Page 4 of 13
OR2.8 | Spine Injury Mobilisation Principles — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis and mechanism of injury in spinal column injuries, including flexion, extension, rotation, and axial loading patterns
- Classify spinal injuries using the ASIA Impairment Scale and the Thoracolumbar Injury Classification and Severity Score (TLICS)
- Recognise the clinical features of spinal cord injury including neurological levels and spinal shock
- Apply safe spinal precautions and the log-roll technique in the initial assessment and mobilisation of a spine-injured patient
- Outline the principles of definitive management including immobilisation, steroid use controversy, decompression, and rehabilitation
INSTRUCTIONS
Spinal cord injury (SCI) is a catastrophic event with lifelong consequences for the patient. The majority of secondary neurological deterioration following SCI is preventable, and an important fraction occurs in the prehospital and emergency room phases due to incorrect handling. A final-year student must understand why the spine must be protected, how to maintain neutral alignment during log-roll and transfer, when to apply and remove a cervical collar, and how to distinguish a complete from an incomplete spinal cord injury — because an incomplete injury can be converted to a complete one by a single careless movement. Competency OR2.8 demands mastery of both the injury science and the safe-mobilisation practice.
References
- Maheshwari's Essential Orthopaedics, Ch on Spine Injuries (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Spinal Injuries chapter (textbook)
- ATLS Advanced Trauma Life Support, 10th Edition — Spine Injury management (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old man is brought to the emergency department after diving into a shallow pool. He is conscious but cannot move his arms or legs. He tells the paramedics his neck hurts. The paramedics applied a cervical collar in the field and transferred him on a spinal board. In the resuscitation bay, a nurse reaches across to take his blood pressure and inadvertently moves his neck. The patient cries out. The registrar asks you to help perform a log-roll examination. As you prepare, you ask yourself: Do you have enough people? Are you the one controlling the head? What are you looking for, and how will your finding change the management?
WHY THIS MATTERS
Traumatic spinal cord injury occurs in approximately 15–40 per million population annually in India, predominantly affecting young men in their productive years. The consequences are devastating: complete cervical SCI produces quadriplegia and lifelong dependence, while lumbar injuries cause paraplegia and autonomic dysfunction. Critically, up to 25% of spinal cord injuries occurring AFTER trauma result from improper handling during transport, emergency room management, or nursing care — these secondary injuries are entirely preventable. As the doctor supervising emergency care, you are responsible for ensuring that every patient with a suspected spine injury receives meticulous spinal precautions until injury is clinically and radiologically excluded. Additionally, distinguishing a complete from incomplete injury, applying the ASIA scale, and understanding TLICS guides the surgical decision that may restore function.
RECALL
Recall the spinal anatomy: 7 cervical, 12 thoracic, 5 lumbar vertebrae, the sacrum, and coccyx. The spinal canal runs through the vertebral foramina; the cord ends at L1-L2 (conus medullaris), continuing as the cauda equina (nerve roots) below. The stability of the spinal column depends on the three-column model (Dennis): anterior column (vertebral body anterior half + ALL + annulus), middle column (posterior vertebral body + PLL + posterior annulus), and posterior column (facets, pedicles, spinous processes, supraspinous and interspinous ligaments). Disruption of two or more columns = unstable fracture. Recall also dermatomes and myotomes for neurological level assessment.
Aetiopathogenesis and Mechanism of Injury
Spinal injuries result from forces that exceed the combined tensile, compressive, and rotational strength of the vertebral column and its supporting ligamentous structures. Understanding the mechanism is not merely academic — it predicts the fracture pattern, the direction of cord compromise, and the appropriate surgical approach.
The spine has two mechanically vulnerable transition zones: the cervicothoracic junction (C7-T1, where a mobile cervical spine meets the rigid thoracic cage) and the thoracolumbar junction (T12-L2, where the rigid thoracic spine transitions to the more mobile lumbar spine). These zones concentrate stress and are the most common sites of traumatic injury. Approximately 60% of all spinal fractures occur in the thoracolumbar region; the cervical spine accounts for 30%, and pure thoracic fractures are uncommon because the rib cage provides splinting.
Mechanisms and resulting fracture patterns:
1. Flexion injury — forward bending compresses the anterior column while tensing the posterior column. Results in anterior wedge compression fractures. If flexion is severe, the posterior ligaments rupture, producing a flexion-distraction (Chance) injury. Pure flexion compression fractures that maintain ≥50% anterior column height and have intact posterior ligaments are usually stable.
2. Axial compression (burst) — vertical loading compresses the vertebral body circumferentially, driving the nucleus pulposus through the endplate and shattering the vertebral body. The posterior wall fragments are propelled into the spinal canal, compressing the cord or cauda equina. Burst fractures are potentially unstable and must be distinguished from simple compression fractures by CT (retropulsed fragment, posterior wall breach).
3. Flexion-rotation — combined flexion and rotation disrupts all three columns, producing fracture-dislocations with complete ligamentous instability. These are among the most neurologically dangerous injuries; translation of one vertebra on another directly compresses or shears the cord.
4. Extension injury — hyperextension compresses the posterior column while tensing the anterior column. Seen in cervical spine injuries from rear-end collisions (whiplash) and in falls in elderly patients with spondylotic spines. The narrowed spondylotic canal is particularly vulnerable; minor extension can produce central cord syndrome without a fracture.
5. Distraction (Chance fracture) — a seatbelt acting as a fulcrum during sudden deceleration creates a horizontal shearing force through the posterior and middle columns. The fracture runs horizontally through bone (bony Chance) or ligament (ligamentous Chance), dividing the spine into upper and lower halves. Associated with intra-abdominal organ injuries (30%).
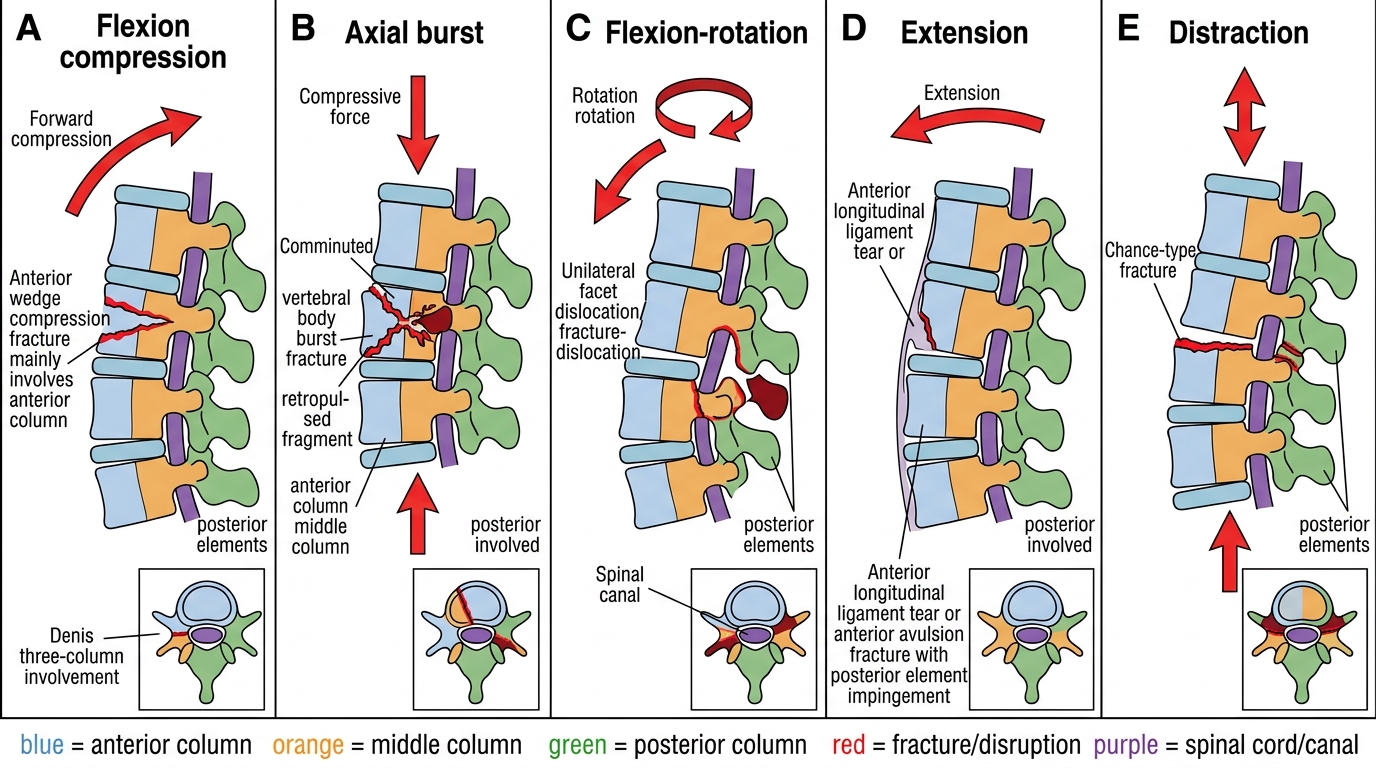
Mechanisms of Spinal Injury and Column Involvement
Pathophysiology of spinal cord injury: Primary injury occurs at the moment of impact — direct contusion, laceration, or compression of the cord. Secondary injury evolves over hours to days through ischaemia, oedema, glutamate excitotoxicity, lipid peroxidation, and inflammatory cell infiltration, progressively extending the zone of cord damage. This secondary injury cascade is the therapeutic target — interventions that reduce cord oedema (maintaining perfusion pressure, avoiding hypotension/hypoxia) and decompress the cord early may limit the secondary injury and improve neurological outcome.
Classification: ASIA Impairment Scale and TLICS
Two classification systems are essential for clinical decision-making in spinal injuries and must be mastered before any management plan can be defended. The ASIA (American Spinal Injury Association) Impairment Scale grades the completeness of spinal cord injury based on systematic neurological examination and predicts prognosis with remarkable reliability — a single finding of preserved sacral function separates a 'complete' injury with poor recovery potential from an 'incomplete' injury where substantial neurological return is possible. The Thoracolumbar Injury Classification and Severity Score (TLICS) integrates three independent injury characteristics into a numerical score that directly guides the conservative-versus-surgical decision, removing much of the historical subjectivity from spinal fracture management. These two systems work together: TLICS tells you whether to operate, and ASIA tells you how urgently and why.
ASIA Impairment Scale (AIS):
The neurological assessment systematically tests motor function (key muscle groups at each level) and sensation (light touch and pin-prick at each dermatomal level) to define the neurological level of injury (NLI — the most caudal segment with normal function bilaterally) and classify injury completeness:
- ASIA A (Complete): No motor or sensory function preserved in sacral segments S4-S5. This includes absence of deep anal pressure sensation. Prognosis for neurological recovery is poor.
- ASIA B (Incomplete — sensory only): Sensory but no motor function below the NLI, including S4-S5.
- ASIA C (Incomplete — motor non-functional): Motor function preserved below NLI; more than half of key muscles have grade <3 (cannot resist gravity).
- ASIA D (Incomplete — motor functional): Motor preserved below NLI; at least half of key muscles grade ≥3.
- ASIA E (Normal): Motor and sensory function normal; may still have pain.
The sacral sparing concept is crucial: even one remaining function below the gross neurological level — voluntary anal sphincter contraction, perianal sensation, big toe flexor activity — classifies the injury as INCOMPLETE (B, C, or D), which carries a dramatically better prognosis than ASIA A. Always test S4-S5 meticulously.
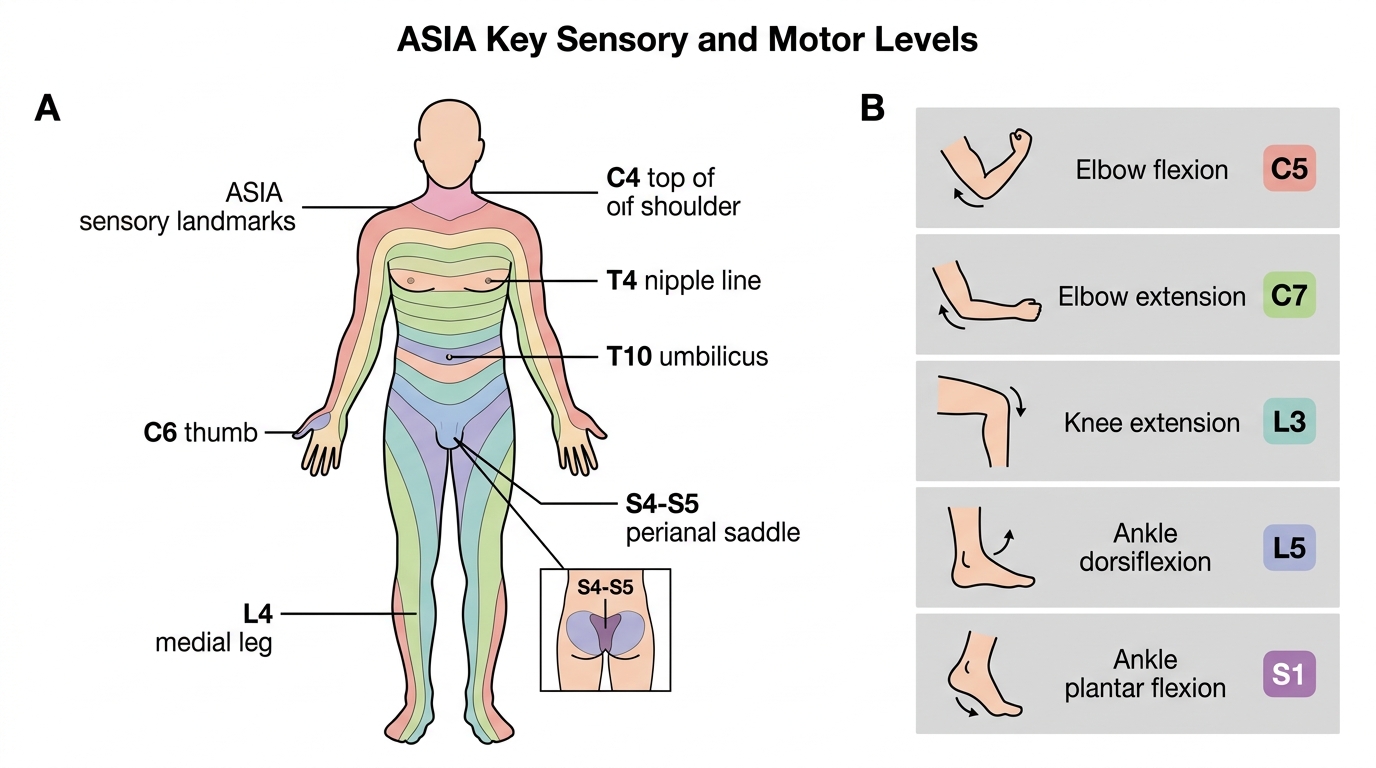
ASIA Key Dermatome and Myotome Levels
Thoracolumbar Injury Classification and Severity Score (TLICS):
TLICS scores three independent injury characteristics to guide management:
| Parameter | Finding | Points |
|---|---|---|
| Morphology | Compression | 1 |
| | Burst | 2 |
| | Translation/rotation | 3 |
| | Distraction | 4 |
| Posterior ligamentous complex (PLC) | Intact | 0 |
| | Suspected/indeterminate | 2 |
| | Disrupted | 3 |
| Neurological status | Intact | 0 |
| | Nerve root involvement | 2 |
| | Complete cord injury | 2 |
| | Incomplete cord injury | 3 |
TLICS <4 → conservative management; TLICS >4 → surgical management; TLICS =4 → either.
An important nuance: a patient with an incomplete cord injury (ASIA B-D) scores HIGHER on TLICS than a complete injury (3 vs 2 for neurological status), because early surgical decompression offers meaningful recovery potential in incomplete injuries that it cannot provide in complete injuries.
Cervical spine management follows similar principles. The Subaxial Cervical Spine Injury Classification (SLIC) parallels TLICS. Additionally, specific upper cervical injuries (atlantoaxial fractures — Jefferson burst of C1, odontoid fractures of C2, Hangman's fracture of C2 pedicles) follow distinct classification and management pathways.
SELF-CHECK
A 30-year-old has a T10 burst fracture after a fall. TLICS calculation: morphology = burst (2 points) + posterior ligamentous complex disrupted (3 points) + incomplete cord injury ASIA C (3 points) = 8 points. What is the appropriate management?
A. Conservative management with thoracolumbar brace alone
B. Surgical decompression and stabilisation
C. Halo traction for 12 weeks
D. Bedrest with serial X-rays monitoring
Reveal Answer
Answer: B. Surgical decompression and stabilisation
TLICS of 8 (>4) indicates surgical management. Crucially, the incomplete neurological deficit (ASIA C) makes decompression especially important because neurological recovery is possible if cord compression is relieved early. An incomplete injury scores 3 on the neurological domain — higher than a complete injury — precisely because surgery can make a meaningful difference. Conservative management (option A) would be appropriate only for TLICS <4.
Clinical Features and Examination
Assessment of a suspected spinal injury patient must follow ATLS principles at every stage: life-threatening injuries — airway obstruction, tension pneumothorax, major haemorrhage — always take precedence over spinal evaluation, and spinal precautions are maintained throughout this process without interrupting resuscitation. Once the patient is haemodynamically stabilised, a calm and systematic neurological examination is performed to define the neurological level of injury, the completeness of cord damage, and to identify any of the recognised incomplete cord syndromes. This examination must be documented clearly and time-stamped, because a change in neurological status — either deterioration or improvement — between two examinations is one of the most important clinical findings in spinal injury management, directly altering the surgical urgency. Never delegate the first detailed neurological examination to a nurse; a doctor must perform and record it.
Symptoms suggesting spinal injury:
- Neck or back pain after trauma, especially axial tenderness over the vertebral column
- Limb weakness or paralysis, particularly bilateral
- Sensory level — a band of altered sensation across the trunk
- Loss of bladder or bowel control (urinary retention or incontinence, faecal incontinence)
- Priapism (sustained penile erection in male patients — a sign of sympathetic disruption)
- Respiratory difficulty (diaphragm C3-C5; intercostals T1-T12) — cervical injuries above C5 may require ventilatory support
Spinal shock must be distinguished from neurogenic shock:
- Spinal shock — transient cessation of all spinal cord function (motor, sensory, AND reflexes) below the level of injury immediately following SCI. It resolves over hours to days, and the return of the bulbocavernosus reflex (anal sphincter contraction on penile/clitoral squeeze or catheter tug) marks the end of spinal shock. Only AFTER spinal shock has resolved can the ASIA grade be considered definitive.
- Neurogenic shock — a haemodynamic phenomenon resulting from loss of sympathetic tone below the cervical/upper thoracic injury level, producing vasodilation and relative bradycardia despite hypotension (the triad: hypotension + bradycardia + warm/dry peripheries). Distinguished from haemorrhagic shock (which produces tachycardia and cool, clammy peripheries). Treatment includes vasopressors (norepinephrine preferred) and careful fluid resuscitation; avoid excessive fluids (risk of pulmonary oedema with lost cardiac sympathetics).
Clinical cord syndromes (incomplete injuries with recognisable patterns):
- Central cord syndrome — most common incomplete SCI; hyperextension in a spondylotic cervical spine in elderly patients; disproportionate weakness of arms > legs; bladder dysfunction. Significant spontaneous recovery likely.
- Brown-Séquard syndrome — hemisection of the cord; ipsilateral motor loss and proprioception loss PLUS contralateral pain and temperature loss (spinothalamic crossing at 2 levels). Best prognosis of all incomplete syndromes.
- Anterior cord syndrome — damage to the anterior two-thirds of the cord (anterior spinal artery territory); loss of motor function and pain/temperature sensation BELOW the level; preserved proprioception and vibration (posterior columns intact). Worst prognosis among incomplete syndromes.
- Cauda equina syndrome — injury below L1-L2 affects the nerve roots of the cauda equina, not the cord itself; produces lower motor neuron features: flaccid paralysis, saddle anaesthesia (S3-S5), urinary retention, faecal incontinence. A surgical emergency — emergent decompression within 24-48 hours preserves bladder/bowel function.
- Conus medullaris syndrome — injury at L1-L2 produces a mixed UMN + LMN picture; variable bladder/bowel and sexual dysfunction.
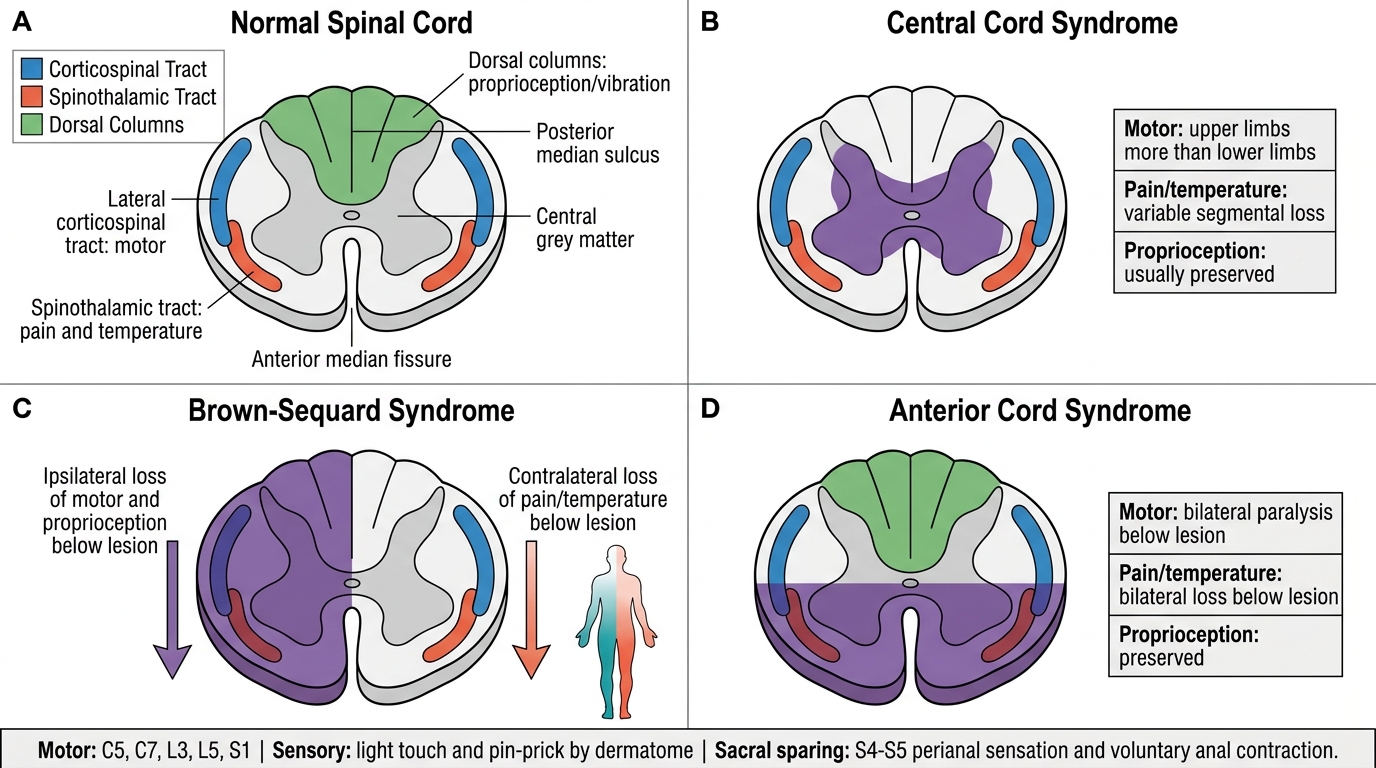
Spinal Cord Syndromes: Tracts and Deficit Patterns
Mandatory examination components:
1. Motor examination — 5 key muscles per side (C5 elbow flexors, C7 elbow extensors, L3 knee extensors, L5 ankle dorsiflexors, S1 ankle plantar flexors) graded 0-5
2. Sensory examination — light touch AND pin-prick at each dermatomal level
3. Perianal sensation and voluntary anal sphincter contraction (S4-S5 — sacral sparing)
4. Bulbocavernosus reflex
5. Abdominal reflexes and lower limb deep tendon reflexes
Imaging:
- Plain X-rays (AP + lateral) are the initial investigation; look for vertebral body height loss, kyphotic angulation (>10°), interspinous distance widening (posterior ligament disruption), translation
- CT scan (gold standard): delineates fracture morphology, canal compromise, retropulsion; mandatory for unstable or complex injuries and before surgical planning
- MRI scan: mandatory for any neurological deficit — defines cord injury extent (contusion, haematoma, oedema), disc herniation, epidural haematoma, posterior ligamentous complex integrity. Cannot replace CT for bony detail.