Page 11 of 22
OR2.5-6 | Forearm Fracture Patterns — SDL Guide (Part 2)
Distal Radius Fractures
Distal radius fractures are the most common fracture in adults under 65 and in elderly women with osteoporosis, collectively representing one of the most frequently encountered fractures in any emergency department. They are caused by a fall on an outstretched hand (FOOSH) with dorsiflexion and slight supination of the wrist. The classic descriptive eponyms define the displacement pattern and the corresponding mechanism of injury; understanding each eponym precisely allows a bedside diagnosis from the clinical deformity alone, before the radiograph is available. Each pattern also has a distinct reduction manoeuvre and a preferred operative approach if non-operative management is inadequate, making the eponyms clinically indispensable rather than historical curiosities. In clinical practice it is essential to understand the three classical eponyms -- Colles, Smith, and Barton -- because each describes a distinct displacement vector, a characteristic clinical deformity, and a different management approach, and each can be identified at the bedside before a radiograph is obtained. A sound grasp of these three fracture types is fundamental to competent emergency orthopaedic care.
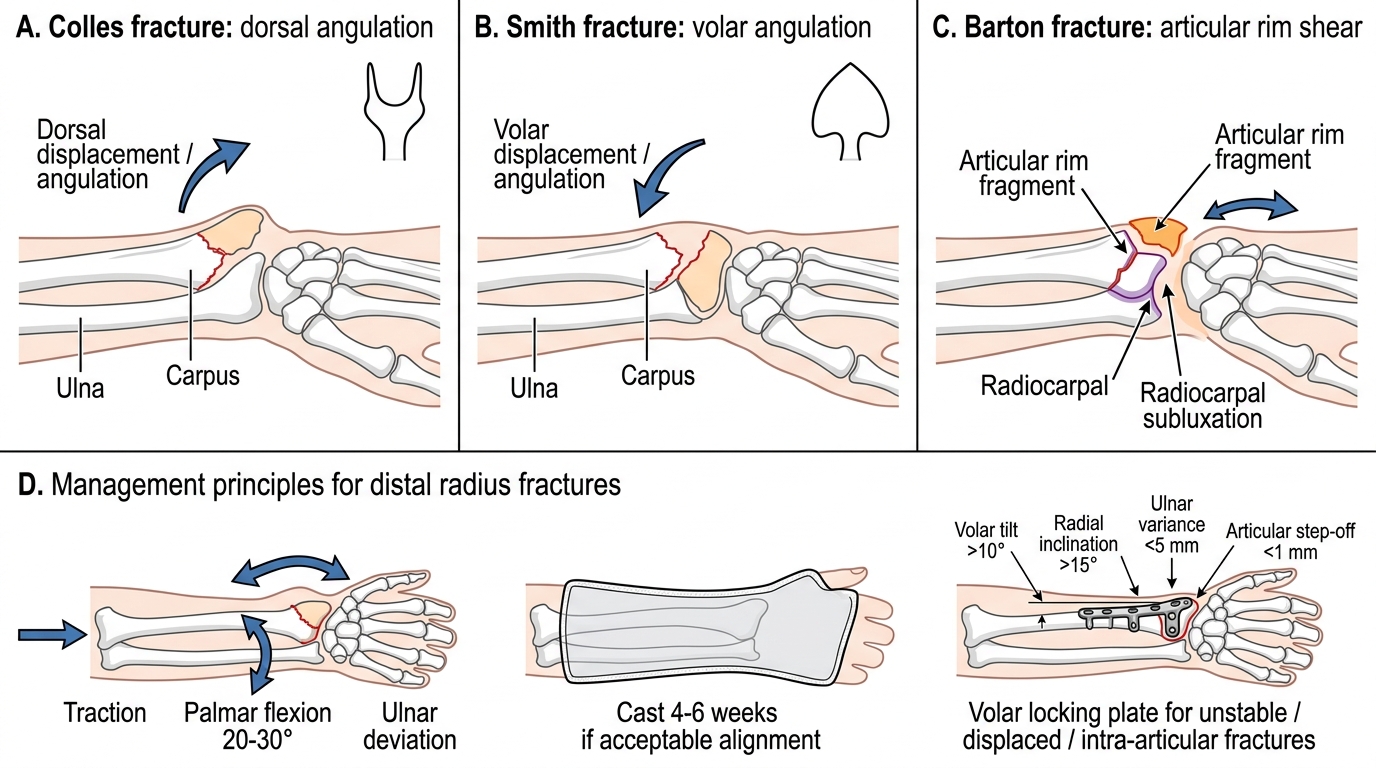
- Colles fracture: by far the most common; fracture of the distal radius (classically within 2.5 cm of the articular surface) with dorsal angulation and dorsal displacement of the distal fragment, producing the characteristic dinner-fork deformity on lateral view. Radial shortening and radial tilt are also present. The injury follows a fall on the outstretched hand in the elderly.
- Smith fracture (reverse-Colles): distal radius fracture with volar angulation and volar displacement of the distal fragment. Also called a 'garden-spade deformity.' Results from a fall on the back of the hand or direct impact on the dorsum. Requires different treatment (volar plate fixation in the operative group).
- Barton fracture: a shear fracture of the dorsal (dorsal Barton) or volar (volar Barton, more common) rim of the distal radius extending into the articular surface, with the carpus subluxating along with the sheared fragment; always articular and unstable.
The AO/OTA classification is the standard: type A (extra-articular), type B (partial articular), type C (complete articular -- both columns). The classification guides operative planning: articular fractures, especially type C, generally require ORIF to restore joint congruity.
Distal Radius Fractures: Colles, Smith, Barton and Management
Management of Distal Radius Fractures
Management of distal radius fractures has evolved with the widespread adoption of volar locking plates, particularly for displaced fractures in active patients. The decision framework integrates fracture pattern, degree of displacement, articular involvement, patient age, bone quality, and functional demands.
Acceptable parameters for non-operative management (in elderly, low-demand patients): radial tilt >10 degrees of volar, radial inclination >15 degrees, ulnar variance <5 mm, articular step-off <1 mm. Fractures meeting these criteria may be managed in a plaster cast for 4-6 weeks. Colles fractures that cannot hold reduction (redisplace within the cast) or that have initial shortening >10 mm, >20 degrees of dorsal tilt, or articular involvement generally do better with operative fixation.
Closed reduction technique for Colles fracture: longitudinal traction + palmar flexion + ulnar deviation, followed by a dorsal plaster slab in the reduced position. The Cotton-Loder position (forced palmar flexion + ulnar deviation) has been largely abandoned due to carpal tunnel nerve compression. Modern practice favours mild palmar flexion (20-30 degrees) and neutral to slight ulnar deviation.
Operative options for distal radius fractures:
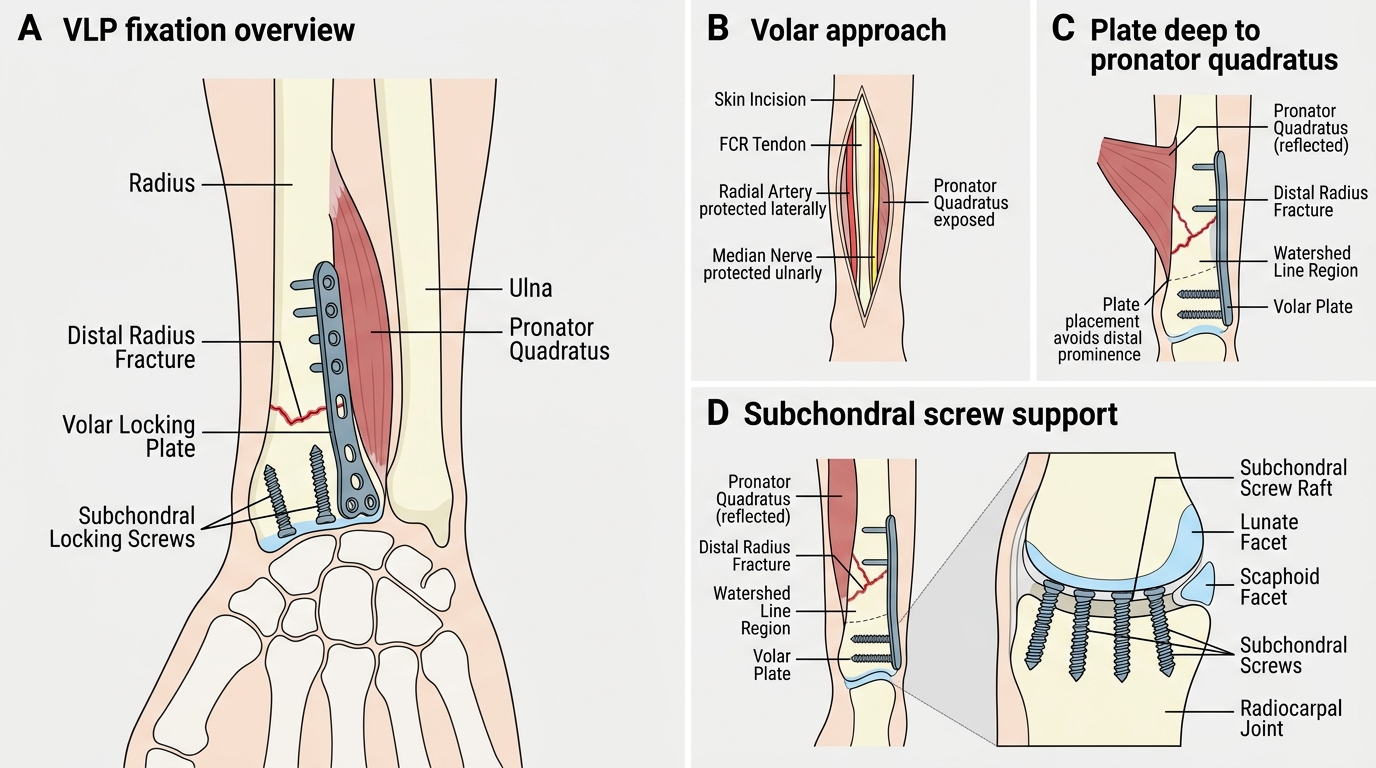
- Volar locking plate (VLP): the most common contemporary operative method; the volar approach (Henry) accesses the fracture; locking screws subchondrally support the articular surface; early mobilisation possible
- External fixation: ligamentotaxis maintains length in severely comminuted fractures; used as definitive treatment in elderly or as bridging in open fractures
- K-wire fixation: supplementary wires after closed reduction; simple, cost-effective, but requires plaster immobilisation
Associated injuries to recognise: scaphoid fracture (check anatomical snuffbox tenderness), DRUJ disruption (always screen the wrist for Galeazzi component), carpal ligament tears, median nerve compression (acute carpal tunnel syndrome -- burning paraesthesia of the thumb-index-middle fingers after distal radius fracture requires urgent decompression).
Volar Locking Plate Fixation of Distal Radius Fracture
Self-Assessment and Case Review
Consolidate your understanding with these scenario-based questions covering the key eponyms and management principles of this module.
Scenario A -- Eponym check: A radiograph shows a fracture of the proximal ulna with the radial head displaced anteriorly out of the elbow joint. Name this injury (Monteggia -- Bado type I). Now the reverse: a distal radius fracture with the ulnar head dorsally displaced at the wrist. Name this injury (Galeazzi). Confirm to yourself: Monteggia = proximal ULNA + radial head dislocation at ELBOW (PRUJ). Galeazzi = distal RADIUS + DRUJ disruption at WRIST.
Scenario B -- Distal radius management: A 65-year-old woman with osteoporosis sustains a Colles fracture with 20 degrees of dorsal tilt and 12 mm of radial shortening. After closed reduction, radiographs show improvement to 10 degrees of dorsal tilt and 8 mm shortening, but these are the immediate post-reduction films. She is placed in a plaster cast. At 1-week follow-up the fracture has redisplaced to 22 degrees of dorsal tilt. Management: the fracture is unstable and has redisplaced; operative fixation (volar locking plate) is now appropriate. Late post-reduction redisplacement in the cast is a well-recognised pattern in osteoporotic Colles fractures and is itself an operative indication.
Scenario C -- Compartment syndrome screen: After both-bones forearm ORIF, a patient develops severe forearm pain disproportionate to the expected post-operative level, along with paraesthesia of the fingers and pain on passive finger extension. What complication is suspected? Compartment syndrome of the forearm. Compartment pressure >30 mmHg (or DP <30 mmHg) mandates emergency fasciotomy. This complication can follow both injury and surgery.
Self-check: (1) Define the difference between Monteggia and Galeazzi injuries. (2) What is the dinner-fork deformity and which fracture does it describe? (3) What clinical sign suggests acute carpal tunnel syndrome after a distal radius fracture?
CLINICAL PEARL
The core rule of forearm trauma: never look at just the fracture -- image the whole forearm including both the elbow and the wrist. A Monteggia injury shows the ulna fracture but the radial head dislocation is in the elbow; a Galeazzi shows the radius fracture but the DRUJ disruption is at the wrist. An isolated single-bone forearm fracture is uncommon -- always ask 'where is the force transmitted?' and look at both joints.
SELF-CHECK
Which of the following correctly defines a Monteggia fracture-dislocation?
A. Fracture of the distal radius with disruption of the distal radioulnar joint
B. Fracture of the proximal ulna with dislocation of the radial head at the proximal radioulnar joint
C. Fracture of both radius and ulna at the same level
D. Fracture of the distal ulna with disruption of the distal radioulnar joint
Reveal Answer
Answer: B. Fracture of the proximal ulna with dislocation of the radial head at the proximal radioulnar joint
Monteggia fracture-dislocation = fracture of the proximal ulna + dislocation of the radial head at the proximal radioulnar joint (PRUJ, within the elbow). Option A describes Galeazzi. Option C is a both-bones fracture. Option D is a variant of Galeazzi-type DRUJ injury but with the ulna rather than the radius -- not the standard Monteggia definition.