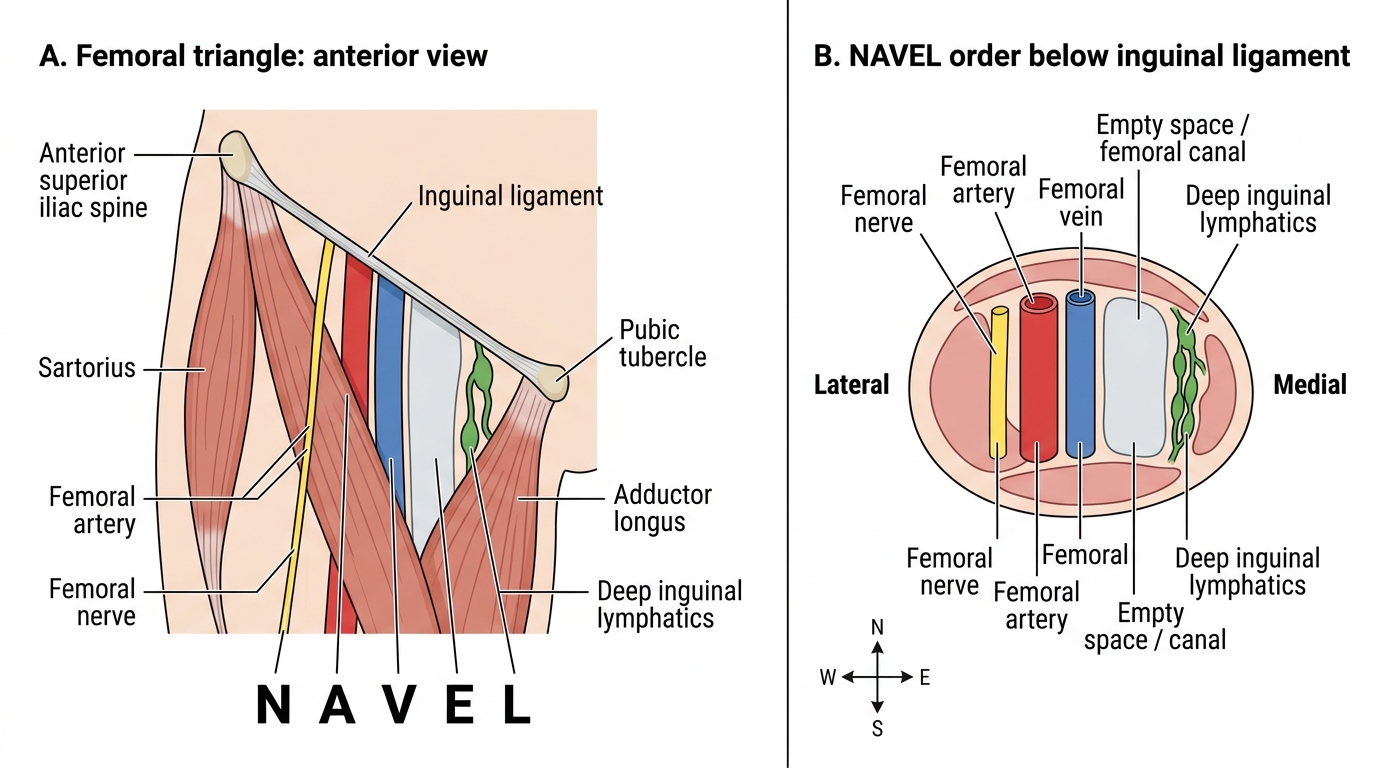
NAVEL Mnemonic in the Femoral Triangle
Anatomy and Governing Principles: Bladder Catheterisation
Bladder catheterisation in trauma serves two purposes: it relieves acute urinary retention and — more importantly for monitoring — enables accurate hourly urine output measurement as a real-time proxy for renal perfusion and resuscitation adequacy. The target urine output in resuscitation is ≥0.5 mL/kg/hour in adults and ≥1 mL/kg/hour in children. Unlike blood pressure, which can be artificially preserved by compensatory vasoconstriction for a surprising period in a young fit patient, urine output reflects splanchnic and renal perfusion directly and falls early in the compensated phase of shock. A trauma patient producing 40 mL of urine per hour is adequately perfused at the renal level; one producing 15 mL/h despite a seemingly normal blood pressure is not — the catheter turns that invisible physiological signal into a visible, actionable number. Recognising this makes bladder catheterisation not merely a nursing task but a genuine diagnostic and monitoring intervention that the informed physician orders and interprets.
The most important governing principle is the contraindication to catheterisation when urethral injury is suspected. Attempting to catheterise a ruptured urethra converts a partial tear into a complete disruption and introduces infection into the periurethral haematoma. The clinical signs of urethral injury that MUST be checked before catheterisation are:
1. Blood at the urethral meatus — the single most reliable clinical sign; if present, catheterisation is absolutely contraindicated until a urethrogram confirms urethral integrity.
2. Perineal or scrotal bruising/haematoma — bruising in the butterfly distribution in the perineum indicates a bulbar urethral injury (straddle injury mechanism).
3. High-riding or impalpable prostate on digital rectal examination (DRE) — in men with pelvic fractures, a disrupted urethra allows the prostate to displace superiorly; absence of the normal anterior rectal wall bulge on DRE suggests this. Note: DRE is NOT mandatory in all trauma patients but is performed when urethral injury is suspected.
If any of these three signs is present, do NOT catheterise transurethrally. A suprapubic catheter (inserted percutaneously above the pubic symphysis into the distended bladder) is the safe alternative and should be placed by the supervising surgeon.
Anatomy for male catheterisation: the male urethra is 18–20 cm long with two acute angulations — at the external sphincter (membranous urethra) and at the prostatic apex. The catheter must be advanced its full length (until urine flows) before inflating the balloon; inflating the balloon in the urethra causes traumatic rupture.
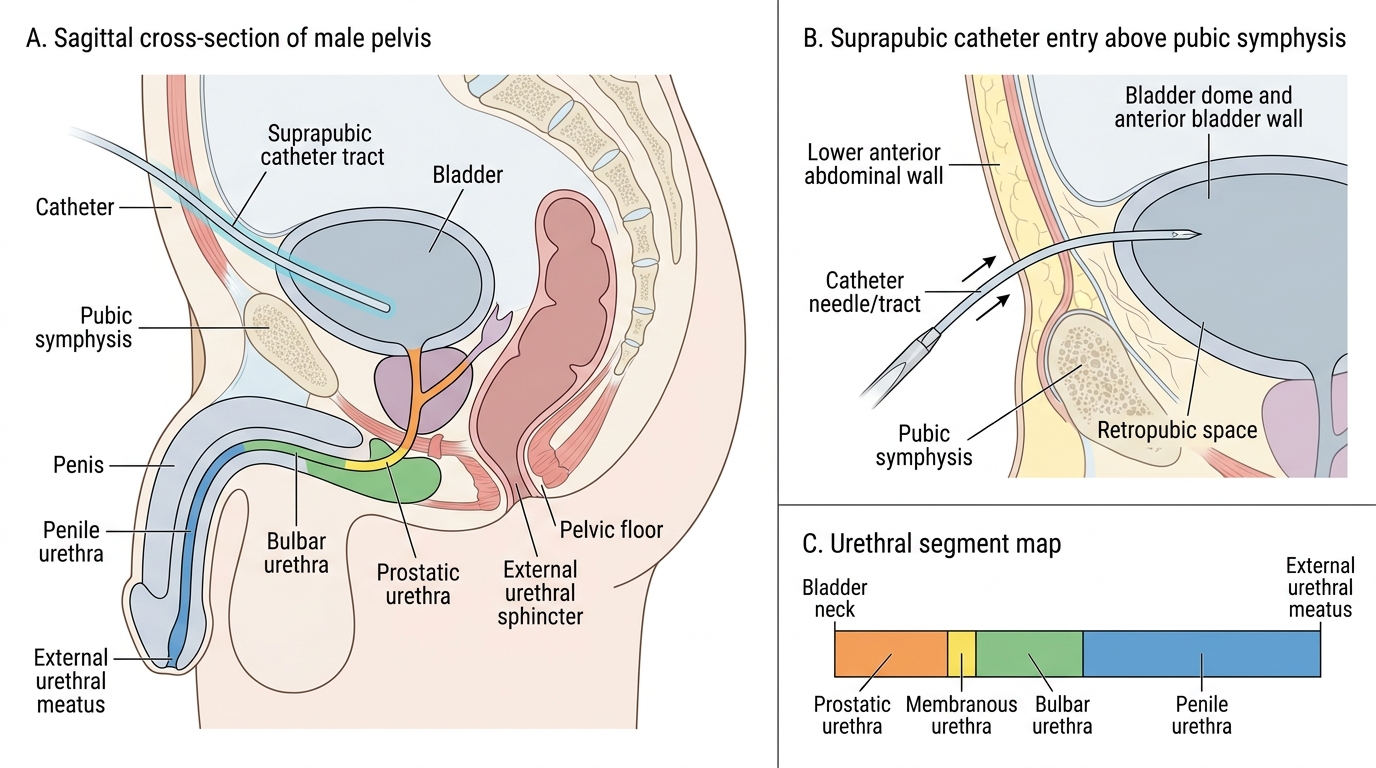
Male Pelvis Urethral Course and Suprapubic Catheter Site