Page 8 of 22
OR2.4 | Humeral Shaft Fracture with Neurovascular Risk — SDL Guide (Part 2)
Management
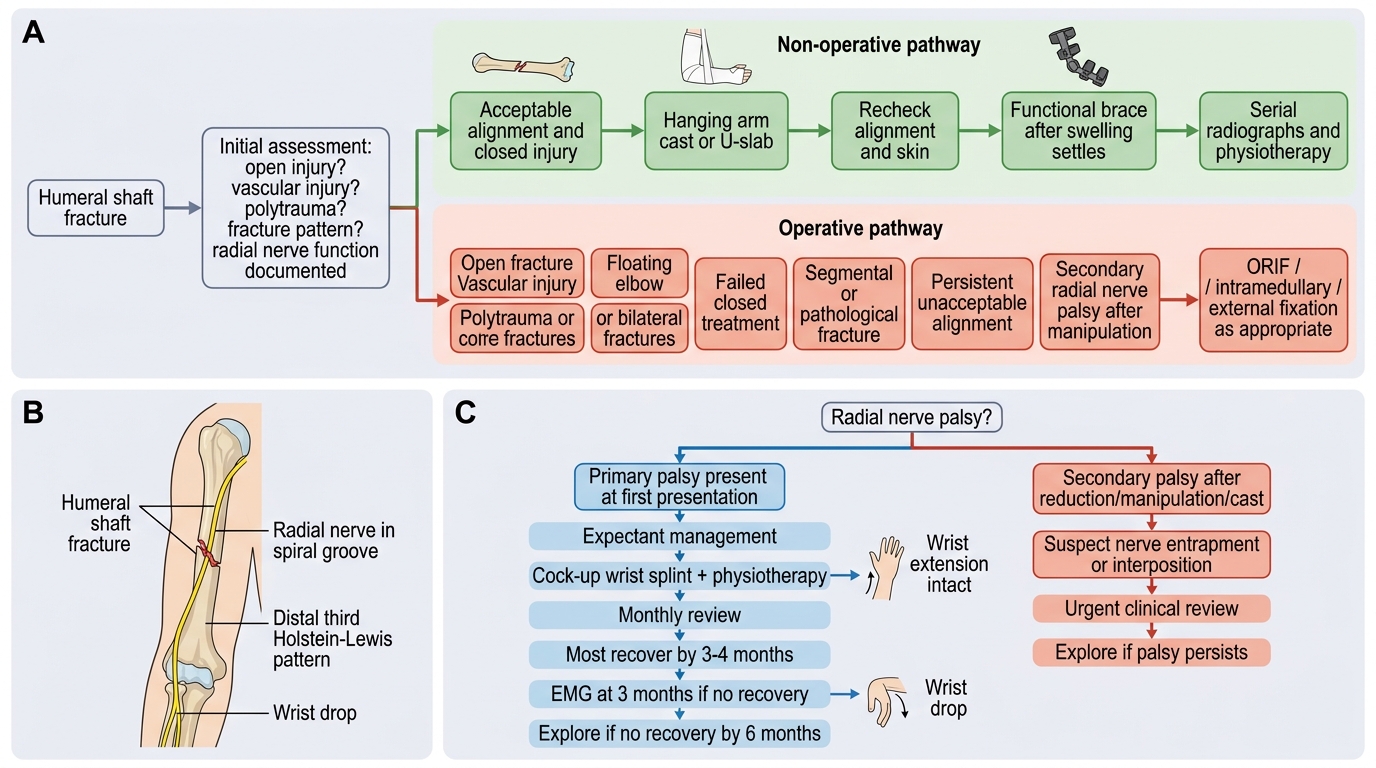
The management of humeral shaft fractures is primarily non-operative in the majority of closed, non-comminuted fractures. The humerus has significant tolerance for malunion: up to 20 degrees of anterior or varus angulation and up to 3 cm of shortening are acceptable functionally because the shoulder and elbow joints can compensate.
Non-operative management: The hanging-arm cast (U-slab or coaptation splint) uses gravity to apply longitudinal traction and is effective for displaced shaft fractures in the first 1-2 weeks. After swelling subsides, a functional fracture brace (Sarmiento brace) is applied -- a prefabricated or custom sleeve that creates hydraulic pressure from the soft tissues to maintain alignment while allowing elbow and shoulder movement; it is the gold standard non-operative device and achieves union in ~90% of isolated closed fractures. Pendulum exercises begin from day one to prevent shoulder stiffness; elbow flexion-extension is encouraged from week 2.
Operative indications for humeral shaft fractures include: open fracture, polytrauma (facilitates nursing/early mobilisation), bilateral humeral fractures, floating elbow (ipsilateral humeral shaft + forearm fracture), brachial artery injury requiring repair (plating at the same time as vessel repair), pathological fracture, failed closed management (unacceptable angulation/shortening), and Holstein-Lewis fracture with secondary radial nerve palsy or progressive palsy. The most common operative implants are: plate-and-screw fixation (anterolateral or posterior approach; the standard for most operative cases) and intramedullary nailing (antegrade -- risk of shoulder impingement; retrograde -- risk of elbow stiffness). External fixation is used for damage-control in polytrauma.
For radial nerve palsy management, the established principle is:
- Primary palsy (present at time of fracture): expectant management; spontaneous recovery in 70-90% within 3-4 months. Apply a cock-up wrist splint to maintain a functional wrist position and prevent contracture. Physiotherapy for passive joint maintenance. If no recovery by 3 months, EMG; if no recovery by 6 months, explore.
- Secondary palsy (post-manipulation): urgent exploration recommended.
For intercondylar (T-condylar) fractures of the humerus, the treatment in active adults is operative -- open reduction and internal fixation via the triceps-splitting or olecranon osteotomy approach, using parallel or perpendicular medial and lateral column plates. The ulnar nerve must be visualised and transposed (anteriorly) at surgery to prevent post-operative ulnar nerve compression. In elderly patients with severely comminuted articular fractures, total elbow arthroplasty is an option.
Management of Humeral Shaft Fractures and Radial Nerve Palsy
Self-Assessment: Key Scenarios
Apply the principles of this module to the following scenarios, confirming your understanding of the radial nerve trap and management decisions.
Scenario A: A 25-year-old presents with a mid-shaft humeral spiral fracture after arm-wrestling. On arrival he has intact wrist extension. After reduction and application of a hanging-arm cast, he is unable to extend the wrist. This is a secondary (post-manipulation) radial nerve palsy. Management: the nerve may be entrapped in the fracture or soft tissues. This requires urgent clinical review and, if palsy persists, surgical exploration. The surgeon should explore the radial nerve at the fracture site and confirm it is not interposed.
Scenario B: A 55-year-old woman is found to have wrist drop after a distal third spiral humeral shaft fracture (Holstein-Lewis pattern). Pre-fracture nerve function was normal (documented). The wrist drop was present at first presentation. This is a primary radial nerve palsy in a Holstein-Lewis fracture. Management: expectant -- apply a cock-up wrist splint, begin physiotherapy, monitor monthly. Most will recover by 3-4 months. EMG at 3 months if no recovery; explore if no recovery by 6 months.
Scenario C: A 40-year-old is brought in after a motor vehicle accident with a humeral shaft fracture and an open wound exposing the bone (Gustilo-Anderson type II). Management priorities: antibiotics within 1 hour (cephalosporin IV); tetanus prophylaxis; urgent debridement and irrigation; stabilisation (plating preferred for open fractures requiring operative access); radial nerve assessment documented before and after surgery.
Self-check: (1) Name the artery at risk in humeral shaft fractures and how to assess it. (2) What is the acceptable deformity tolerance for non-operative humeral shaft fracture management? (3) What is the approximate rate of spontaneous radial nerve recovery in primary palsies?
CLINICAL PEARL
The single most important procedural rule for humeral shaft fractures: document radial nerve status BEFORE manipulation. A primary palsy present at injury is a neuropraxia in ~90% of cases and recovers spontaneously; a secondary palsy after manipulation suggests nerve entrapment and requires early exploration. Write the nerve examination findings in the notes and on the cast card. A 'found it after the cast' scenario is a preventable medico-legal problem.
SELF-CHECK
A 35-year-old presents with a Holstein-Lewis fracture. Why does this specific fracture pattern carry a higher radial nerve injury risk than a proximal shaft fracture?
A. The radial nerve is thinner in the distal humerus
B. The radial nerve pierces the lateral intermuscular septum at the distal third and is tethered there, making it unable to escape displacement at this level
C. The brachial artery occludes the nerve in the distal arm
D. Distal shaft fractures always involve the elbow, stretching the nerve over the joint
Reveal Answer
Answer: B. The radial nerve pierces the lateral intermuscular septum at the distal third and is tethered there, making it unable to escape displacement at this level
The Holstein-Lewis zone is at the distal third of the humeral shaft where the radial nerve transitions from the posterior compartment to the anterior compartment by piercing the lateral intermuscular septum. At this point the nerve is tethered against the bone and cannot easily escape a fracture that displaces or spirals here, explaining the ~22% nerve injury rate (versus ~12% overall). This anatomical choke point is the pathological basis for the higher risk.