Page 8 of 16
OR14.4 | Lower Limb Amputation Rehabilitation Counselling — SDL Guide (Part 2)
Phantom Limb Pain: Counselling and Management
Phantom limb pain is one of the most distressing and misunderstood sequelae of amputation, and inadequate counselling about its existence and nature is a significant source of patient distress and delayed rehabilitation. Understanding its neurophysiological basis enables you to counsel patients accurately and compassionately rather than dismissing it as 'psychological.'
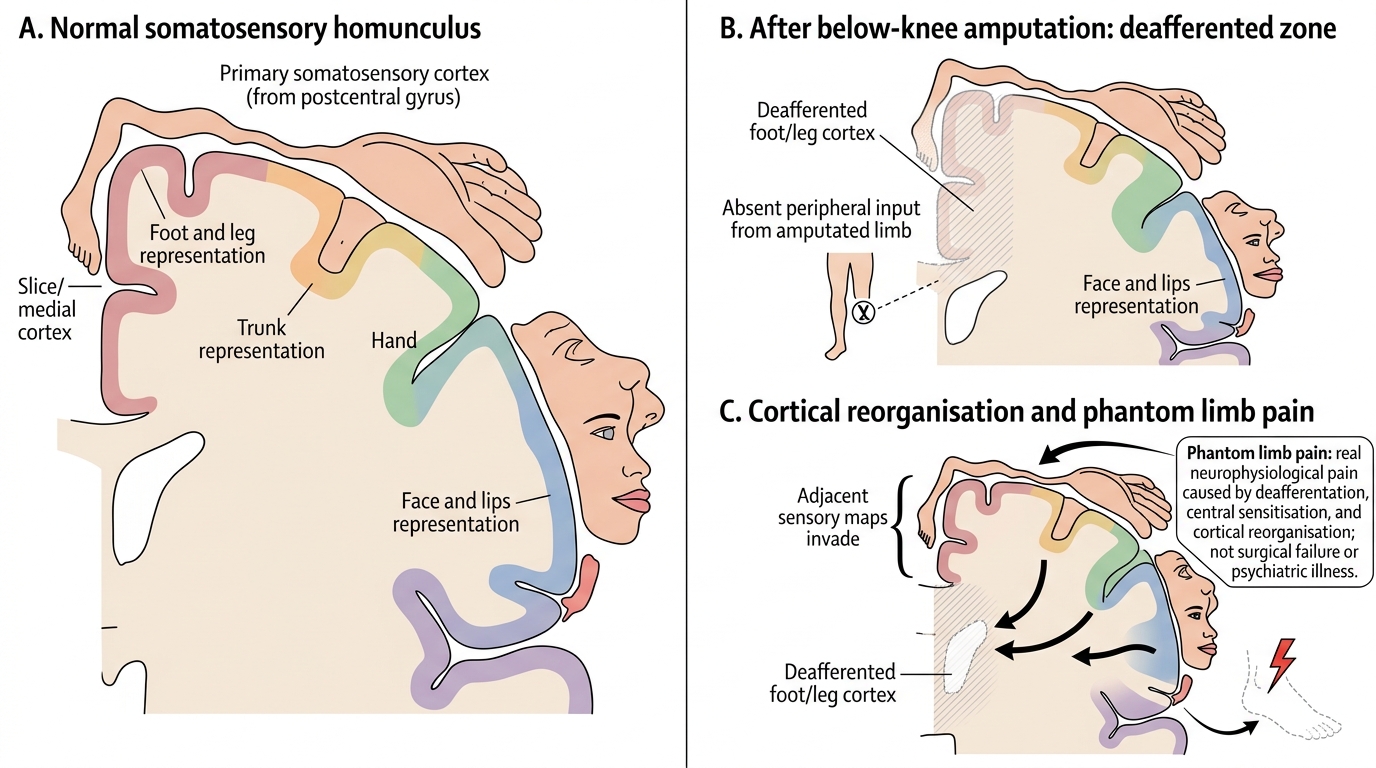
Phantom limb sensation — the perception that the amputated limb is still present — is experienced by approximately 70–80% of amputees. It arises because the cortical representation of the limb in the somatosensory cortex (the homunculus) does not immediately reorganise after amputation. The brain continues to receive and process 'signals' that it interprets as arising from the absent limb. Phantom sensation is usually not painful and may be helpful — the patient who perceives a phantom foot can 'feel' the position of their prosthetic foot, aiding proprioceptive adjustment during walking.
Phantom limb pain is pain perceived as arising from the absent limb — often described as burning, squeezing, cramping, or electric shock-like sensations. It is experienced by 60–80% of amputees to some degree, and is severe or disabling in approximately 10–15%. The neurophysiological basis involves cortical reorganisation after amputation: the deafferented cortical zone representing the amputated limb is 'invaded' by adjacent cortical representations (typically the face area, which abuts the hand area, or the genitalia area, which abuts the foot area in the homunculus). This reorganisation generates spontaneous and stimulus-triggered pain signals perceived as originating from the absent limb.
In counselling an amputee, the following points must be communicated:
- Phantom limb pain is real — it has a neurophysiological basis and is not imagined or 'in the mind.' Patients who are not told this often believe they are developing a psychiatric illness, which adds psychological distress to the physical pain.
- It is common. Knowing that 60–80% of amputees experience it reduces the patient's sense of being singled out by an incomprehensible symptom.
- For most patients it decreases over time (months to years), though it rarely disappears completely.
- It is treatable. First-line pharmacological agents include amitriptyline (a tricyclic antidepressant with sodium-channel blocking properties effective for neuropathic pain), gabapentin or pregabalin (calcium-channel modulators at the α2δ subunit, reducing central sensitisation), and topical or systemic analgesics. The mirror therapy technique — placing a mirror at the stump so that the reflection of the intact limb creates a visual illusion of the amputated limb — has Level II evidence for reducing phantom limb pain by exploiting the visual-motor mismatch hypothesis of cortical reorganisation.
- Early prosthetic use is itself therapeutic — proprioceptive inputs from the prosthesis accelerate cortical remapping and reduce phantom pain in many patients.
Stump pain must be distinguished from phantom pain, as the treatment differs. Stump pain is localised to the residual limb and has identifiable causes: neuromas, bony prominences, skin breakdown, infection, or socket pressure. Phantom pain is perceived in the absent limb. Patients often conflate the two — careful history-taking ('Is the pain in the part of the leg that is still there, or in the part that was removed?') usually distinguishes them.
Cortical Reorganisation in Phantom Limb Pain
SELF-CHECK
Three months after a below-knee amputation, a patient reports severe burning pain in the absent foot, especially at night. He is distressed and asks, 'Is this pain because something is wrong with the surgery?' The most appropriate response is:
A. Reassure him that this is normal and no treatment is needed
B. Explain that phantom limb pain is a recognised neurophysiological phenomenon affecting most amputees, that it is real and treatable, and discuss pharmacological and non-pharmacological options
C. Tell him the pain is psychological and refer him to a psychiatrist
D. Perform urgent imaging of the stump to exclude a neuroma requiring surgical excision
Reveal Answer
Answer: B. Explain that phantom limb pain is a recognised neurophysiological phenomenon affecting most amputees, that it is real and treatable, and discuss pharmacological and non-pharmacological options
Phantom limb pain is a recognised neurophysiological phenomenon (central sensitisation and cortical reorganisation after deafferentation) experienced by 60–80% of amputees. It is not a sign of surgical failure and not a psychiatric disorder. Simple reassurance without management is inadequate when the pain is severe. The appropriate response is to validate the patient's experience with an accurate explanation of the mechanism, quantify severity, and initiate treatment — first-line agents include amitriptyline, gabapentin/pregabalin, and mirror therapy. Imaging may be appropriate if stump pain (distinct from phantom pain) is suspected, but the described pain in the 'absent foot' is phantom pain, not stump neuroma pain.
Rehabilitation Team and Staged Rehabilitation Programme
Lower limb amputation rehabilitation is a multidisciplinary process that cannot be delivered by a single clinician. The rehabilitation team, the staged programme, and the realistic timeline are all essential elements of the counselling conversation — a patient who understands that their recovery has defined stages and clear milestones is far more likely to sustain engagement through the difficult early weeks. The journey from the operating table to independent community walking with a prosthesis involves at minimum six months of sustained physiotherapy and prosthetic adjustment, and requires coordinated input from surgeons, rehabilitation physicians, therapists, prosthetists, psychologists, and social workers. A patient who arrives at a prosthetic fitting appointment without having been told what to expect — that the initial socket will be uncomfortable, that gait will feel unnatural, that the stump will continue to change shape for a year — is a patient who is at high risk of abandoning the process. Your counselling, delivered from the first post-operative day, is what determines whether that patient reaches independent ambulation or becomes wheelchair-dependent for avoidable reasons.
The multidisciplinary rehabilitation team in a well-equipped orthopaedic rehabilitation setting comprises:
- Orthopaedic surgeon: responsible for the amputation procedure, stump wound management, and review for surgical complications (haematoma, wound dehiscence, bony prominence requiring revision).
- Physiatrist (Physical Medicine and Rehabilitation specialist): coordinates the overall rehabilitation programme, prescribes the prosthesis, and manages phantom pain and other post-amputation syndromes.
- Physiotherapist: delivers the exercise programme — pre-prosthetic (stump strengthening, range of motion, balance training, upper limb strengthening for crutch mobility) and prosthetic (gait training, balance, stair-climbing, slope and uneven-ground walking).
- Prosthetist and orthotist: designs, fabricates, and fits the prosthetic device; adjusts the socket as the stump changes shape over time.
- Occupational therapist: assists with activities of daily living adaptation, home modification recommendations, and return to work planning.
- Psychologist or counsellor: addresses body image disruption, depression, grief over the lost limb, and adjustment disorder — all of which are recognised psychological sequelae of amputation that, if unaddressed, impair rehabilitation engagement.
- Social worker: manages financial assistance applications (Ayushman Bharat, state disability schemes, ALIMCO prosthetic provision), transport to physiotherapy, and family support coordination.
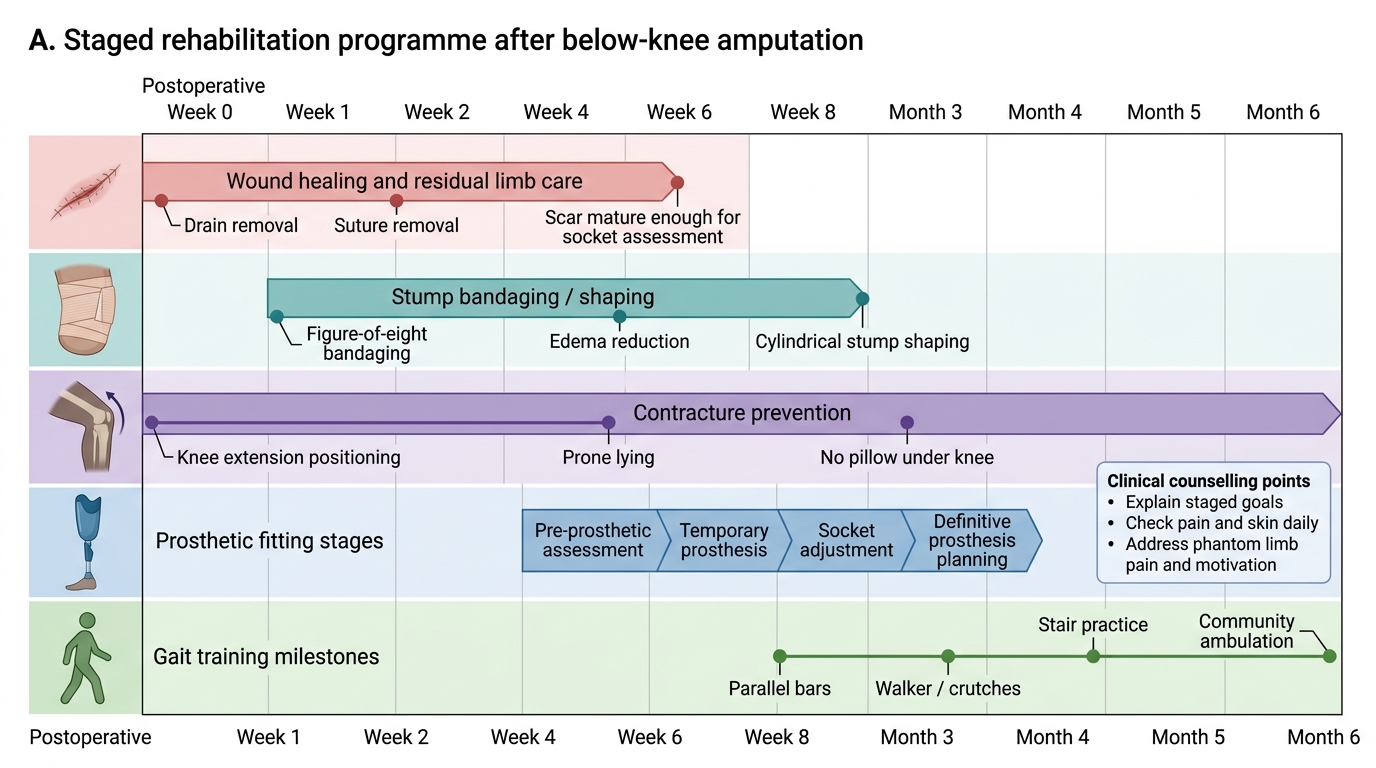
Staged rehabilitation programme for a below-knee amputee:
Pre-prosthetic phase (weeks 1–6): Wound healing, stump oedema reduction with graduated compression bandaging (applied distal to proximal), prevention of joint contractures, upper limb and core strengthening, balance training on one leg and with axillary crutches. This phase is critical — a stump that is allowed to remain oedematous and conical during this period will be much harder to fit with a socket later.
Preparatory prosthetic phase (weeks 6–12): Once the stump wound is fully healed and the volume is beginning to stabilise, a preparatory (training) prosthesis is fitted. Initial standing in the parallel bars, then stepping, then walking with the prosthesis under physiotherapy supervision. Energy expenditure is high in this phase; the patient must be counselled that fatigue is normal and will improve.
Definitive prosthetic fitting (months 3–6): A definitive (permanent) prosthesis is fitted once stump maturation is complete. Gait training advances to community walking, slope negotiation, public transport boarding, and return-to-work activities. For agricultural patients, this includes specific training for walking on uneven terrain.
Long-term follow-up: Annual or biannual review with the prosthetic team for socket adjustments, replacement of worn components, and monitoring for late stump complications (skin breakdown, socket-induced pressure ulcers, contralateral limb overload).
The realistic timeline for a healthy young adult with a traumatic below-knee amputation to achieve independent community walking with a prosthesis is 4–6 months. For an elderly diabetic patient, the timeline is longer (6–12 months) and independent community walking may not be achievable — household ambulation and standing transfers may be the realistic goal.
Rehabilitation Timeline After Below-Knee Amputation
Self-Assessment: Integrating Amputation Knowledge with Counselling Practice
The following self-assessment tasks test your ability to integrate knowledge of amputation levels, ideal stump characteristics, prosthetic principles, and phantom limb pain management into a coherent counselling approach.
Knowledge check A: List from memory the six characteristics of an ideal amputation stump and give one sentence on the clinical consequence if each is absent.
Expected answer: (1) Adequate length — insufficient lever arm for prosthetic control if too short; (2) cylindrical shape — concentrated load at stump tip causing pressure necrosis if conical; (3) painless — prosthetic non-use if pain persists; (4) non-adherent scar — skin ulceration from shear forces if adherent to bone; (5) good muscle cover — pressure necrosis of skin over bone end if no padding; (6) no joint contracture — inability to fit prosthetic socket if contracture present. You might also add adequate skin quality as a seventh characteristic for vascular/diabetic amputees.
Counselling scenario B: A 65-year-old diabetic man with a right below-knee amputation for diabetic foot gangrene is 8 weeks post-operation. The wound is fully healed. His stump is conical, and there is 6 cm of viable tibia below the knee. His son asks you whether his father will ever walk again with a prosthesis. What do you counsel?
Discussion: The stump, while short (6 cm below the tibial plateau is at the lower edge of fittable length — some prosthetists consider 6–8 cm as a 'very short BK' but still potentially fittable with a specialised socket), is healed. The conical shape requires correction with graduated compression bandaging before fitting. The age and diabetic status mean skin integrity must be monitored carefully under the prosthesis. The counselling should be honest about the limitations — 6 cm is a challenging stump length — while not dismissing the possibility. A trial fitting with a preparatory prosthesis is the appropriate next step, with the goal of household ambulation (not community walking) as the initial target. If a below-knee fitting is not achievable, a through-knee level would have been preferable for end-bearing capacity.
Scenario C: A 28-year-old man undergoes an above-knee amputation for osteosarcoma. Two weeks post-operatively, he asks you, 'Can I use a prosthesis and walk normally again?' What are the key points in your counselling?
Discussion: Above-knee prosthetic walking is achievable for a young, motivated patient. The prosthesis includes a prosthetic knee joint (with different mechanisms from a simple hinge, e.g. polycentric or hydraulic) and a prosthetic foot. Walking speed and energy expenditure will be higher than with a below-knee prosthesis, but community-level ambulation is a realistic target. The learning period is longer (6–12 months) and requires intensive physiotherapy. Return to work depends on the nature of the work — office or light work is realistic; heavy physical labour is generally not. For osteosarcoma, the oncological prognosis (approximately 60–70% 5-year survival for localised disease) should be discussed separately by the oncology team, but the rehabilitation counselling can proceed in parallel with chemotherapy, once stump wound healing is complete.
After working through these scenarios, identify one area of amputation rehabilitation counselling where you feel least confident. For most final-year students, this is phantom limb pain management — the pharmacology is often poorly remembered. Review the first-line agents (amitriptyline, gabapentin/pregabalin, mirror therapy) before your internship posting in orthopaedics.
Lower Limb Amputation Quick Reference
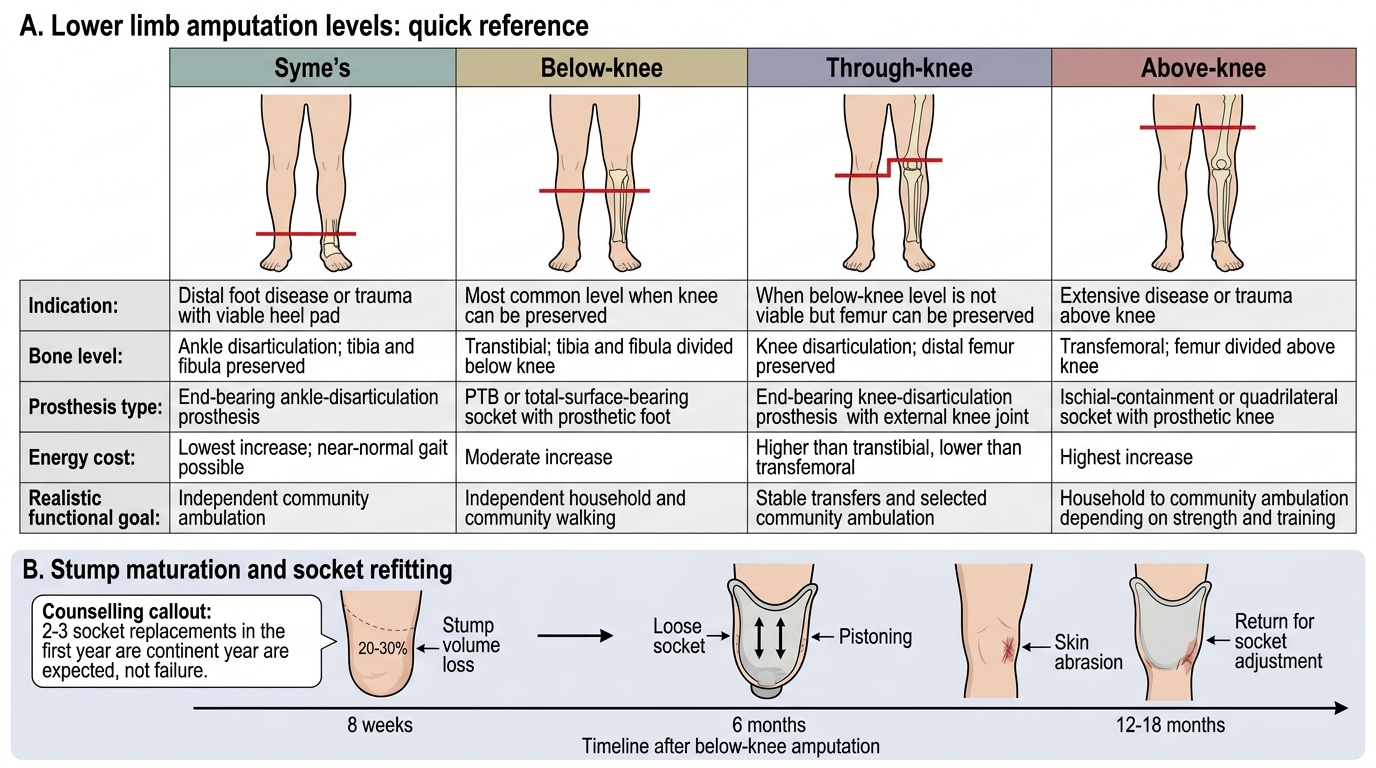
CLINICAL PEARL
The single most common preventable cause of prosthetic non-use in Indian below-knee amputees is socket ill-fit due to stump shape changes after early fitting. The stump loses approximately 20–30% of its volume over the first 12–18 months as post-operative oedema resolves and muscle atrophy stabilises. A socket fitted at 8 weeks post-amputation will be significantly too loose by 6 months, causing pistoning (the stump moving up and down in the socket), skin abrasion, and a prosthesis that feels unreliable. Counsel every patient that two to three socket replacements in the first year are not a sign of failure — they are the expected course of stump maturation. The patient who understands this will return for socket adjustments; the patient who is not told will simply stop wearing the prosthesis.