Page 7 of 16
OR14.4 | Lower Limb Amputation Rehabilitation Counselling — SDL Guide
Learning Objectives
- Describe the standard levels of lower limb amputation — Syme's, below-knee (transtibial), through-knee, and above-knee (transfemoral) — and the clinical indications that determine the level chosen
- Enumerate the characteristics of an ideal amputation stump and explain why each characteristic matters for prosthetic fitting and rehabilitation
- Explain the types of prosthesis used in below-knee amputation, with particular focus on the patellar tendon bearing (PTB) socket, and counsel a patient on realistic functional expectations with prosthetic use
- Counsel an amputee patient on stump care, phantom limb pain, and the stages of physical rehabilitation
- Describe the composition and roles of the multidisciplinary rehabilitation team in lower limb amputation rehabilitation
INSTRUCTIONS
Amputation of the lower limb is a life-altering event. The surgery itself, however skilled, is only the first step in a long journey of physical rehabilitation, psychological adjustment, and vocational reintegration. How a patient is counselled about what to expect — the stump, the prosthesis, the phantom limb pain, the rehabilitation timeline — determines how effectively they engage with that journey. A patient with realistic expectations and a clear understanding of their prosthetic options will work harder in physiotherapy, manage stump complications better, and return to function sooner than one who is left to discover these realities by accident. This module develops your knowledge of amputation levels, ideal stump characteristics, prosthetic principles, and the communication skills required to counsel an amputee patient and their family through the rehabilitation process.
References
- Maheshwari's Essential Orthopaedics, 6th ed, Ch 35 (Rehabilitation and Prosthetics) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 10 (Amputations) (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed, Ch 34 (Amputations and Prosthetics) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 32-year-old farmer sustains a severe crush injury to his right foot and lower leg when his tractor rolls over it. He is brought to your trauma centre in shock. After resuscitation, the surgical team assesses the leg and determines that a below-knee amputation is unavoidable — the tibial and peroneal vessels are irreparably destroyed and the soft tissue contamination is extensive. The surgery is necessary tonight. The patient is conscious and has been told the operation is needed. He grabs your hand and asks, 'Will I be able to walk again, doctor? Will I be able to work in my fields?' What do you tell him — and how do you prepare him for the rehabilitation ahead?
WHY THIS MATTERS
Lower limb amputation is not an uncommon event in Indian hospitals. The aetiology includes road traffic accidents, agricultural machinery injuries, diabetic foot disease (a rapidly growing category), peripheral vascular disease, malignant bone tumours, severe infections, and congenital limb deficiencies. For a young active patient, a below-knee amputation with a well-fitted patellar tendon bearing prosthesis allows return to near-normal walking, light farming, and in many cases employment. For an elderly diabetic patient, the rehabilitation pathway is more modest but still aims for community mobility with a prosthesis. The difference between an amputee who achieves independent walking with a prosthesis and one who becomes wheelchair-dependent often lies not in the surgical technique but in the quality of counselling, stump preparation, prosthetic fitting, and sustained physiotherapy engagement — all of which begin with what you tell the patient in those first post-operative days.
RECALL
Activate your foundational knowledge before proceeding. Recall the anatomy of the lower limb relevant to amputation: the major muscle groups of the thigh (quadriceps anteriorly, hamstrings posteriorly), the neurovascular bundle of the popliteal fossa, and the bony anatomy of the tibia and fibula in the leg. Recall the basic principles of wound healing — primary versus secondary intention, the role of blood supply, the significance of skin tension at a wound edge. Recall from your pharmacology what you know about neuropathic pain mechanisms — since phantom limb pain is a form of central sensitisation. Finally, recall the terms 'prosthesis' (an artificial replacement for a missing body part) and 'orthosis' (a device that supports or corrects a present limb) — they are commonly confused in clinical documentation.
Clinical Indications and Levels of Lower Limb Amputation
Provided image
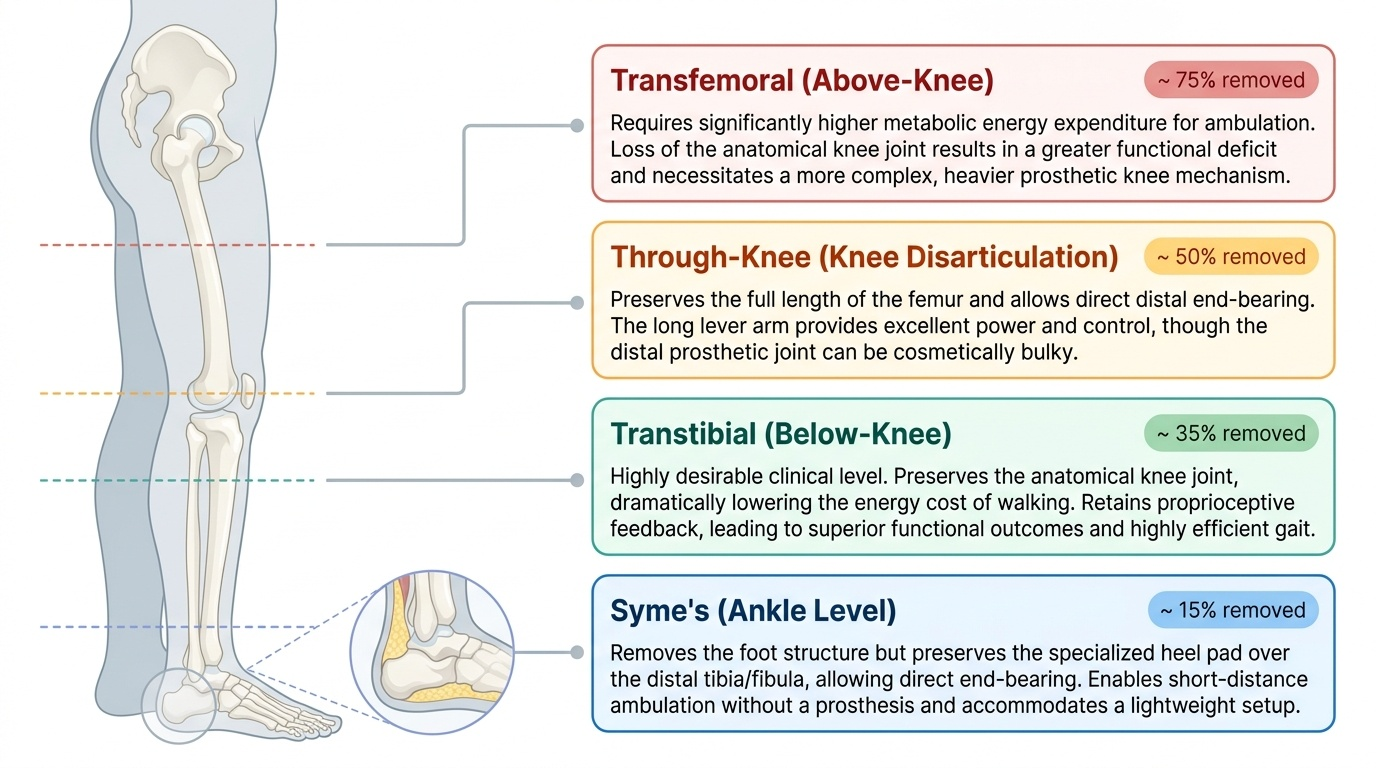
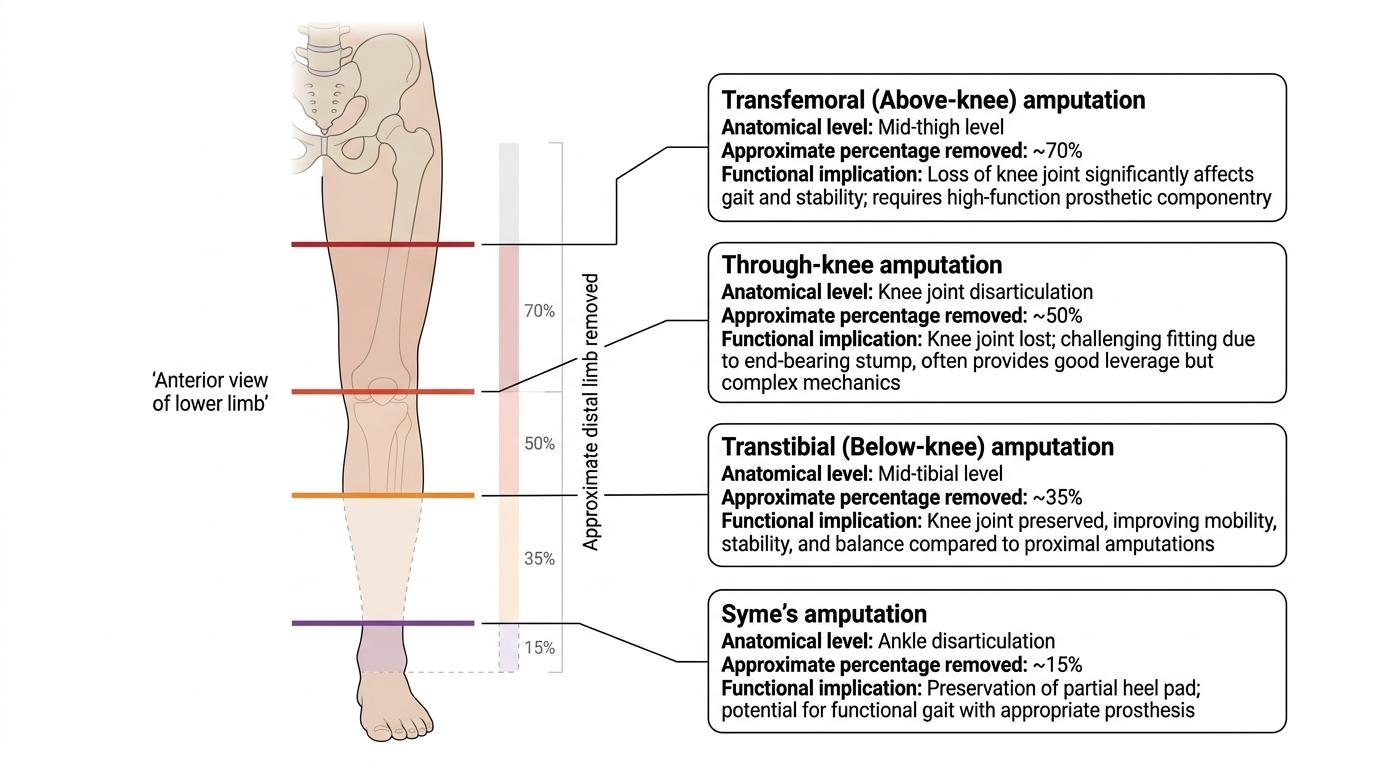
The level of amputation is one of the most consequential surgical decisions in orthopaedics because it directly determines which prostheses are available to the patient and, therefore, their potential functional outcome. The governing principle is to amputate at the most distal level that will produce a viable stump with adequate soft tissue coverage, adequate blood supply, and the potential for prosthetic use. More proximal amputations provide greater certainty of healing but impose a larger functional deficit. Less energy is consumed in ambulation with a below-knee prosthesis than with an above-knee prosthesis — this difference is clinically significant, especially in elderly patients.
The four main levels of lower limb amputation encountered in clinical practice are as follows:
Syme's amputation (ankle disarticulation with heel pad preservation) is performed at the level of the ankle joint, with removal of the foot and talus. The preserved heel pad, which is a specialised weight-bearing structure, is retained and used to cover the distal tibia and fibula. The resulting stump is end-bearing — the patient can put weight through the tip of the stump — which makes it suitable for a lightweight prosthesis. Syme's is indicated for severe forefoot or midfoot injuries and diabetic foot gangrene limited to the distal foot, provided the heel pad and its blood supply are intact. The prosthesis used is a Syme's prosthesis, which closely resembles the shape of the ankle and foot and is worn inside a normal shoe. Its limitation is cosmesis — the bulbous distal stump is visible under thin trouser materials.
Below-knee (transtibial) amputation is the most functionally desirable level in lower limb amputation because the knee joint is preserved, substantially reducing the energy cost of prosthetic walking and maintaining the proprioceptive feedback of the knee. The ideal tibia length is 12–18 cm measured from the tibial plateau (approximately mid-shaft tibia), providing enough lever arm for prosthetic control. The fibula is divided 1–2 cm proximal to the tibial cut to avoid a painful prominence. The key soft tissue principle is the creation of a long posterior myocutaneous flap (the posterior skew flap or Burgess long posterior flap) using the gastrocnemius-soleus muscle group, which provides good muscle padding over the bone ends and a robust blood supply to the skin. Below-knee amputation is indicated for crush injuries, vascular disease, and tumours of the foot and lower leg where the popliteal vessels are patent.
Through-knee (knee disarticulation) is performed at the level of the knee joint without disturbing the femur. It produces an inherently end-bearing stump (the femoral condyles provide a broad weight-bearing surface) and preserves the full length of the femur for prosthetic lever arm. It is indicated primarily when a below-knee level is not viable but the femur can be preserved, for example in some peripheral vascular disease cases or in paediatric patients where preserving the femoral growth plate matters. The main disadvantage is cosmesis — the bulky distal femoral condyles create difficulty fitting a prosthetic knee unit inside a trouser leg that matches the opposite limb.
Above-knee (transfemoral) amputation removes the limb above the knee joint, sacrificing both the tibia and the knee. It is indicated when the blood supply to the knee or below is irreparably compromised, when a tumour extends into the distal femur, or when a below-knee stump fails. The energy cost of walking with an above-knee prosthesis is substantially higher than with a below-knee prosthesis — above-knee amputees expend approximately 60–70% more energy per unit distance than normal walkers, compared to approximately 40% more for below-knee amputees. Elderly or comorbid patients may find above-knee prosthetic walking too energy-demanding for community ambulation and may rely on wheelchair mobility instead.
Lower Limb Amputation Levels and Functional Implications
Ideal Stump Characteristics and Stump Care
A functionally successful amputation rehabilitation depends critically on the quality of the stump. The stump is the interface between the patient's body and the prosthesis; its characteristics determine whether a prosthesis can be fitted at all, how comfortable it will be to wear, and how long it can be worn each day. The following characteristics define an ideal amputation stump, and each has a mechanistic basis that the counselling clinician should understand and be able to explain to the patient.
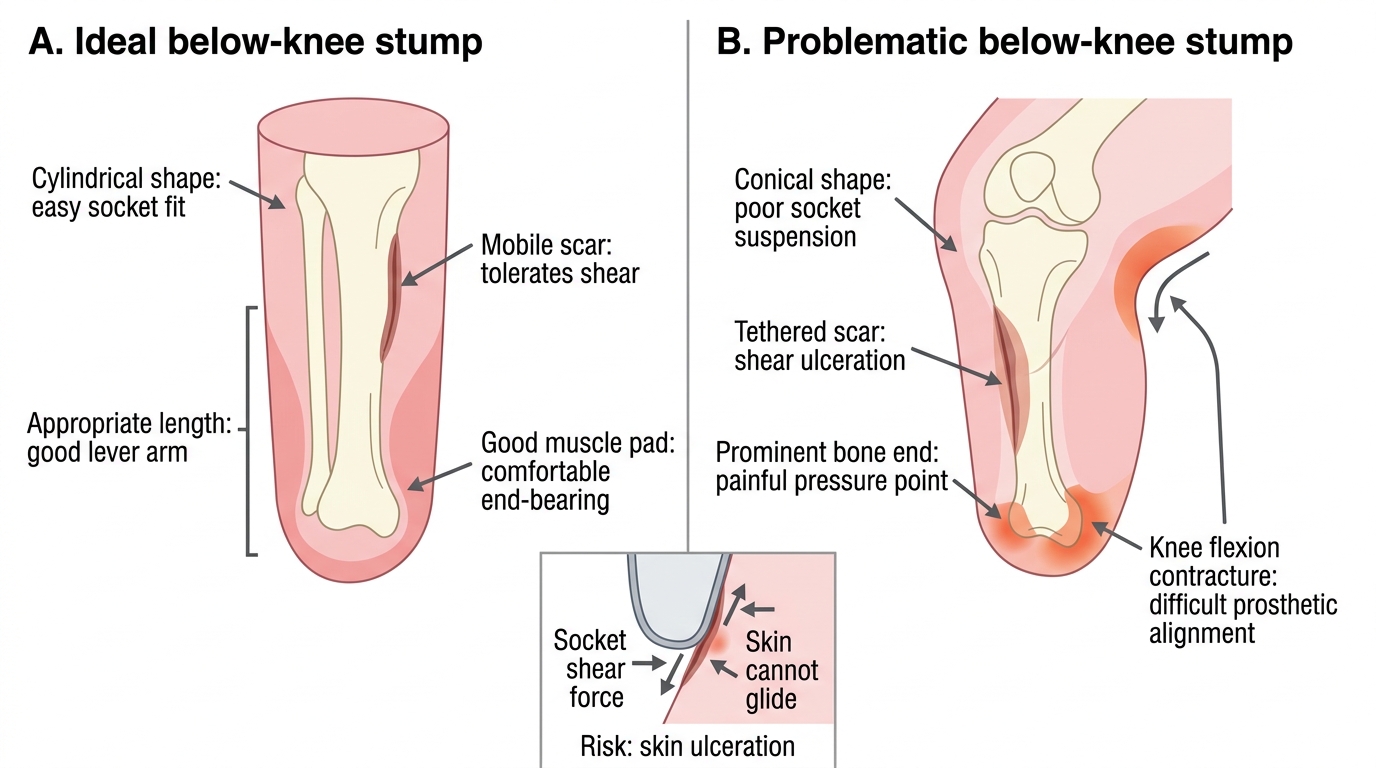
Adequate length: The stump must be long enough to provide a lever arm for prosthetic control, but not so long that there is insufficient soft tissue to cover the bone end comfortably. For a below-knee stump, 12–18 cm of tibia is the target range. A stump shorter than 8 cm of tibia (a 'very short below-knee stump') is difficult to fit and control prosthetically. A stump too long with inadequate soft tissue coverage over the bony tip will develop pressure necrosis under a prosthetic socket.
Cylindrical shape: An ideal stump is cylindrical (uniform diameter along its length), not conical (tapering to a point) or bulbous (wider at the tip). A cylindrical stump fills the prosthetic socket uniformly, distributing load evenly. A conical stump concentrates load at the tip, causing skin breakdown. Bandaging technique in the post-operative period is designed to achieve the cylindrical shape by applying firm pressure from distal to proximal (not the reverse).
Painless stump: Pain is the most common reason for prosthetic non-use. Sources of stump pain include neuromas (bulbs of regenerating axons at cut nerve ends — treated by burying the nerve in muscle during surgery; neuromas that become symptomatic later are treated by injection or surgical excision), bony prominences (inadequate bone rounding at the cut end), skin breakdown under prosthetic pressure, and infection. A patient should be counselled that stump pain in the first weeks is expected and managed with analgesia; persisting stump pain after 6 weeks requires clinical re-evaluation.
Non-adherent, mobile scar: The surgical scar must not be adherent to the underlying bone (a 'tethered scar'), as a tethered scar over a bony prominence causes pain and skin ulceration under prosthetic shear forces. The scar should be positioned away from the weight-bearing surface of the stump — ideally anterior or lateral. Scar mobilisation massage, begun once the wound is healed, prevents adhesion and maintains skin mobility.
Good muscle cover and soft tissue padding: Bone ends covered only by skin without adequate muscle interposition are prone to pressure necrosis under prosthetic sockets. The posterior myocutaneous flap in a Burgess below-knee amputation provides both the gastrocnemius-soleus muscle as padding and the skin from the calf — both tissues with superior vascularity compared to the anterior tibial skin.
No joint contracture: Above-knee stumps are prone to hip flexion and abduction contracture if the patient is allowed to rest with a pillow under the stump; below-knee stumps develop knee flexion contracture if the patient keeps the knee bent. Either contracture prevents proper prosthetic fitting. Active contracture-prevention exercises begin immediately post-operatively, and the patient is counselled not to rest the stump in a flexed or pillowed position.
Adequate skin condition: Healthy, well-vascularised skin is essential. Diabetic or vascular amputees may have compromised skin healing — these patients require more careful post-operative monitoring, slower prosthetic fitting timelines, and more frequent socket adjustments as the stump matures.
Ideal Versus Problematic Below-Knee Stump
SELF-CHECK
A patient has had a below-knee amputation 6 weeks ago. His stump is well-healed, but the scar is adherent to the anterior tibial surface. The most likely functional consequence of this finding is:
A. Phantom limb pain in the amputated foot
B. Knee flexion contracture preventing prosthetic socket fitting
C. Skin ulceration at the scar site under prosthetic shear forces
D. Neuroma formation at the cut posterior tibial nerve
Reveal Answer
Answer: C. Skin ulceration at the scar site under prosthetic shear forces
A scar adherent to the underlying bone (tethered scar) overlying a weight-bearing or high-shear-force zone will develop skin ulceration because normal skin tolerates shear only when it is mobile relative to the underlying structures. A tethered scar cannot slide under the prosthetic socket wall; instead, the skin is abraded and breaks down. This is why scar position (not over bone prominences) and scar mobilisation (post-healing massage to free adherence) are critical elements of stump preparation. Phantom limb pain arises from central sensitisation, not from the scar. Knee flexion contracture is a positioning complication. Neuromas are associated with cut nerve ends buried in scar, not with skin adherence.
Prosthetics for Below-Knee Amputation: Types and Counselling
The prosthesis is the technology that bridges between the stump and the function the patient seeks to restore. Counselling a below-knee amputee about prosthetics requires that you understand the basic types, their indications, their limitations, and the realistic functional expectations associated with each — since a patient who expects a prosthesis to feel 'exactly like a real foot' will be profoundly disappointed, while a patient who understands the learning curve and the genuine capabilities of a modern prosthesis will engage successfully with rehabilitation.
The patellar tendon bearing (PTB) socket is the standard prosthetic socket for below-knee amputation and the design most widely available in India's government prosthetic centres (through the ALIMCO scheme and Ayushman Bharat-supported prosthetic services). The name reflects its primary load-bearing design: in the original PTB socket, a shaped anterior brim applies firm pressure over the patellar tendon (the infra-patellar area), which is a pressure-tolerant soft tissue area, transferring weight from the stump to the socket. The socket is custom-moulded from the patient's stump impression to achieve an intimate fit. Weight-bearing is distributed across the patellar tendon anteriorly, the flares of the tibial condyles, the fibular shaft, and the popliteal fossa — with pressure relief over bony prominences (tibial crest, fibular head, distal fibula) carefully hollowed out.
Modern PTB socket variations include the total-surface bearing (TSB) socket, which uses a silicone liner worn over the stump to distribute load across the entire stump surface rather than selectively over pressure-tolerant areas. TSB sockets, when fitted with a locking pin mechanism, also provide suspension (keeping the socket on the stump) and proprioceptive feedback, and are associated with lower rates of skin breakdown in patients with good tissue quality. However, they are more expensive and less widely available through public prosthetic services in India.
Prosthetic feet are the distal component attached to the socket. The two main types are:
- SACH foot (Solid Ankle Cushion Heel): the most basic and widely available design, using a cushioned heel wedge to absorb heel strike energy and a rigid forefoot keel; no moving parts; durable and low-maintenance; appropriate for low-activity walkers and community-level ambulation. The SACH foot is the standard prosthetic foot in Indian government rehabilitation centres.
- Dynamic response (energy-storing) feet: use a carbon fibre keel (e.g. Seattle foot, Flex-Foot) that stores energy during loading and releases it at toe-off, mimicking the energy return of the Achilles tendon and calf musculature. They improve walking speed, reduce energy expenditure, and allow jogging and recreational sports. They are more expensive and less universally available but represent the standard in private prosthetic centres and for younger, active patients.
Suspension systems keep the socket on the stump. The simplest is a supracondylar cuff (a strap around the femoral condyles), which is adequate for most below-knee amputees. Silicone liners with pin-lock systems provide more secure suspension for active patients.
Counselling points for a below-knee amputee regarding their prosthesis:
- A below-knee prosthesis will allow walking — including community-level distances and, with a dynamic foot, recreational activities — but the gait will not feel identical to the pre-amputation gait. The learning curve is approximately 3–6 months of consistent physiotherapy.
- The stump will change shape (shrink, then stabilise) over the first 12–18 months as post-operative oedema resolves and the stump matures. Socket refitting is expected at 3 months, 6 months, and 12 months post-amputation. Patients who abandon physiotherapy after the initial fitting frequently find their socket no longer fits after stump maturation.
- The skin over the stump must be inspected daily for pressure areas, blisters, or redness. Any skin breakdown requires stopping prosthetic use and consulting the prosthetic team immediately — continuing to wear a prosthesis over a skin breakdown can convert a minor lesion into a major wound.
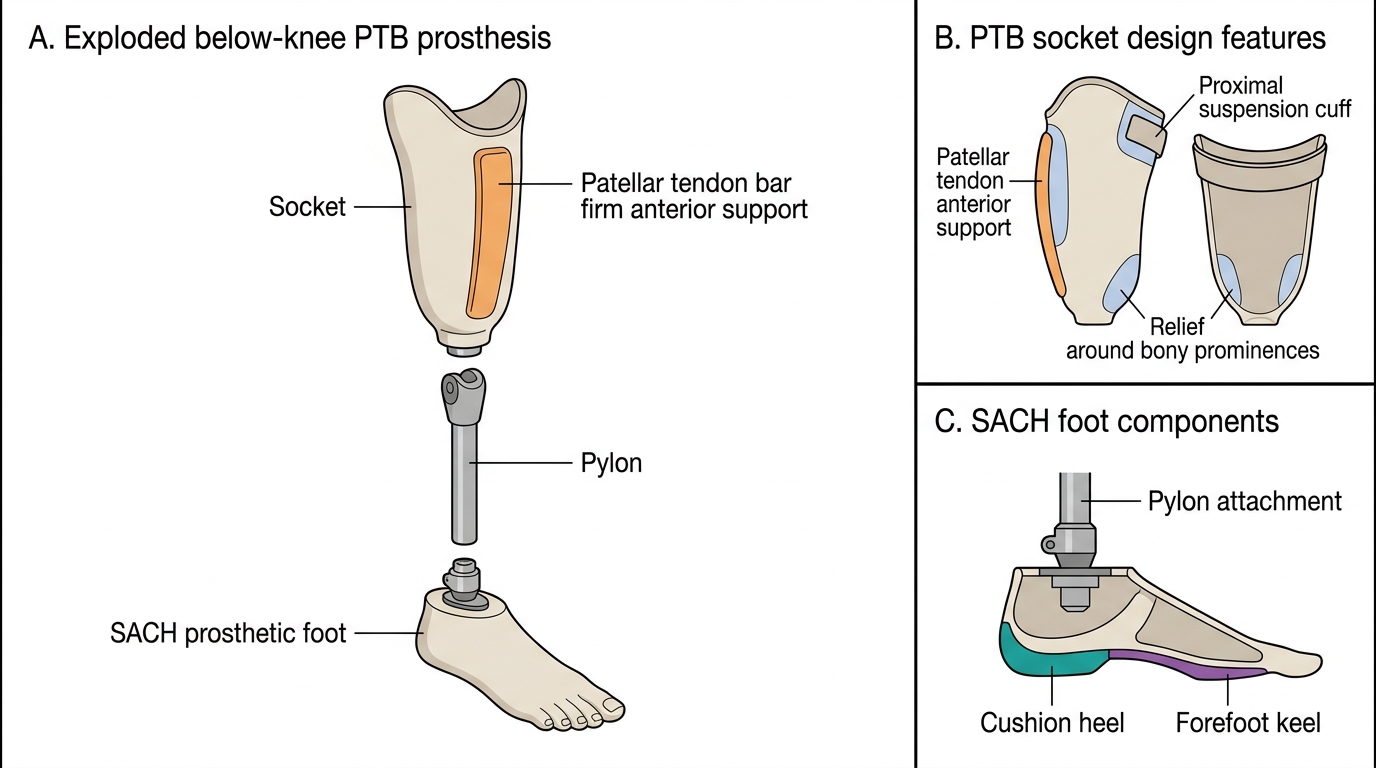
Below-Knee PTB Prosthesis: Exploded Components