Page 13 of 22
OR2.3 | Joint Pain Medication Selection — SDL Guide
Learning Objectives
- Select appropriate analgesic and anti-inflammatory medications for joint pain based on aetiology, severity, and patient comorbidities
- Apply the WHO analgesic ladder to musculoskeletal pain and prescribe NSAIDs safely with gastric and renal protection
- Differentiate pharmacological management of acute traumatic joint pain, inflammatory arthritis, and degenerative joint pain
- Communicate medication benefits, risks, and monitoring requirements to patients clearly and in non-technical language
- Prescribe corticosteroid joint injections appropriately and recognise contraindications
INSTRUCTIONS
Selecting and prescribing appropriate pain medications for joint conditions is one of the most common clinical tasks in any practice setting -- from the casualty officer managing a fresh fracture to the primary care physician treating osteoarthritis. Orthopaedic competency OR2.3 specifically requires the ability to select, prescribe, and communicate medications for joint pain. This module builds on your pharmacology knowledge and applies it clinically to the orthopaedic context, emphasising the patient consultation and shared decision-making skills that distinguish safe prescribing from mechanical drug selection.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch 3 -- Pain Management in Orthopaedics (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 1 -- Orthopaedic Examination and Management (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 58-year-old man with known peptic ulcer disease and mild chronic kidney disease (eGFR 55 mL/min) presents to your orthopaedic outpatient clinic with bilateral knee pain due to osteoarthritis. He is taking low-dose aspirin for secondary prevention. A colleague has already prescribed ibuprofen 400 mg three times daily without any gastroprotection. The patient now reports worsening epigastric pain and ankle swelling. What prescribing error occurred, what is the correct approach, and how would you communicate the need to change his medications?
WHY THIS MATTERS
Joint pain medication selection is not a mechanical task -- it requires integrating the diagnosis, the mechanism of pain, the patient's comorbidities, their current medications, and the likely duration of treatment. NSAIDs are among the most commonly prescribed drugs in the world and among the most commonly misused, with well-documented gastrointestinal, renal, and cardiovascular toxicity that is often preventable by appropriate prescribing and monitoring. The ability to select medications, explain risks in lay language, identify contraindications, and conduct a monitoring conversation is a core competency that will be tested in clinical examinations and applied daily in practice.
RECALL
From your pharmacology course, recall that pain medications for musculoskeletal conditions are broadly classified into non-opioid analgesics (paracetamol), NSAIDs (ibuprofen, diclofenac, naproxen, celecoxib), weak opioids (codeine, tramadol), strong opioids (morphine, oxycodone), disease-modifying antirheumatic drugs (DMARDs -- methotrexate, sulfasalazine, hydroxychloroquine), and intra-articular therapies (corticosteroids, hyaluronic acid). The WHO analgesic ladder (originally developed for cancer pain) has been adapted for musculoskeletal pain: step 1 = non-opioids; step 2 = mild opioids +/- non-opioids; step 3 = strong opioids. Recall that NSAIDs work by inhibiting cyclo-oxygenase (COX-1 and COX-2), reducing prostaglandin synthesis -- hence their anti-inflammatory and analgesic effects, and also their gastric and renal side effects.
Clinical Indication and Classification of Joint Pain
Provided image
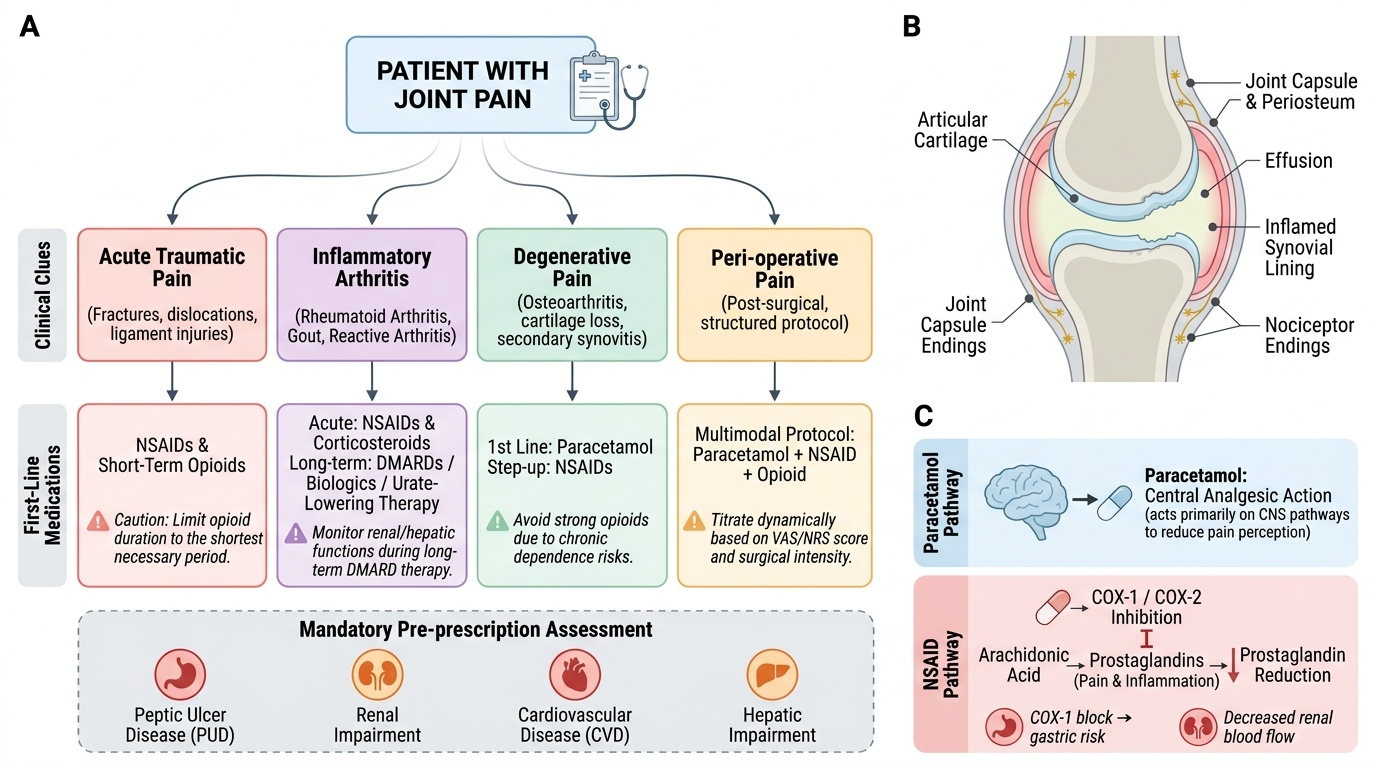
The first step in selecting appropriate joint pain medication is to correctly classify the type of joint pain, because the mechanism of pain determines the most effective drug class. Joint pain in orthopaedics falls into four broad categories, each with distinct pharmacological implications.
Acute traumatic joint pain (fractures, dislocations, ligament injuries, post-operative pain) involves acute nociceptive pain from tissue injury and inflammation; NSAIDs and opioids are appropriate in the short term, but opioids must be used with caution and for the shortest necessary duration. Inflammatory arthritis (rheumatoid arthritis, gout, reactive arthritis) involves cytokine-mediated synovitis; NSAIDs and corticosteroids are effective acutely, but disease-modifying therapy (DMARDs or biologics in rheumatoid arthritis, urate-lowering therapy in gout) is the cornerstone of long-term management. Degenerative joint pain (osteoarthritis) involves cartilage loss and secondary synovitis; paracetamol is first-line; NSAIDs are step-up therapy; strong opioids are rarely appropriate for chronic degenerative pain due to dependence risk. Peri-operative pain (post-surgical) requires a structured multimodal analgesia protocol: paracetamol + NSAID + opioid as a combination, titrated by the pain score and surgical intensity.
A careful patient history and physical examination are indispensable before prescribing: establish the pain mechanism (nociceptive, inflammatory, neuropathic), the severity (VAS or NRS 0-10), the functional impact, and the key comorbidities that modify drug choice -- peptic ulcer disease, renal impairment, cardiovascular disease, and hepatic impairment.
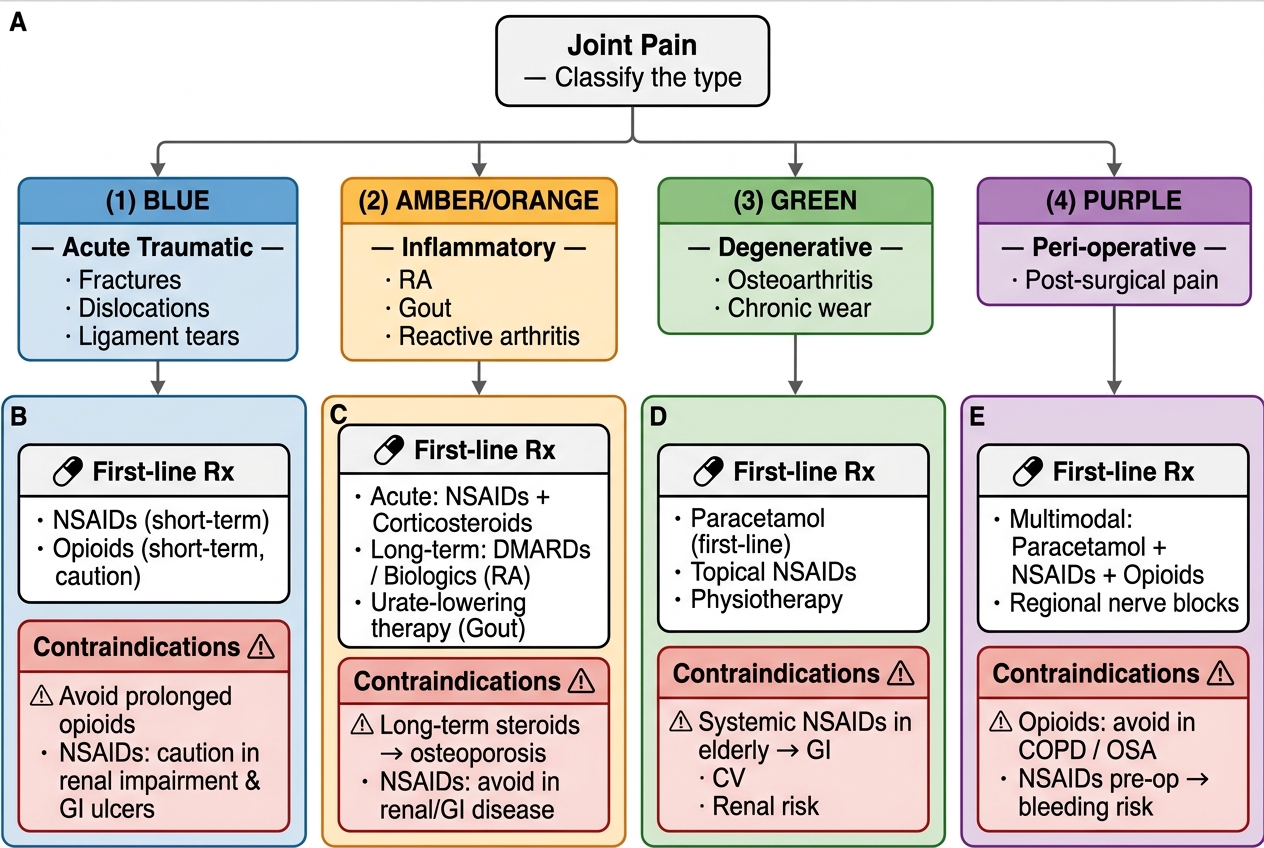
Joint Pain Classification: Decision Tree with First-Line Pharmacotherapy
Anatomy and Governing Pharmacological Principles
Understanding the pharmacological principles that govern safe prescribing requires a working knowledge of the mechanisms, indications, and toxicity profiles of the main drug classes used for joint pain. The prescriber must internalise these before reaching for a prescription pad, as the most common prescribing errors arise from failure to account for an existing contraindication or drug interaction.
Paracetamol (acetaminophen): Works by a central prostaglandin-independent mechanism (exact mechanism still partially debated). Effective for mild-to-moderate pain; has no anti-inflammatory activity. Remarkably safe when used within the recommended dose (adults: 500-1000 mg every 4-6 hours, maximum 4 g/day). Hepatotoxic in overdose or with chronic alcohol use. No gastroprotection required. No renal restriction at standard doses.
NSAIDs (non-steroidal anti-inflammatory drugs): Inhibit COX-1 (gastroprotective prostaglandins, platelet thromboxane) and COX-2 (inflammatory prostaglandins, vascular prostacyclin). Traditional non-selective NSAIDs (ibuprofen, diclofenac, naproxen) inhibit both; selective COX-2 inhibitors (celecoxib, etoricoxib) spare COX-1 and thus have a lower GI risk. Key safety rules for NSAIDs:
- Always co-prescribe a proton pump inhibitor (PPI) in patients with peptic ulcer disease history, elderly patients, or those on concomitant aspirin or corticosteroids
- Avoid in renal impairment (eGFR <30 mL/min is an absolute contraindication; use with caution if eGFR 30-60)
- Use the lowest effective dose for the shortest necessary duration
- Avoid in patients with decompensated heart failure (fluid retention risk)
- Selective COX-2 inhibitors carry an increased cardiovascular risk -- avoid in ischaemic heart disease unless benefit outweighs risk
Opioids: Used for moderate-to-severe acute pain or post-operative pain. In the orthopaedic context, codeine (weak opioid) and tramadol are used for step-2 pain; morphine for post-operative step-3 pain. Side effects: constipation, nausea, sedation, respiratory depression. Do not use strong opioids for chronic degenerative pain as a routine.
Corticosteroids (intra-articular): Injections of methylprednisolone or triamcinolone into the joint cavity provide rapid anti-inflammatory relief for inflammatory arthritis flares and osteoarthritis. Systemic absorption is minimal but not absent. Contraindications: joint infection (septic arthritis -- corticosteroid injection into an infected joint is catastrophic), coagulopathy, skin infection over the injection site. Frequency limit: no more than 3-4 injections per joint per year, spaced at least 3 months apart, to avoid cartilage toxicity.
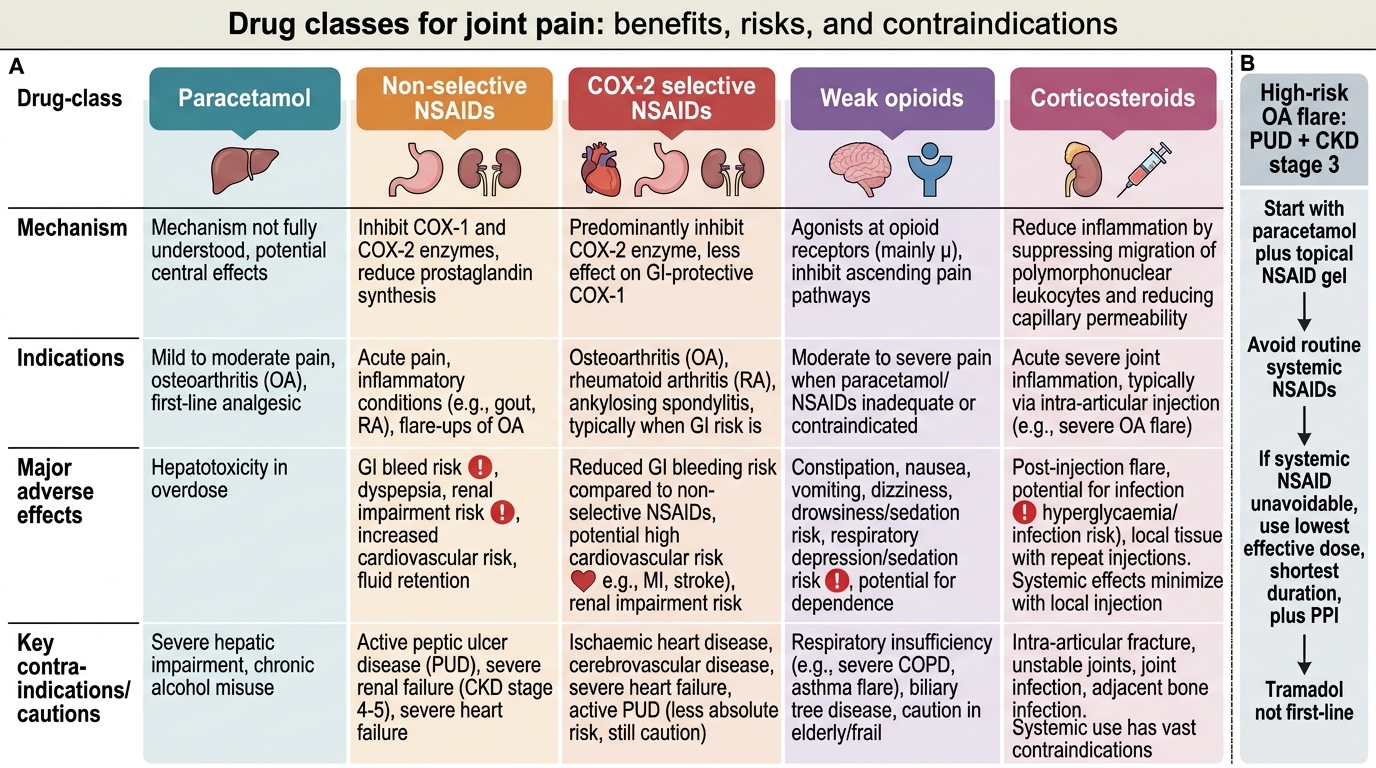
Main Drug Classes for Joint Pain
SELF-CHECK
A 60-year-old patient with known peptic ulcer disease and CKD stage 3 (eGFR 45 mL/min) presents with acute knee osteoarthritis flare. Which analgesic regimen is most appropriate?
A. Ibuprofen 400 mg TDS (no gastroprotection needed for short courses)
B. Paracetamol 1 g QDS + topical NSAID gel; PPI if systemic NSAID required at lowest dose
C. Celecoxib 200 mg BD (COX-2 selective; no gastroprotection needed in this context)
D. Tramadol 50 mg TDS as first-line analgesic
Reveal Answer
Answer: B. Paracetamol 1 g QDS + topical NSAID gel; PPI if systemic NSAID required at lowest dose
With peptic ulcer disease and CKD eGFR 45 mL/min, systemic NSAIDs carry significant GI and renal risks. The correct first step is paracetamol at maximum safe doses, with topical NSAID as a low-systemic-absorption alternative. If a systemic NSAID is unavoidable (inadequate response), use the lowest effective dose for the shortest duration AND add a PPI. Celecoxib option C is wrong because COX-2 inhibitors still require gastroprotection in high-GI-risk patients (guidelines recommend PPI co-prescription) and carry cardiovascular risk; eGFR 45 is also a caution zone. Tramadol is not first-line for degenerative joint pain.
Procedure and Prescribing Technique
Provided image
The act of prescribing for joint pain is a clinical skill with defined steps, not merely writing a drug name. A safe prescribing consultation in the orthopaedic setting follows this sequence and can be practised as a structured procedure. Internalising this sequence transforms an ad hoc habit into a reproducible clinical skill that protects both the patient and the prescriber. Each step has a specific purpose: the diagnosis step prevents the wrong drug class being chosen; the contraindication screen prevents harm from a predictable interaction; the dose-selection step minimises toxicity; and the safety-net step ensures the patient knows when to seek help. Practised together, these four steps constitute the safe prescriber framework.
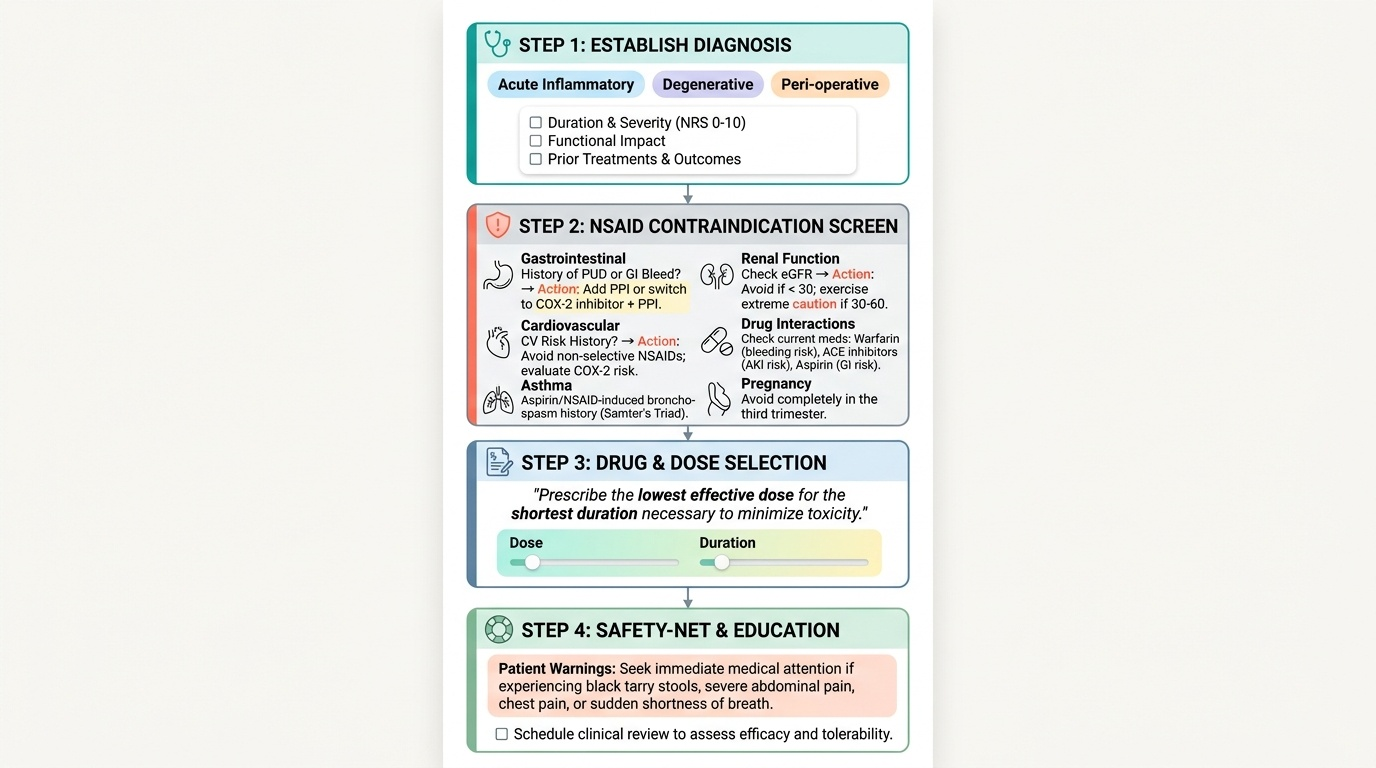
Step 1 -- Establish the diagnosis and pain mechanism. Is this acute inflammatory, degenerative, or peri-operative pain? This determines the drug class (see arc step 1). Ask about duration, severity (NRS 0-10), functional impact, and previous treatments and their outcomes.
Step 2 -- Screen for contraindications. Run through a mental checklist before prescribing any NSAID:
- Past history of peptic ulcer disease or GI bleed? -> Add PPI or switch to COX-2 inhibitor with PPI
- Renal function (eGFR)? -> Avoid NSAIDs if eGFR <30; caution 30-60
- Cardiovascular history? -> Avoid non-selective NSAIDs + consider cardiovascular risk with COX-2 inhibitors
- Current medications? -> Check for interactions: NSAIDs + warfarin (bleeding risk), NSAIDs + ACE inhibitors (acute kidney injury risk), NSAIDs + aspirin (additive GI risk)
- Asthma? -> ~10% of asthmatics have aspirin/NSAID-induced bronchospasm (Samter's triad)
- Pregnancy? -> Avoid NSAIDs in the third trimester (premature closure of ductus arteriosus)
Step 3 -- Select the drug, dose, and duration. Use the lowest effective dose for the shortest necessary duration. Write the drug name (generic), dose, route, frequency, and duration explicitly. Include instructions (with or after food for NSAIDs). If adding a PPI (e.g. omeprazole 20 mg OD), write it simultaneously.
Step 4 -- Safety-net and monitoring. Tell the patient what to watch for: GI symptoms (epigastric pain, black stools for NSAIDs), ankle swelling (renal retention), and skin rash. Give a review date. If the patient is on NSAIDs for >2 weeks, check urea and creatinine.
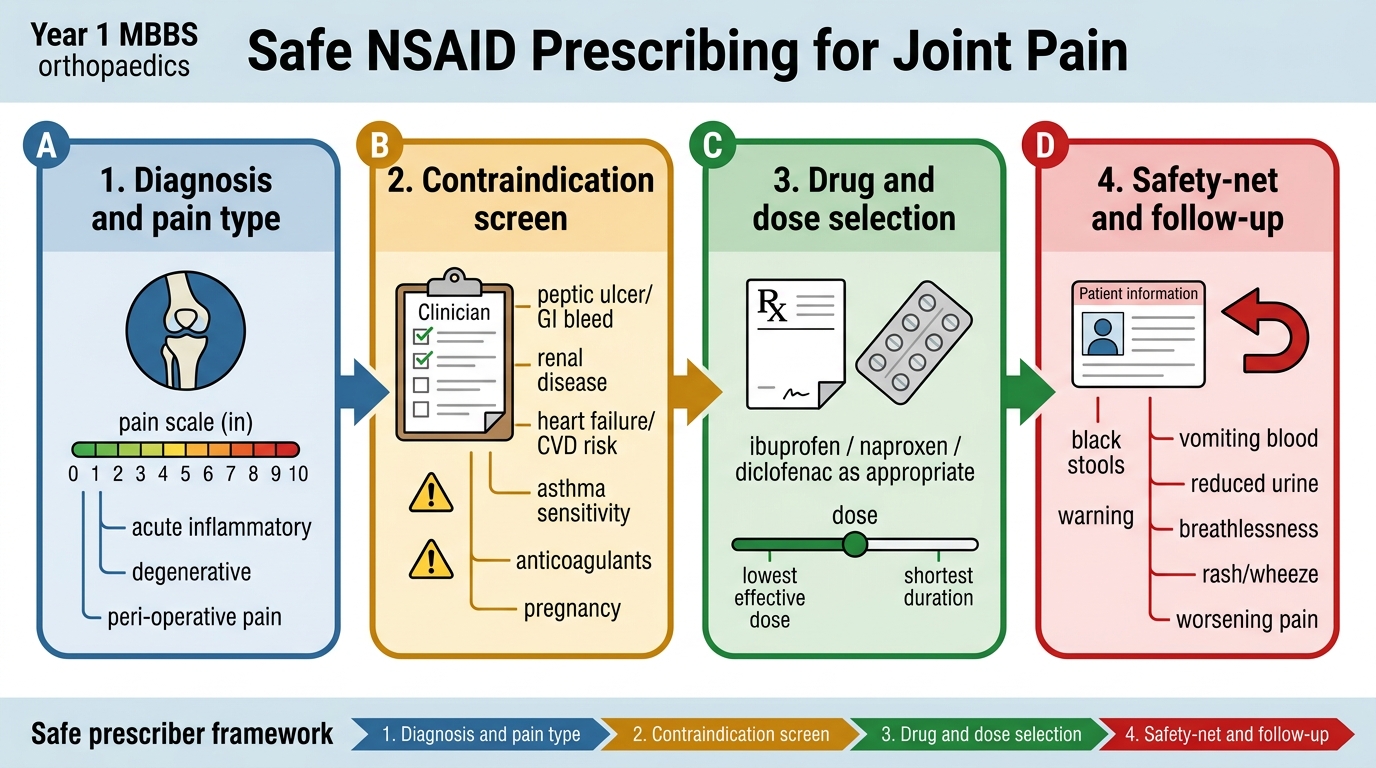
Safe NSAID Prescribing Checklist for Joint Pain