Page 2 of 18
OR2.14 | Fracture Complication Investigation — SDL Guide (Part 2)
Radiological Investigation of Malunion
The radiological workup for malunion begins with standard anteroposterior (AP) and true lateral radiographs of the affected bone taken on long-leg cassettes that include the joints above and below. Long-leg standing films are mandatory when assessing lower-limb alignment, because supine films underestimate functional angulation. The key measurements on radiographs are: the angular deformity in both planes (degrees of varus/valgus and flexion/extension); the amount of shortening (measured as overlap or step-off); and the rotational appearance, which on plain film is assessed by comparing the cross-sectional appearance of the bone at the fracture site with its proximal and distal ends. Plain radiography cannot quantify true rotational malunion accurately — for this, a CT scanogram is required. CT with three-dimensional reconstruction defines: (1) the exact degree of angulation and rotation; (2) the extent of callus formation and cortical continuity; and (3) the presence of bony spurs or hardware. In lower limb, a standing AP of both lower limbs on a single cassette allows measurement of the mechanical axis deviation and the contribution of the malunion to overall alignment. Bone scintigraphy is generally not required for uncomplicated malunion but becomes relevant when there is concern about the viability of the malunited segment.
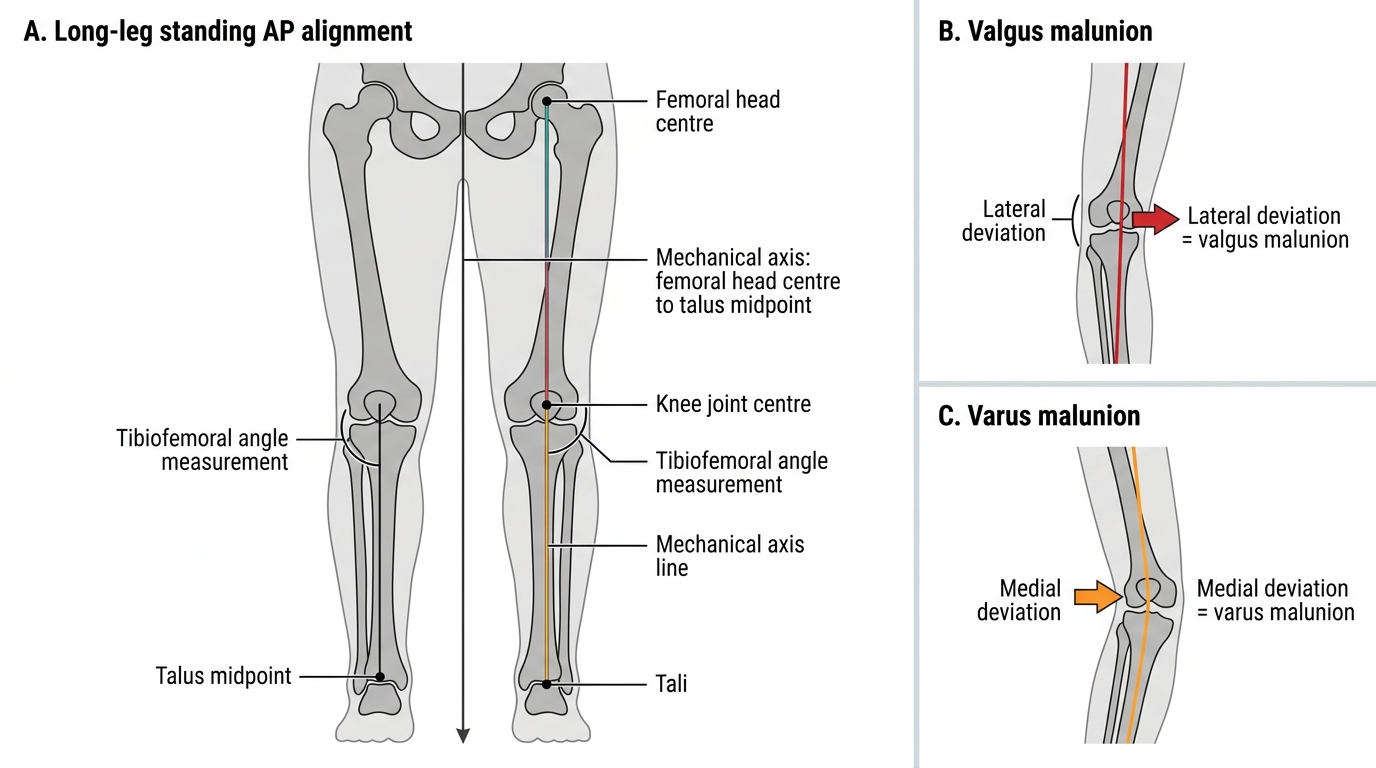
Mechanical Axis and Malunion Alignment
Investigation of Non-union — Radiological
The radiological investigation of non-union forms the backbone of clinical assessment and should be systematic and complete. The standard starting point is serial plain radiographs — AP and lateral projections — taken at the initial evaluation and then at scheduled intervals, because the criterion for non-union requires radiological evidence of no progression over at least 3 months (some protocols use 3 consecutive sets at 6-week intervals). The plain-film features that define the non-union type are central to planning treatment: abundant callus with visible fracture line = hypertrophic; absent callus with rounded, sclerotic, or tapered bone ends = atrophic; moth-eaten cortex, periosteal reaction, and involucrum formation = infected. CT scanning is now the gold standard for detailed non-union assessment because it provides cross-sectional views that overcome the overlap seen on plain films. CT quantifies: (1) the degree of callus and cortical bridging (a standard union criterion is ≥3 cortices bridged on AP and lateral); (2) the bone gap if any; (3) the presence of sequestra (dense cortical fragments within the medullary cavity, classically not showing uptake on bone scan); and (4) the position and integrity of internal fixation hardware. MRI is the most sensitive imaging modality for early bone infection and bone marrow oedema — it shows medullary signal change before plain radiographs reflect it. MRI findings in infected non-union include: low T1, high T2/STIR signal in the marrow; cortical destruction; sinus tract; and an enhancing abscess cavity on gadolinium-enhanced sequences. MRI is mandatory when clinical suspicion of infection exists even with equivocal plain films.
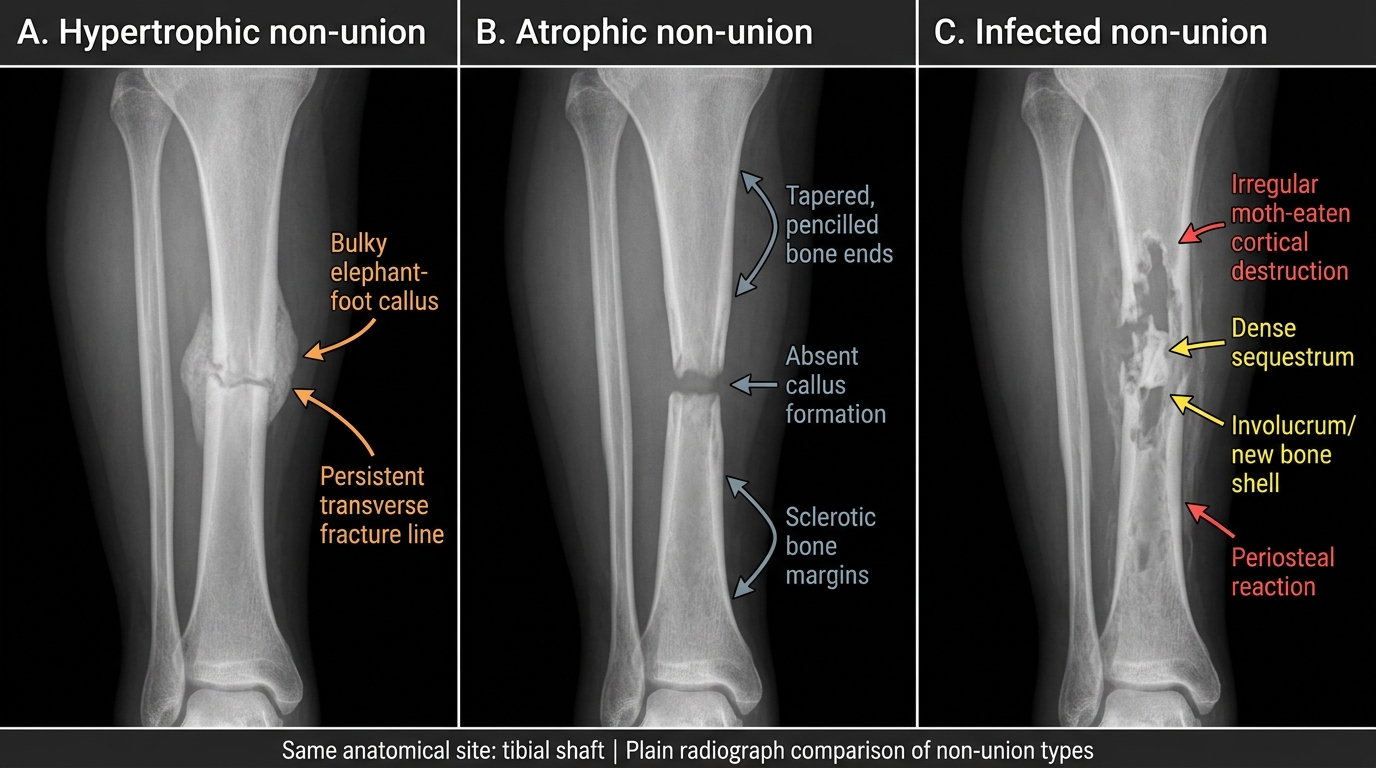
Plain Radiographic Types of Tibial Shaft Non-union
Investigation of Non-union — Biochemical and Microbiological
Biochemical and microbiological investigations are essential when infection is suspected and are also useful in identifying systemic conditions that impair fracture healing. The baseline inflammatory markers for suspected infected non-union are: white blood cell count (WBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). ESR has high sensitivity (approximately 75–90%) but poor specificity for chronic bone infection; CRP normalises more rapidly with treatment and is the preferred marker for monitoring response to therapy. Procalcitonin is more specific for bacterial infection than CRP and is gaining use, though it may be normal in chronic low-grade osteomyelitis. Microbiological cultures are the cornerstone of management planning for infected non-union. Superficial swabs of sinus tracts are notoriously unreliable because they reflect sinus colonisation rather than deep bone infection — they are correctly positive in only 40–50% of cases and may mislead antibiotic selection. The standard of care requires intraoperative deep bone biopsy and peri-implant tissue sampling: at least 5 specimens from separate sites in the infected zone, sent in separate labelled containers for aerobic and anaerobic culture, prolonged incubation (14 days for slow-growing organisms), and fungal culture if the patient is immunocompromised. Histopathology of the same biopsy specimen confirms infection (>5 polymorphonuclear leucocytes per high-power field in multiple tissue samples is a validated threshold) and excludes malignancy in suspicious lesions. Where culture results are pending, empirical antibiotic coverage should target S. aureus and common Gram-negatives, with MRSA cover added if the patient has had prior hospital admission, indwelling hardware for >30 days, or a history of MRSA colonisation.
| Investigation | Best Use | Limitation |
|---|---|---|
| ESR | Sensitive screen for chronic infection | Non-specific; raised in many conditions |
| CRP | Monitor response to treatment | May be normal in chronic low-grade infection |
| WBC | Acute flare detection | Insensitive for chronic osteomyelitis |
| Sinus-tract swab | Rapid result | 40–50% concordance with deep tissue cultures — not reliable for antibiotic selection |
| Intraoperative bone biopsy (×5) | Definitive microbiological diagnosis | Requires operative access |
| MRI | Early bone infection, medullary extent, soft-tissue involvement | Artefact from metalwork; costly |
| Bone scintigraphy (Tc-99m) | Sensitive for increased bone turnover | Low specificity; sequestra are 'cold' |
| Labelled leucocyte scan (WBC scan) | Specific for active infection | Less available; lower sensitivity in chronic vs acute |
SELF-CHECK
A plain radiograph of a tibial non-union at 10 months post-injury shows abundant callus at both fracture ends with a clear fracture line still visible but no bridging. Which type of non-union is this, and what is the primary treatment principle?
A. Atrophic non-union — requires bone grafting plus stabilisation
B. Hypertrophic non-union — requires rigid mechanical stabilisation; biological stimulus is already present
C. Infected non-union — requires source control before any fixation
D. Oligotrophic non-union — requires vascular anastomosis of the bone ends
Reveal Answer
Answer: B. Hypertrophic non-union — requires rigid mechanical stabilisation; biological stimulus is already present
Abundant callus with a persisting fracture line is the radiological hallmark of hypertrophic (vascular/biologically active) non-union. The biology is working — the problem is insufficient mechanical stability, which prevents the callus from maturing. Treatment is rigid stabilisation (typically intramedullary nail or compression plating) without biological augmentation. Bone graft is not needed because vascularity is intact. Atrophic non-union would show absent callus and sclerotic bone ends.