Page 10 of 22
OR2.5-6 | Forearm Fracture Patterns — SDL Guide
Learning Objectives
- Describe the mechanisms and displacement forces in fractures of both bones of the forearm
- Distinguish Monteggia from Galeazzi injury by anatomy, mechanism, and the associated joint dislocation
- Classify distal radius fractures (Colles, Smith, Barton) and apply the AO classification
- Outline management principles: conservative vs operative, and timing for each pattern
- Identify the neurovascular and compartment syndrome complications of forearm fractures
INSTRUCTIONS
The forearm functions as a two-bone unit -- radius and ulna must be considered together, not separately. The classic eponymous fracture-dislocations (Monteggia: proximal ulna + radial head dislocation; Galeazzi: distal radius + DRUJ disruption) illustrate this principle: fixing only the visible fracture without addressing the hidden dislocation leads to permanent disability. Distal radius fractures are among the most common injuries in clinical practice. This module covers OR2.5 (both-bones forearm, Galeazzi, Monteggia) and OR2.6 (distal radius fractures) in an integrated module because the forearm's biomechanical unity makes them inseparable.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch 22 -- Fractures of the Forearm (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 31 -- Injuries of the Forearm (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old man falls from a bicycle and sustains a displaced fracture of the proximal ulna. The orthopaedic registrar applies a cast and discharges the patient. Two days later the patient returns with persistent elbow pain and an X-ray reveals the radial head is dislocated anteriorly. The registrar treated the ulna fracture but missed the joint dislocation. What is this injury called, why is fixing the fracture alone insufficient, and how should it be managed?
WHY THIS MATTERS
Forearm fractures are among the most functionally demanding injuries because the radius and ulna form a kinematic pair: rotation of the forearm (pronation and supination) depends on the precise geometry of both bones and their connecting interosseous membrane. A fracture of one bone that alters its length or angulation necessarily affects the other bone or its proximal or distal joint. Recognising fracture-dislocation patterns -- where a bony fracture is accompanied by a joint dislocation -- is the single most important clinical skill in forearm trauma, as the dislocation is easily missed on radiographs obtained without the correct joints visible. Missing a Monteggia dislocation or a Galeazzi DRUJ disruption converts a fixable injury into a permanent deformity.
RECALL
From your anatomy, recall that the radius and ulna are connected proximally at the proximal radioulnar joint (PRUJ, within the elbow), distally at the distal radioulnar joint (DRUJ, at the wrist), and across their lengths by the interosseous membrane. Pronation and supination rotate the radius around the fixed ulna through approximately 170 degrees of arc. The annular ligament holds the radial head within the radial notch of the ulna at the PRUJ. The triangular fibrocartilage complex (TFCC) stabilises the DRUJ and allows axial load transmission from the carpus through the ulna. Disruption of either joint while the opposite end is fractured is the definition of a Monteggia (proximal) or Galeazzi (distal) injury.
Fractures of Both Bones of the Forearm
Fractures of both bones of the forearm (radius and ulna at the same level, usually middle or distal third) are a common injury in adults following falls, direct impact, or road traffic accidents. The mechanism is typically a fall on the outstretched hand with axial loading and a rotational component, or a direct blow to the forearm. In children, the forearm is the most common fracture site; greenstick and plastic deformity patterns predominate in young children, while complete fractures with displacement occur in older children and adolescents. The combined injury of both bones is often more functionally disabling than fractures of either bone alone because forearm rotation depends on the precise length and alignment of both the radius and the ulna working in concert.
Displacement in both-bones forearm fractures is driven by the pronator muscles (pronator teres and pronator quadratus) and the supinator; the level of fracture relative to pronator teres insertion determines the rotational deformity:
- Fracture above the insertion of pronator teres (proximal third): biceps supinates the proximal fragment; pronator teres pronates the distal fragment
- Fracture below pronator teres insertion (middle/distal third): pronator quadratus pronates the distal fragment; biceps and supinator create a variable proximal fragment position
In adults, both-bones forearm fractures are almost always managed operatively because even small angular or rotational malunion significantly restricts forearm rotation, which is critically important for hand function. The gold standard is plate-and-screw fixation of both bones (3.5 mm dynamic compression plate) via separate anterolateral (Henry) approach for the radius and dorsal (Thompson) or direct lateral approach for the ulna. Open fractures of the forearm follow the Gustilo-Anderson classification and require antibiotics within 1 hour, debridement, and fixation.
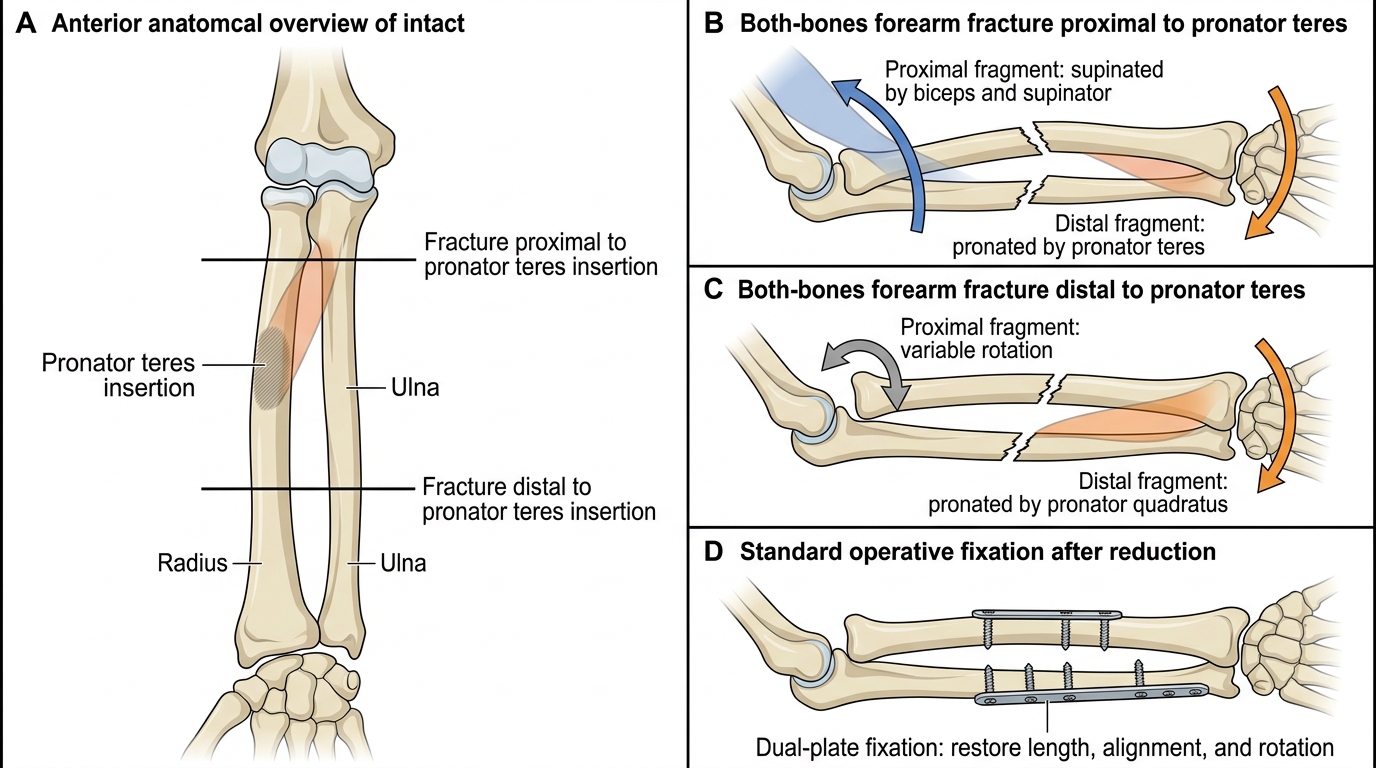
Both-Bones Forearm Fracture: Rotation and Dual-Plate Fixation
| Fracture level | Proximal fragment rotation | Distal fragment rotation |
|---|---|---|
| Proximal to pronator teres | Supinated (biceps, supinator) | Pronated (pronator teres) |
| Distal to pronator teres | Variable | Pronated (pronator quadratus) |
Monteggia Fracture-Dislocation
The Monteggia fracture-dislocation is defined as a fracture of the proximal ulna associated with dislocation of the radial head (at the PRUJ -- the proximal radioulnar joint within the elbow). It is named after Giovanni Battista Monteggia, who described it in 1814. The critical anatomical point: when the proximal ulna fractures, it shortens, and this shortening drives the radial head out of the annular ligament and the PRUJ. The fracture is in the ulna; the dislocation is in the elbow (radial head). This pattern is one of the most commonly missed injuries in emergency orthopaedics because the dislocation is not at the fracture site -- the clinician fixes their attention on the visible ulna fracture and fails to include the elbow joint in the radiograph series, overlooking the dislocated radial head entirely. The Bado classification (1967) categorises Monteggia injuries into four types based on the direction of radial head dislocation and the ulnar fracture pattern:
- Bado type I (most common, ~60%): anterior radial head dislocation + anterior ulnar fracture angulation
- Bado type II: posterior radial head dislocation + posterior ulnar fracture (apex posterior)
- Bado type III: lateral radial head dislocation (in children, produces a lateral Monteggia)
- Bado type IV: anterior radial head dislocation + fractures of both the radius and ulna
The key clinical rule: whenever an isolated ulnar shaft fracture is seen on radiograph, the elbow joint must be imaged -- the radial head dislocation is the missed injury. An undisplaced or minimally displaced isolated ulnar fracture ('nightstick fracture') in adults can be managed non-operatively, but any angulation of the ulna fracture must be assessed for concomitant radial head dislocation. In children, closed reduction under anaesthesia (reducing the radial head after fixing the ulna) is usually sufficient. In adults, Monteggia injuries require ORIF of the ulna (which reduces the radial head); if the radial head does not reduce after ulnar fixation, open reduction of the PRUJ is required, with annular ligament repair or reconstruction.
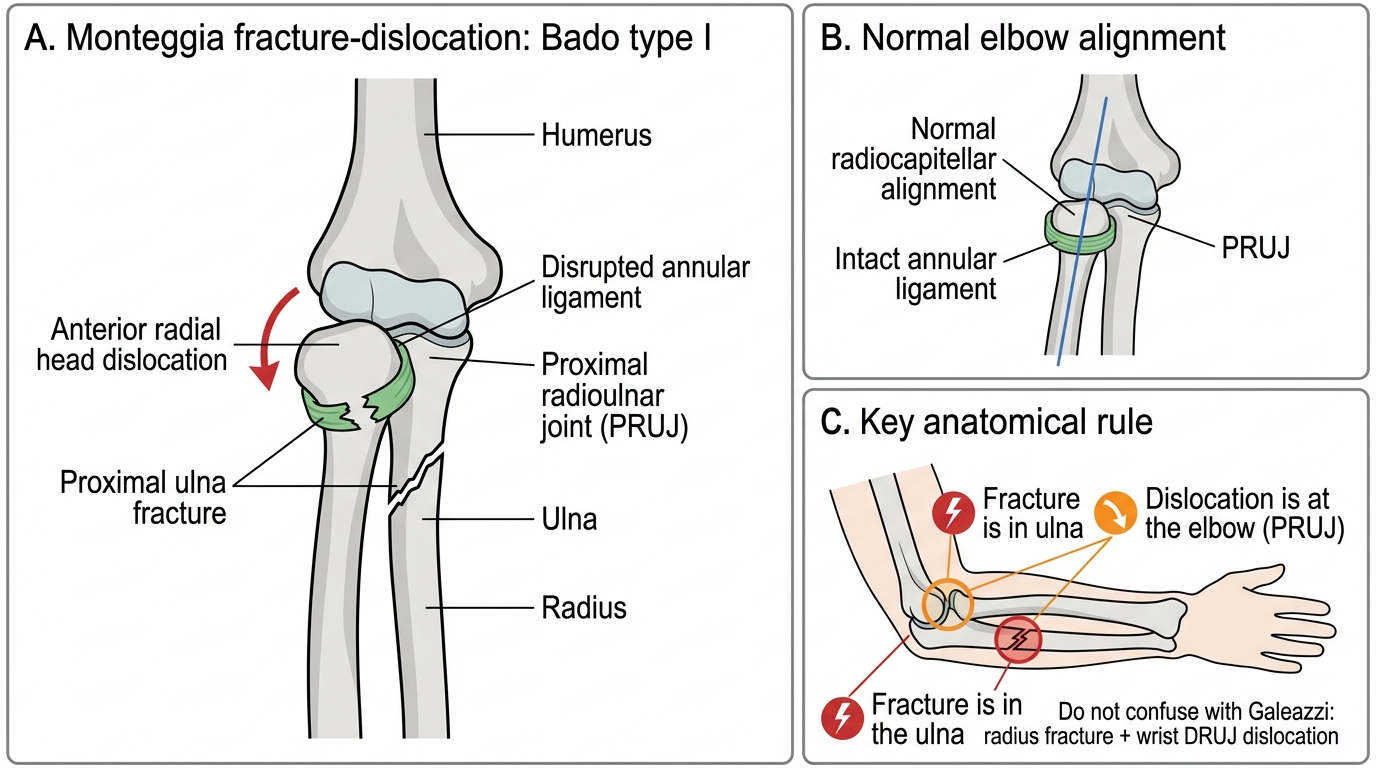
Monteggia Fracture-Dislocation: Bado Type I
Galeazzi Fracture-Dislocation
The Galeazzi fracture-dislocation is defined as a fracture of the distal third of the radius associated with disruption of the distal radioulnar joint (DRUJ). It is named after Riccardo Galeazzi, who described it in 1934. The critical anatomical point: a fracture of the distal radius shortens the bone, and the DRUJ stabilisers (TFCC) are either disrupted or the ulnar head dislocates (usually dorsally). The fracture is in the radius; the dislocation is at the wrist (DRUJ). This is sometimes called a 'fracture of necessity' because the nature of the injury makes it impossible to maintain non-operatively: closed reduction of a Galeazzi fracture inevitably redisplaces the DRUJ.
The DRUJ disruption can be confirmed clinically by a painful, prominent ulnar head at the wrist, and radiographically by ulnar head dorsal or volar subluxation on a lateral wrist view. The rule for Galeazzi: whenever a distal radius fracture is seen, image the wrist and check the DRUJ alignment. The management principle in adults is ORIF of the radius fracture (3.5 mm plate), which -- if anatomical -- usually reduces the DRUJ; if DRUJ remains unstable after radius fixation, it is stabilised by Kirschner wire in supination or TFCC repair. Galeazzi fractures cannot be managed non-operatively in adults.
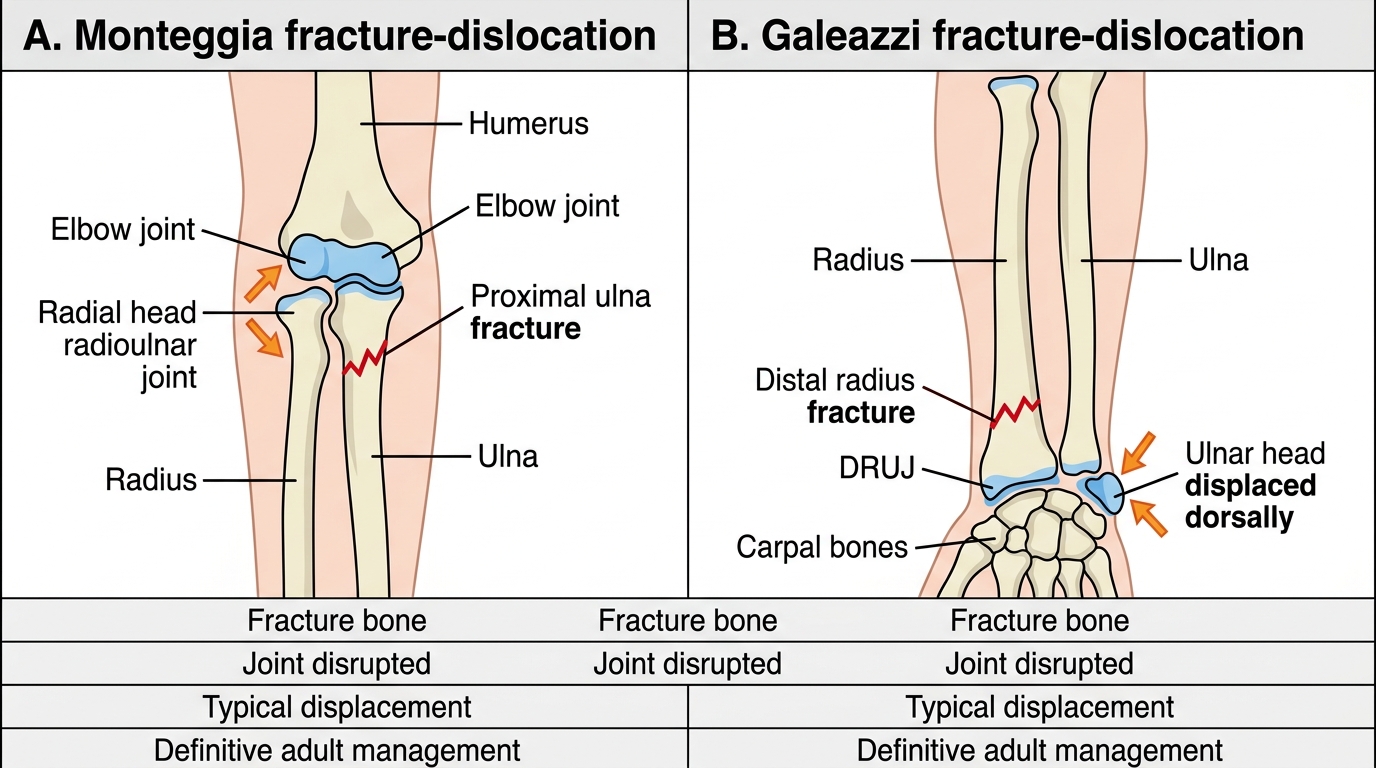
Monteggia Versus Galeazzi Fracture-Dislocations
| Feature | Monteggia | Galeazzi |
|---|---|---|
| Fracture bone | Proximal ulna | Distal radius |
| Joint disrupted | PRUJ (radial head, elbow) | DRUJ (wrist) |
| Direction | Radial head anteriorly (Bado I) | Ulnar head dorsally |
| Management | ORIF ulna; reduce radial head | ORIF radius; stabilise DRUJ |
| Non-op possible? | No (adults) | No (adults) |
SELF-CHECK
A radiograph shows a spiral fracture of the distal third of the radius with apparent shortening and the ulnar head displaced dorsally at the wrist. What is this injury and what is the definitive treatment?
A. Monteggia fracture -- ORIF of the proximal ulna reduces the radial head dislocation
B. Galeazzi fracture-dislocation -- ORIF of the distal radius restores DRUJ alignment; DRUJ stabilised if unstable
C. Colles fracture -- closed reduction and plaster in the 'position of immobilisation'
D. Both-bones forearm fracture -- dual plate fixation required
Reveal Answer
Answer: B. Galeazzi fracture-dislocation -- ORIF of the distal radius restores DRUJ alignment; DRUJ stabilised if unstable
Galeazzi = distal radius fracture + DRUJ disruption at the wrist. The ulnar head displaces dorsally because the TFCC stabilisers are disrupted. Management is ORIF of the radius fracture (which usually reduces the DRUJ); if the DRUJ remains unstable, it is held in supination with a K-wire or the TFCC is repaired. Non-operative management is inadequate in adults. Monteggia involves the proximal ulna with elbow (PRUJ) dislocation -- the opposite end.