Page 5 of 13
OR2.8 | Spine Injury Mobilisation Principles — SDL Guide (Part 2)
Spinal Precautions and Safe Mobilisation: Log-Roll Technique
Provided image
Safe mobilisation of the spine-injured patient is the most clinically actionable skill for a house officer, and it is the domain where preventable secondary neurological injury most often occurs. The fundamental principle of spinal precautions is maintaining neutral spinal alignment throughout every patient movement — preventing any flexion, extension, axial rotation, or lateral bending that could displace an unstable fracture fragment into the cord or worsen cord compression from an expanding haematoma. This principle applies not only to formal log-rolls but to every mundane interaction with the patient: helping them drink, adjusting the bed position, taking blood pressure, performing a rectal examination, inserting a urinary catheter. Every movement of a spinal-precautions patient requires a plan and a designated spinal guardian — if no plan exists, the movement should not occur until one does. This section teaches you how to execute these principles, from the choice of immobilisation device in the field to the formal four-person log-roll in the emergency room.
Spinal immobilisation in the field and emergency room:
- Cervical collar: a semi-rigid collar (Philadelphia, Aspen, Miami-J) maintains neutral cervical alignment. It does NOT completely immobilise the cervical spine (residual motion at C1-C2 is significant); it serves primarily as a reminder to handlers. The collar must be the correct size (chin supported, no extension forced). Prolonged collar use causes pressure sores on the occiput and mandible, increases intracranial pressure, and increases dysphagia risk — remove as soon as spinal injury is cleared clinically and radiologically.
- Long spinal board: used for extraction and transport; the patient must be transferred off the board as soon as possible in the ED — prolonged board use causes pressure ulceration within 2 hours. Transfer to a hospital bed or vacuum mattress on arrival.
- Vacuum mattress: preferred for prehospital immobilisation over rigid boards; conforms to body contours, provides better immobilisation with less pressure injury risk.
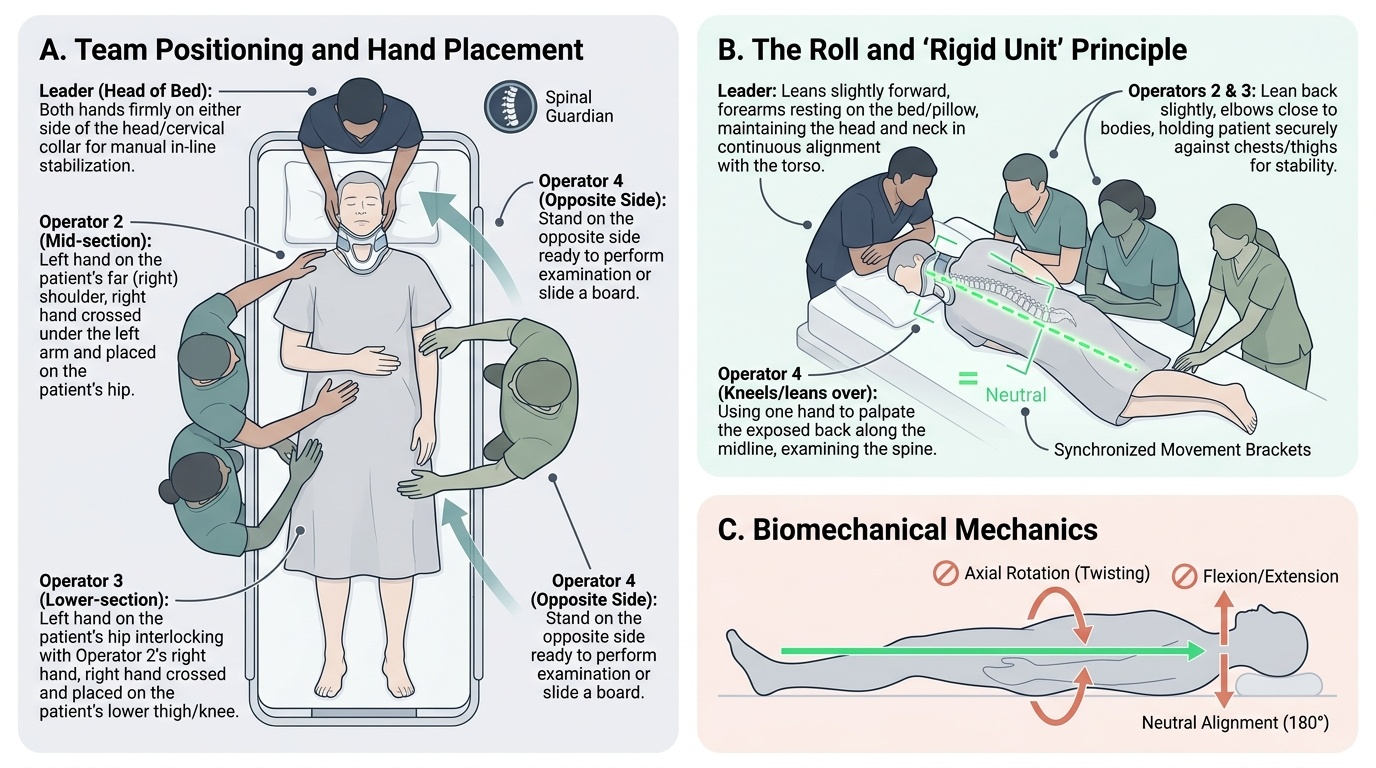
The log-roll procedure is the standard method for examining the posterior spine, inserting a urinary catheter, placing a pressure-relieving mattress, or turning the patient. It requires coordinated movement of the whole body as a rigid unit.
Minimum team for log-roll: 4 people (ideally 5 for obese patients or thoracolumbar injuries):
1. Leader at the head — commands the roll; maintains cervical spine in neutral alignment using both hands in-line stabilisation. This is the most skilled role; the team leader must be here. The leader calls "On my count: roll."
2. Shoulder/chest person — controls the shoulder girdle and upper chest
3. Pelvis person — controls the pelvis and hips (NOT the legs alone)
4. Legs person — controls the lower limbs in neutral alignment
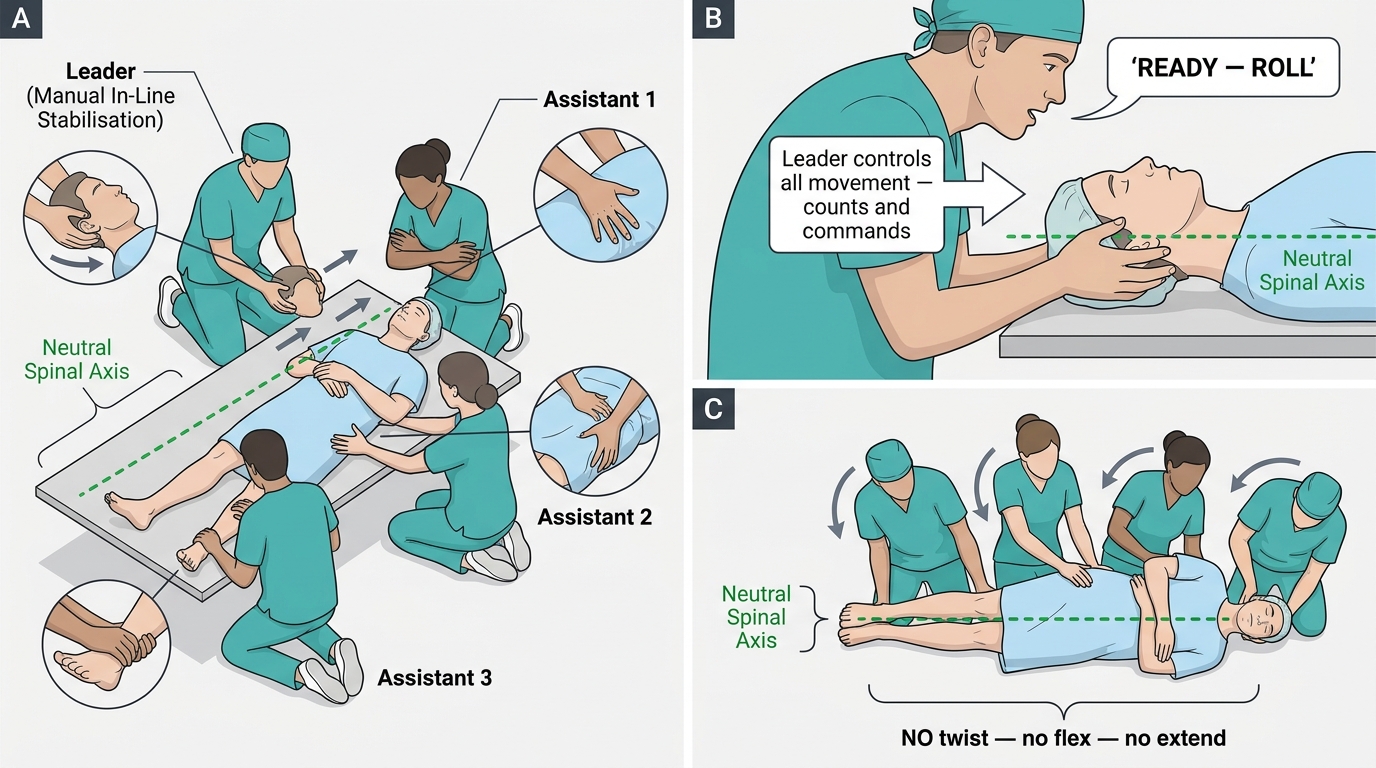
Log-roll steps:
1. Ensure adequate analgesia (roll is painful)
2. Leader at head applies manual in-line stabilisation and directs team positioning
3. All team members kneel/stand on the SAME side (the side the patient will roll AWAY from)
4. Team members place their hands without crossing arms
5. On the leader's count ("1-2-3 ROLL"), the patient is rolled as a rigid unit — the head, spine, and pelvis rotate together without relative motion between segments
6. Posterior spine examined, perineum inspected if needed
7. On the leader's count, the patient is returned to supine
8. The cervical collar is reapplied; manual in-line stabilisation is maintained until the collar is secured
Four-Person Log-Roll Technique: Team Positions and the Rigid Unit Principle
Clearance of cervical spine (removing collar):
- Clinical clearance (NEXUS criteria / Canadian C-spine Rule) — the collar may be removed WITHOUT imaging in patients who are: alert and cooperative; no distracting injury; no posterior midline tenderness; no neurological deficit; no intoxication. Low-risk mechanism (Canadian C-spine Rule) allows clinical clearance.
- Radiological clearance — all high-risk patients (altered consciousness, distracting injury, suspected injury) need CT. MRI additionally required if neurological symptoms.
- NEVER remove a collar without formal clearance in an obtunded, intoxicated, or distracting-injury patient.
Pressure ulcer prevention is a non-negotiable component of spinal cord injury care:
- Turn every 2 hours using log-roll from day 1
- Appropriate mattress (low-air-loss or alternating pressure from day 1)
- Inspect pressure areas (occiput, heels, sacrum, greater trochanters) at every turn
- A single full-thickness sacral pressure ulcer in an SCI patient is a preventable catastrophe
SELF-CHECK
During a four-person log-roll of a suspected cervical spine injury patient, who has the highest-priority role and what is their specific responsibility?
A. The leg person, because leg rotation must be controlled to prevent spinal twisting
B. The person at the head, who maintains manual in-line cervical stabilisation and commands the roll
C. The pelvis person, because pelvic rotation drives spinal movement
D. Any team member can lead as they all perform equivalent functions
Reveal Answer
Answer: B. The person at the head, who maintains manual in-line cervical stabilisation and commands the roll
The person at the head commands the entire log-roll and maintains manual in-line stabilisation of the cervical spine throughout. This is the highest-skill, highest-priority role because the cervical spine is most vulnerable to uncontrolled movement, and the leader's count ("1-2-3 ROLL") synchronises all team members. An unsynchronised roll — even with four people — can produce relative motion between spinal segments. This role must be taken by the most experienced clinician present, not delegated to a junior.
Principles of Management: Definitive Treatment and Rehabilitation
Definitive management of spinal injuries is guided by three interconnected axes: fracture stability assessed through the three-column model and TLICS, neurological status graded using the ASIA scale, and the presence of specific indications for either emergency or elective surgical intervention. These axes must be considered simultaneously rather than sequentially, because the appropriate management pathway depends on all three: a mechanically stable fracture in a neurologically intact patient may be managed conservatively, while the same fracture morphology in a patient with an incomplete cord injury and a disrupted posterior ligamentous complex demands prompt surgical decompression and stabilisation. Across this spectrum — from simple analgesia and bracing to emergency decompression and multi-level fusion — the overarching goals remain consistent: prevent secondary neurological injury, restore spinal stability, enable early mobilisation and rehabilitation, and manage the systemic consequences of cord injury.
Medical management (all spinal cord injuries):
- Maintain mean arterial pressure ≥85-90 mmHg for 7 days post-injury to optimise cord perfusion (spinal cord perfusion pressure = MAP − cord pressure). Avoid systemic hypotension at all costs.
- Avoid hypoxia (SaO₂ >95%); early intubation for C3-C5 injuries with respiratory compromise.
- Urinary catheterisation (suprapubic or urethral as appropriate) — the areflexic bladder in spinal shock leads to overdistension injury.
- DVT prophylaxis — SCI patients have the highest DVT/PE risk of any surgical population; low molecular weight heparin within 72 hours once haemorrhage risk falls, combined with compression stockings and sequential compression devices.
- Bowel management programme from day 1 — digital stimulation, suppositories, scheduled evacuation.
- Temperature regulation (poikilothermia in high SCI due to loss of sympathetic vasomotor control).
Pharmacological neuroprotection:
High-dose methylprednisolone (NASCIS-II protocol: 30 mg/kg bolus then 5.4 mg/kg/h for 23 hours) was previously widely used but is now NOT recommended as standard of care — subsequent meta-analyses showed minimal neurological benefit against significant harms (increased pneumonia, sepsis, GI haemorrhage, pulmonary embolism). If used at all, it must be started within 8 hours and only with careful consideration. Most current guidelines (AANS/CNS 2013) recommend AGAINST routine use. Students must know this shift — the NASCIS-II protocol is no longer the standard it once appeared.
Conservative management:
Indicators: TLICS ≤4, neurologically intact, mechanically stable fractures. Methods include:
- Thoracolumbar brace (TLSO) — extension orthosis for compression fractures; maintains alignment during healing, allows mobilisation
- Cervical orthosis or halo vest — for specific cervical fractures (odontoid type II/III in elderly patients may be managed in halo)
- Physiotherapy and graded mobilisation within the brace
Surgical management:
Indications: TLICS >4, progressive neurological deterioration, irreducible deformity, mechanically unstable fracture, cauda equina syndrome (emergency). Principles:
- Decompression — removal of bone, disc, or haematoma compressing the cord or nerve roots; achieved via anterior (corpectomy) or posterior (laminectomy) approach depending on the source of compression
- Stabilisation and fusion — pedicle screw-rod instrumentation (posterior) or anterior cage/plate systems restore alignment and provide rigid fixation while the arthrodesis heals
- Timing: emergent (<24 hours) for cauda equina syndrome, incomplete SCI with progressing deficit, or irreducible cervical dislocation; urgent (within 24-72 hours) for other unstable injuries; delayed (3-5 days) for medically unstable polytrauma patients once resuscitated.
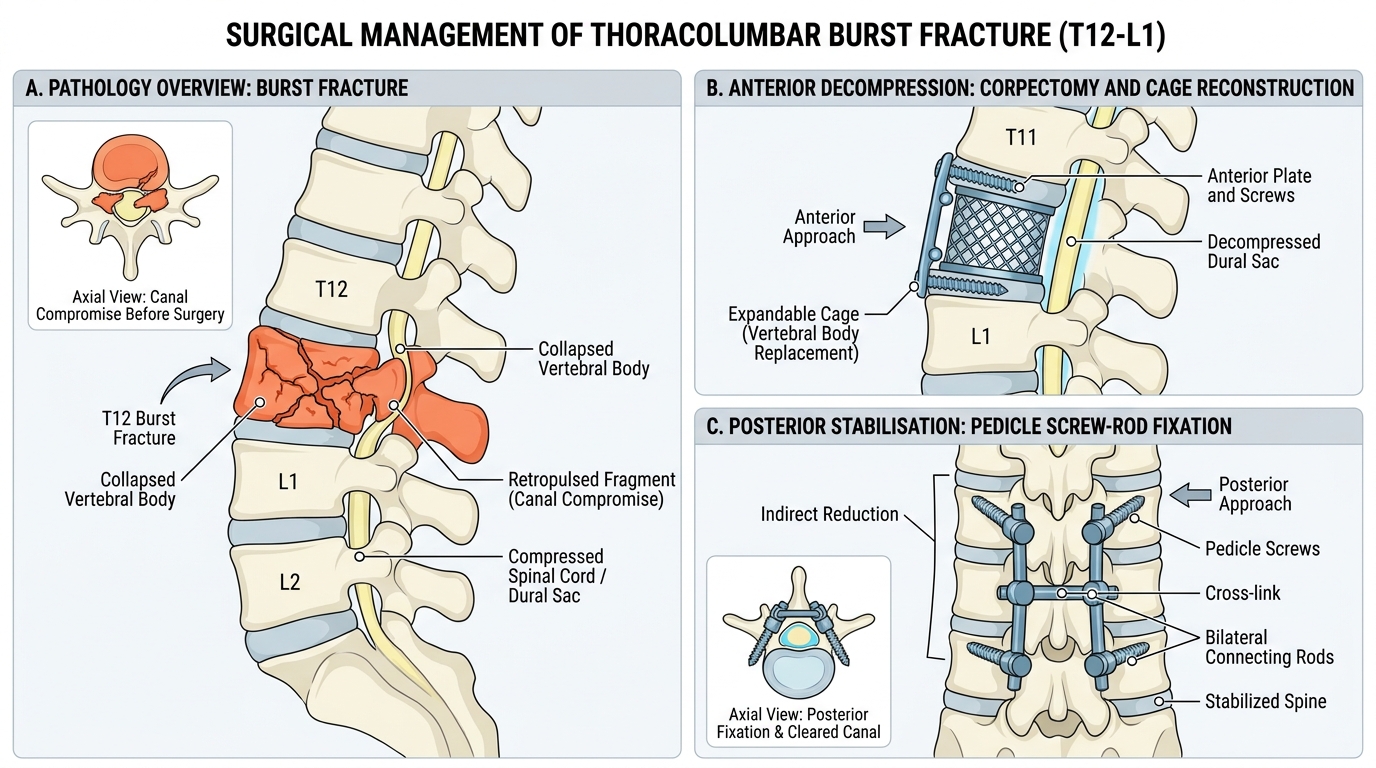
Thoracolumbar Burst Fracture: Anterior Decompression vs Posterior Stabilisation
Specific injuries:
- Jefferson fracture (C1 burst): from axial compression; typically treated conservatively in a halo vest unless transverse ligament is ruptured (rule of Spence — lateral mass overhang >6.9 mm total on open-mouth odontoid X-ray suggests ligament disruption).
- Odontoid fracture: Type I (tip, stable), Type II (base of dens, most common, high non-union risk in elderly — often requires surgery), Type III (body of C2, good healing with halo).
- Hangman's fracture (traumatic spondylolisthesis of C2): bilateral C2 pedicle fractures from hyperextension+distraction; paradoxically often neurologically intact (fracture decompresses the canal); Levine-Edwards classification guides management (Type I stable, Types II/IIA/III increasingly unstable).
Rehabilitation begins on day 1 and runs in parallel with medical and surgical care:
- SCI rehabilitation is a multidisciplinary endeavour (physiotherapist, occupational therapist, clinical psychologist, social worker, dietitian, urology)
- Functional goals by injury level: C1-C3 requires ventilatory support; C5-C6 can feed self with adaptive equipment; C7 can self-propel in manual wheelchair; T1-T6 good upper limb function, wheelchair independence; T11-L2 may achieve ambulatory function with orthoses
- Community reintegration, vocational rehabilitation, and sexual health counselling are integral
- Autonomic dysreflexia — a medical emergency in patients with SCI above T6; a noxious stimulus below the level of injury (distended bladder, faecal impaction, pressure sore) triggers massive sympathetic discharge (hypertension, bradycardia, headache, sweating); treat by eliminating the stimulus and positioning patient upright.
SELF-CHECK
A 65-year-old man falls backwards down stairs and presents with upper limb weakness greater than lower limb weakness, preserved perianal sensation, and bladder retention. His MRI shows cervical spondylosis with cord oedema at C5-C6. Which cord syndrome is this?
A. Brown-Séquard syndrome
B. Anterior cord syndrome
C. Central cord syndrome
D. Cauda equina syndrome
Reveal Answer
Answer: C. Central cord syndrome
Central cord syndrome is the most common incomplete SCI, classically occurring in elderly patients with pre-existing cervical spondylosis following a hyperextension injury — often without a fracture. The hallmarks are disproportionate upper limb > lower limb weakness (the centrally-located corticospinal tract fibres serving the arms lie more medially and are preferentially damaged), preserved sacral sensation (sacral sparing), and bladder dysfunction. Brown-Séquard produces an ipsilateral motor/proprioception deficit with contralateral pain/temperature loss. Anterior cord spares proprioception. Cauda equina is below the cord and produces LMN features, not this pattern.
Self-Assessment: Consolidating Spine Injury Principles
Having worked through the mechanisms, classification, examination, mobilisation technique, and management of spinal injuries, this self-assessment section consolidates the concepts most frequently tested in final MBBS examinations and most critical for safe clinical practice. Spinal injury management is an area where knowledge gaps carry immediate patient harm — the house officer who cannot recall the mean arterial pressure target after SCI, or who places the wrong person in command of a log-roll, directly endangers the patient. The examiner is particularly interested in whether you can integrate classification with management, recognise the incomplete cord syndromes from their neurological deficit patterns, and demonstrate that you understand the log-roll as a four-person coordinated procedure rather than an improvised group manoeuvre. Most importantly, you need to distinguish spinal shock from neurogenic shock — two concepts with identical-sounding names but entirely different mechanisms, clinical presentations, and treatments. The questions below cover every high-yield domain from this module. Answer each from memory before reviewing the reasoning; this is the only reliable way to identify genuine knowledge gaps rather than superficial recognition of prompted cues.
Verify that you can answer the following without hesitation:
- Can you grade a patient ASIA A vs ASIA D from an examination description, and state why sacral sparing is the pivotal test?
- Can you calculate a TLICS score from a fracture description and state the management recommendation?
- In a clinical vignette with disproportionate arm > leg weakness in an elderly patient after a fall, can you name the syndrome, the mechanism, and the prognosis?
- Can you describe the four-person log-roll from memory — who stands where, who commands, and what the team does on the count?
- Can you state the MAP target, the DVT prophylaxis timing, and the current recommendation on methylprednisolone for acute SCI?
- Can you distinguish neurogenic shock from haemorrhagic shock on clinical grounds and state the correct treatment for each?
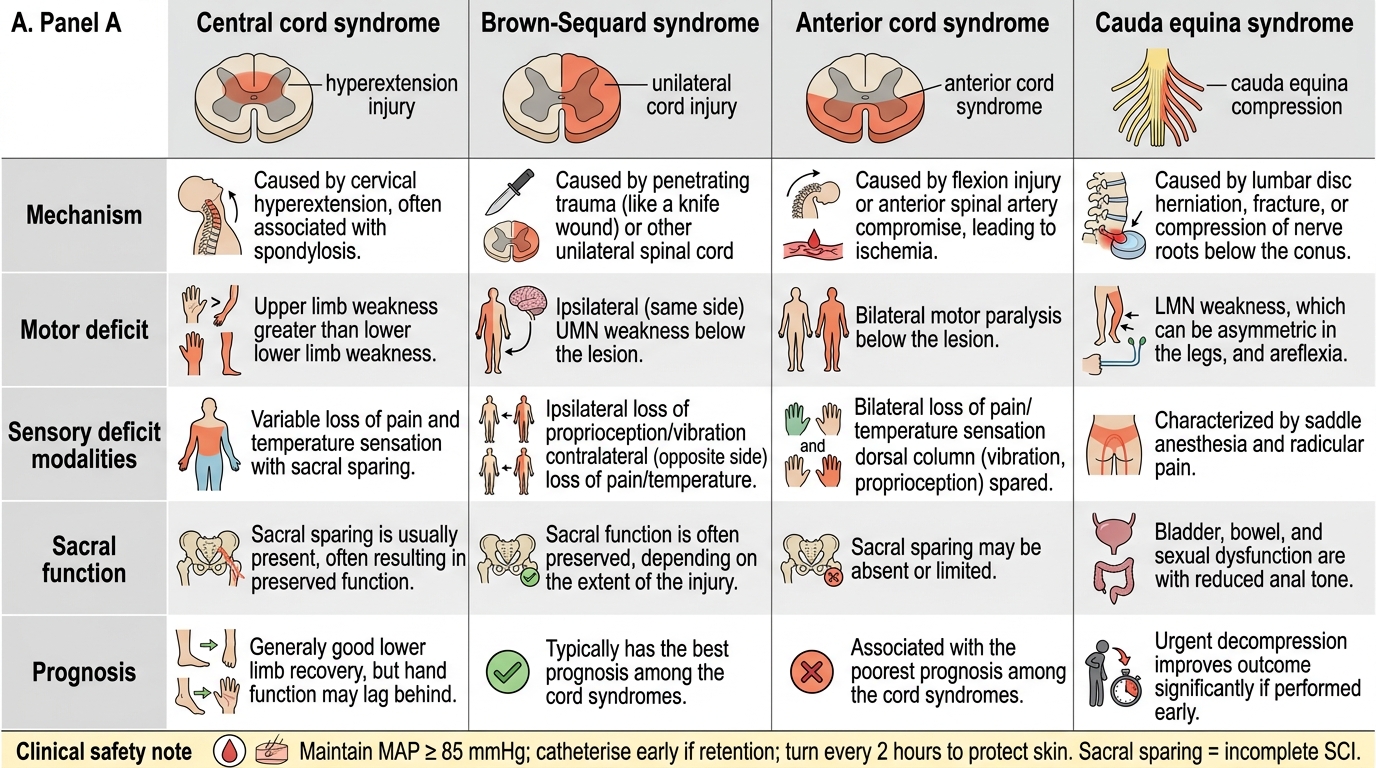
Incomplete Cord Syndromes Compared
If any question exposed a gap, return to the relevant section and re-read the specific mechanism or criterion before moving on. These are not optional details — they are the minimum safe-practice knowledge for a doctor managing a spinal-precautions patient.
CLINICAL PEARL
The three most important things to protect in spinal cord injury care: (1) Cord perfusion — maintain MAP ≥85 mmHg, never allow hypotension (a single episode of hypotension after SCI causes measurable cord ischaemia); (2) The bladder — a distended areflexic bladder in spinal shock causes overdistension injury to the detrusor; catheterise early; (3) The skin — a full-thickness pressure ulcer in an insensate SCI patient requires months to heal and risks sepsis; turn every 2 hours from day 1. Remember: sacral sparing (ANY preserved function at S4-S5 — perianal sensation, voluntary anal contraction) classifies the injury as INCOMPLETE, not complete — this dramatically changes the prognosis and urgency of surgical decompression.