Page 1 of 18
OR2.14 | Fracture Complication Investigation — SDL Guide
Learning Objectives
- Define malunion and non-union and distinguish hypertrophic from atrophic non-union on radiological and clinical grounds
- Describe the pathological basis and clinical presentation of post-fracture infection including infected non-union
- Select and interpret the appropriate investigations — radiological, biochemical, microbiological — for each complication type
- Outline the principles of management for malunion, each sub-type of non-union, and infected non-union
- Recognise the clinical and imaging red flags that demand urgent reassessment after fracture treatment
INSTRUCTIONS
Fractures are expected to heal. When they do not — or when they heal in the wrong position — patients lose function, face further surgery, and risk limb loss. As a final-year student you will encounter these complications in outpatient clinics and ward rounds. This module equips you to recognise the clinical and radiological patterns of malunion, non-union (hypertrophic and atrophic), and infected non-union, and to plan a systematic investigation workup that directly drives management decisions.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch. 7 — Complications of Fractures (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch. 23 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 35-year-old construction worker presents eight months after a closed tibial shaft fracture treated with a below-knee plaster cast. He still has pain, localised tenderness, and cannot bear weight. His general practitioner's X-ray shows 'no significant new callus' and an obvious angulation deformity. He is worried he will never walk properly again. What has gone wrong, and how do you investigate it?
WHY THIS MATTERS
Complications of fracture healing — malunion, delayed union, non-union, and infection — are among the most common reasons for prolonged disability after injury. In a resource-limited setting where implant failure and under-treatment are real, final-year students must be able to: (1) identify which complication is present from the history and plain radiograph; (2) select confirmatory investigations that are both cost-effective and clinically actionable; and (3) distinguish infected from non-infected non-union because the two have entirely different management pathways. Missing an infected non-union and proceeding to bone grafting without source control is a surgical disaster.
RECALL
Recall from your fracture-healing studies: normal bone repair passes through haematoma, soft callus (fibrocartilage, 2–3 weeks), hard callus (woven bone, 6–8 weeks), and remodelling phases. The periosteum is the primary source of callus in subperiosteal injuries; the medullary canal and endosteum contribute to intramedullary fractures. Adequate immobilisation, biological vascularity, and mechanical stability are the three biological prerequisites of union. When any of these is disrupted, healing stalls or proceeds in the wrong alignment.
Malunion — Pathological Basis and Clinical Features
Malunion is defined as healing of a fracture in a position that is unacceptable in terms of angulation, rotation, or shortening, and that either causes current functional impairment or will predictably cause degeneration over time. The threshold for 'unacceptable' alignment depends on the bone and the patient's functional demands: the femur tolerates up to 5° of varus/valgus and 1–1.5 cm of shortening before altered biomechanics become clinically significant, whereas even 5–10° of rotational malunion of the tibia causes gait abnormality and knee/ankle joint stress. The clinical presentation of malunion depends on its site. A patient with a Colles fracture malunited in excessive dorsal angulation will show the classic dinner-fork deformity on lateral view, with restricted wrist extension and weakness of grip. Femoral shaft malunion in internal rotation causes a 'toeing-in' gait. Tibial malunion in varus transfers load to the medial knee compartment, accelerating medial-compartment osteoarthritis. Shortening malunion causes a limb-length discrepancy that throws off the pelvis and lumbar spine. In children, compensatory overgrowth may partially remodel malunion of the femoral shaft, but rotational deformity in any age group does not remodel significantly.
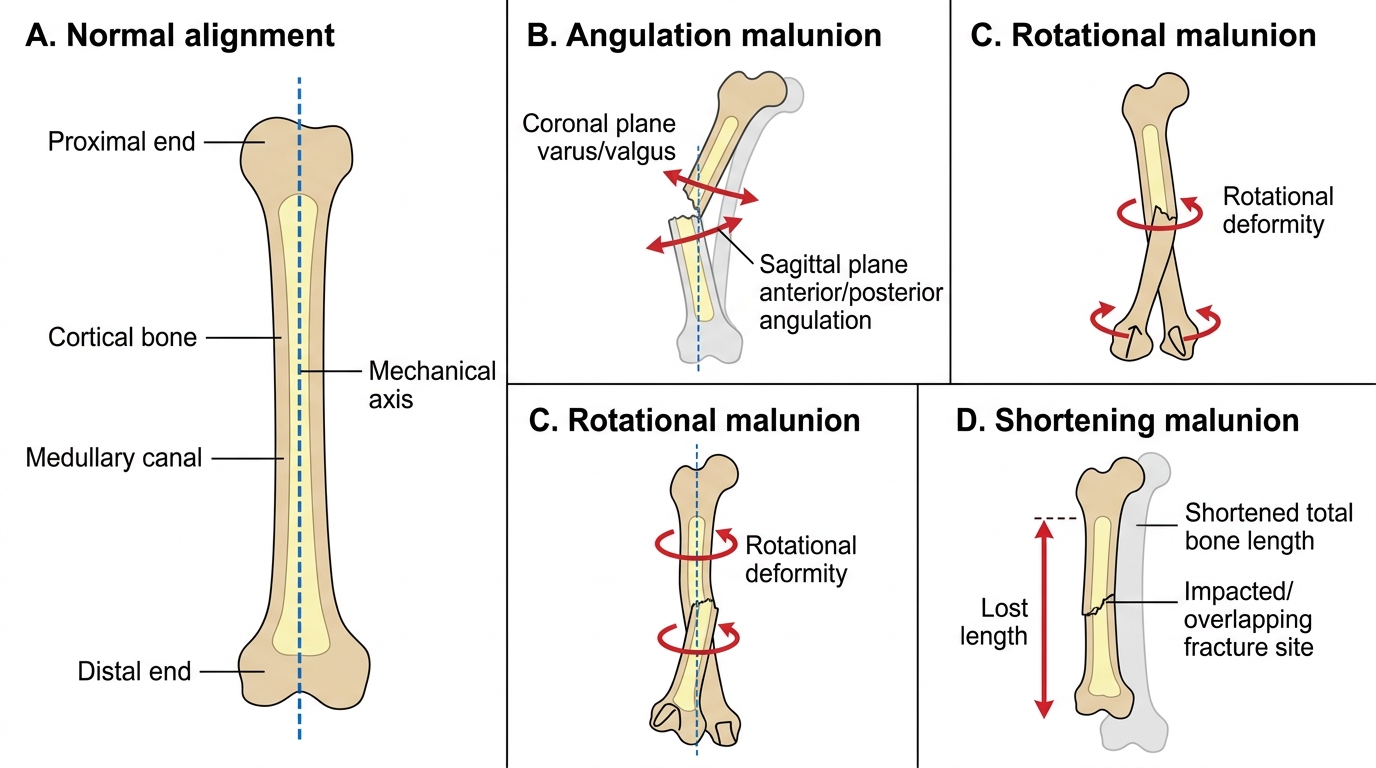
Three Planes of Long-Bone Malunion
The clinical examination for suspected malunion should include: measurement of limb lengths (true and apparent) with the limb in a standardised position; goniometric measurement of joint range of motion; assessment of lower limb alignment in the standing position (genu varum/valgum, tibial torsion); and rotational profiling of the femur and tibia by comparing hip and ankle rotation angles. Neurovascular examination should also be repeated even in the chronic setting, since late nerve stretching around a malunited supracondylar fracture can produce a tardy ulnar or median nerve palsy years after the original injury.
Non-union — Definition, Classification and Pathological Basis
Non-union is defined as a fracture that has failed to heal within a time period beyond which union is expected for that particular bone and fracture pattern — conventionally taken as six months for most long bones, though some authorities use 'delayed union' (3–6 months) as an intermediate category. Non-union implies that the natural healing process has ceased and will not resume without intervention. The US FDA definition, widely cited in research, requires at least 9 months from injury with no radiological progress for 3 consecutive months. The aetiology of non-union is captured by the mnemonic DAMNED — Damage (severe soft-tissue stripping, periosteal loss), Avascular necrosis (loss of vascularity to one or both fragments), Mobility (inadequate immobilisation, implant failure), Nerve injury (associated neurological damage reducing trophic stimulus), Excessive gap (bone loss, distraction, interposition of soft tissue), and Drugs/disease (steroids, NSAIDs, smoking, diabetes, poor nutrition, bone disease). The Weber–Cech classification divides non-unions into two mechanistic groups that have fundamentally different management implications.
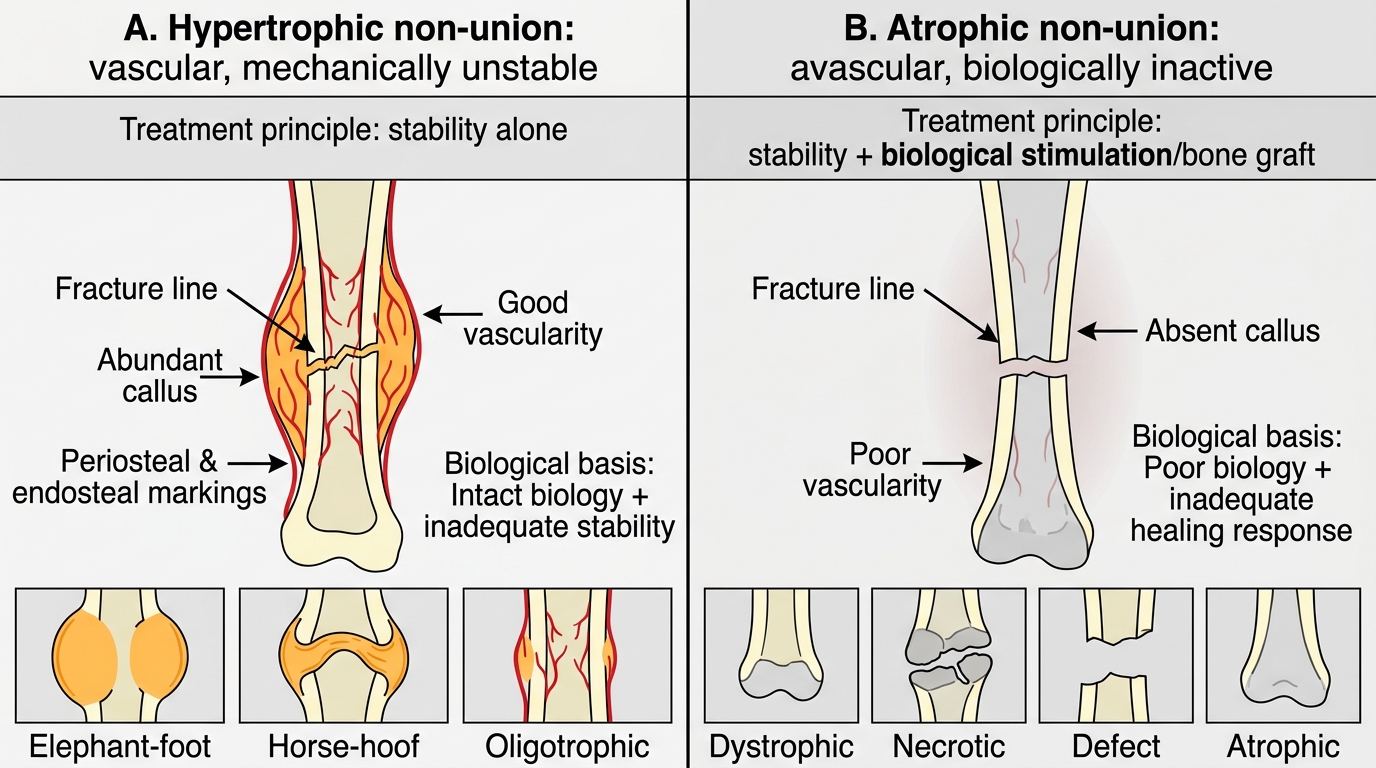
Weber-Cech Classification of Non-union
Hypertrophic non-union (also called vascular or biologically active non-union) results from mechanical instability in the presence of adequate blood supply. The biology is intact — the periosteum and endosteum are producing callus — but because the fracture site is still mobile, the callus cannot mature from fibrocartilage to woven bone. On radiograph, the classic 'elephant-foot' appearance shows abundant callus ballooning around the fracture ends. The horse-hoof and oligotrophic sub-types show progressively less callus but all have active vascularity. These non-unions respond to stability alone — rigid fixation (usually intramedullary nailing or plating) provides the mechanical environment the biology is waiting for, and union follows without bone graft. Atrophic non-union results from inadequate biological activity — either a devascularised bone end (from periosteal stripping or segmental loss), excessive soft-tissue damage, or systemic factors impairing healing. The fracture ends are osteoporotic, pointed ('pencilled'), and show no callus. These require both biological stimulation (bone grafting, bone morphogenetic protein) and mechanical stabilisation. The most severe form, the infected non-union, combines all these problems with superimposed sepsis.
Infected Non-union — Pathophysiology and Clinical Presentation
Infected non-union represents the convergence of biological failure (as in atrophic non-union) and chronic osteomyelitis in the same segment of bone. It is one of the most challenging problems in orthopaedic surgery and carries a high risk of amputation if mismanaged. The infection is almost always the result of open fracture, implant infection, or post-surgical wound breakdown — Staphylococcus aureus (including MRSA) is the most common pathogen, followed by Gram-negative rods (Pseudomonas aeruginosa, Klebsiella) in post-traumatic or nosocomial cases. Biofilm formation on devitalised bone (sequestrum) and metalwork makes medical treatment alone ineffective; the biofilm protects organisms from both host immunity and antibiotic penetration, which is why infected non-union cannot be cured without surgical debridement and sequestra removal. The clinical hallmarks of infected non-union are: a persistent draining sinus overlying the fracture site; cyclical flares of local redness, warmth, and discharge; pain out of proportion to the radiological appearance; and wound breakdown over previously healed surgical scars. Systemic features (fever, raised inflammatory markers) may be surprisingly absent in chronic low-grade infection, where the body has partially walled off the septic focus. This is why infection must be actively excluded by investigation before any bone-grafting procedure — to graft into infected bone is to guarantee failure of the graft and propagation of the sepsis.
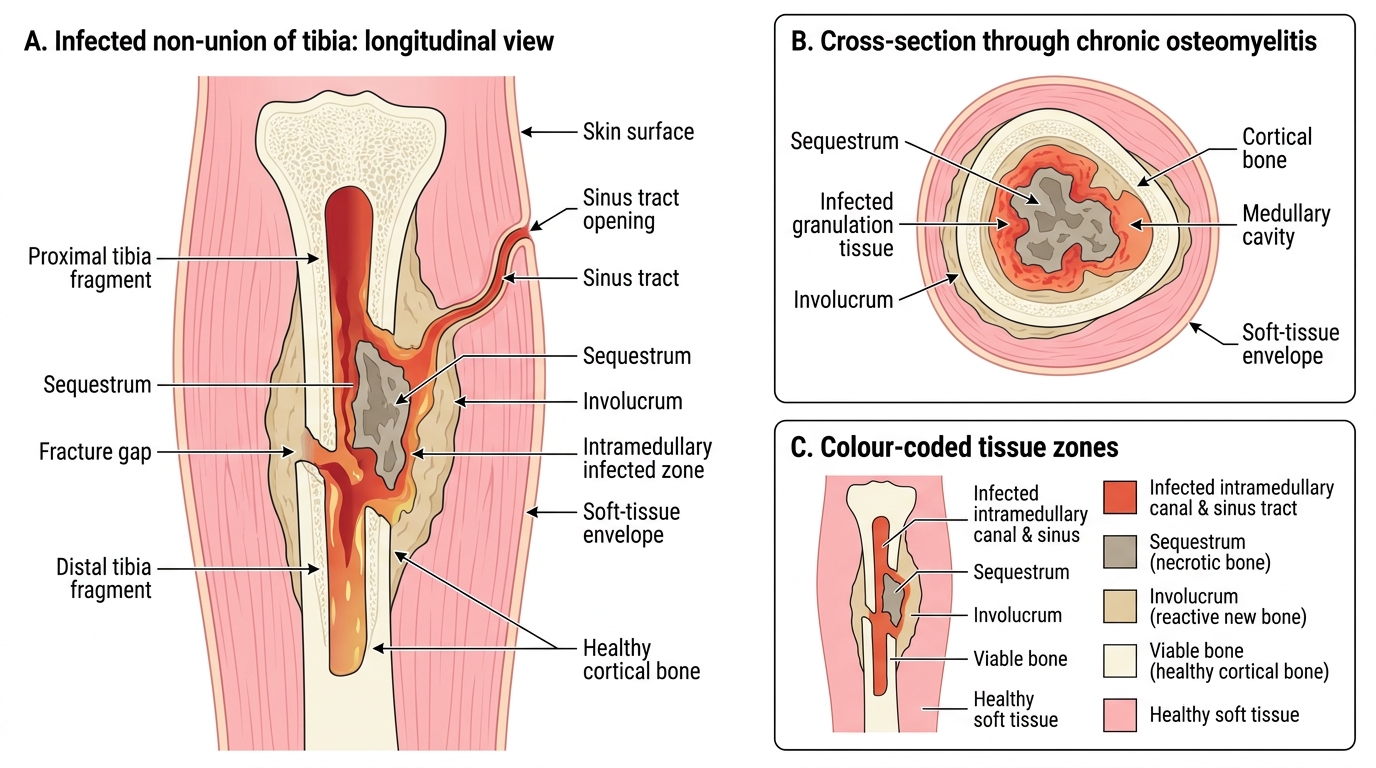
Infected Non-union of the Tibia