Page 14 of 22
OR2.3 | Joint Pain Medication Selection — SDL Guide (Part 2)
Interpretation: Monitoring and Outcome Assessment
The interpretation step in orthopaedic pain medication skills concerns monitoring the patient's response to treatment and recognising treatment failure or adverse effects -- two different but equally important clinical endpoints. A drug can be effective (pain reduced) but simultaneously causing harm (renal impairment, GI ulceration), and detecting either outcome requires a proactive monitoring plan at the time of prescribing, not a reactive response after the patient re-presents with a complication. For a prescribing competency, 'interpretation of findings' means reviewing the patient on therapy using specific clinical and biochemical markers, responding to abnormal findings by adjusting or stopping treatment, and documenting the review clearly. Each major drug class has its own monitoring framework.
For NSAID therapy, the key monitoring parameters are:
- Symptom response: is pain NRS score reduced by >=50% at 2-4 weeks? If not, step up (add opioid, consider intra-articular injection) or re-evaluate the diagnosis
- GI symptoms: new epigastric pain, heartburn, or melaena in a patient on NSAIDs requires stopping the NSAID, obtaining stool occult blood, and GI referral if positive
- Renal function: urea and creatinine at 2 weeks if eGFR was borderline or if any ankle oedema develops; a rise >25% from baseline is an indication to stop
- Blood pressure: NSAIDs can raise blood pressure by 3-5 mmHg on average; check in hypertensive patients at 2-4 weeks
For intra-articular corticosteroid injection, monitor the patient at 4-6 weeks: assess the duration of benefit (typically 4-8 weeks), whether function improved, and whether there is any sign of joint infection (fever, warmth, swelling, increasing pain within 24-72 hours of injection -- this is septic arthritis until proven otherwise and requires immediate joint aspiration and cultures).
For opioids, use the 4 A's: Analgesia (is it working?), Activities (has function improved?), Adverse effects (constipation, sedation, falls risk?), and Aberrant behaviour (evidence of misuse?). Post-operative opioids should be stepped down and discontinued as pain resolves -- not continued indefinitely.
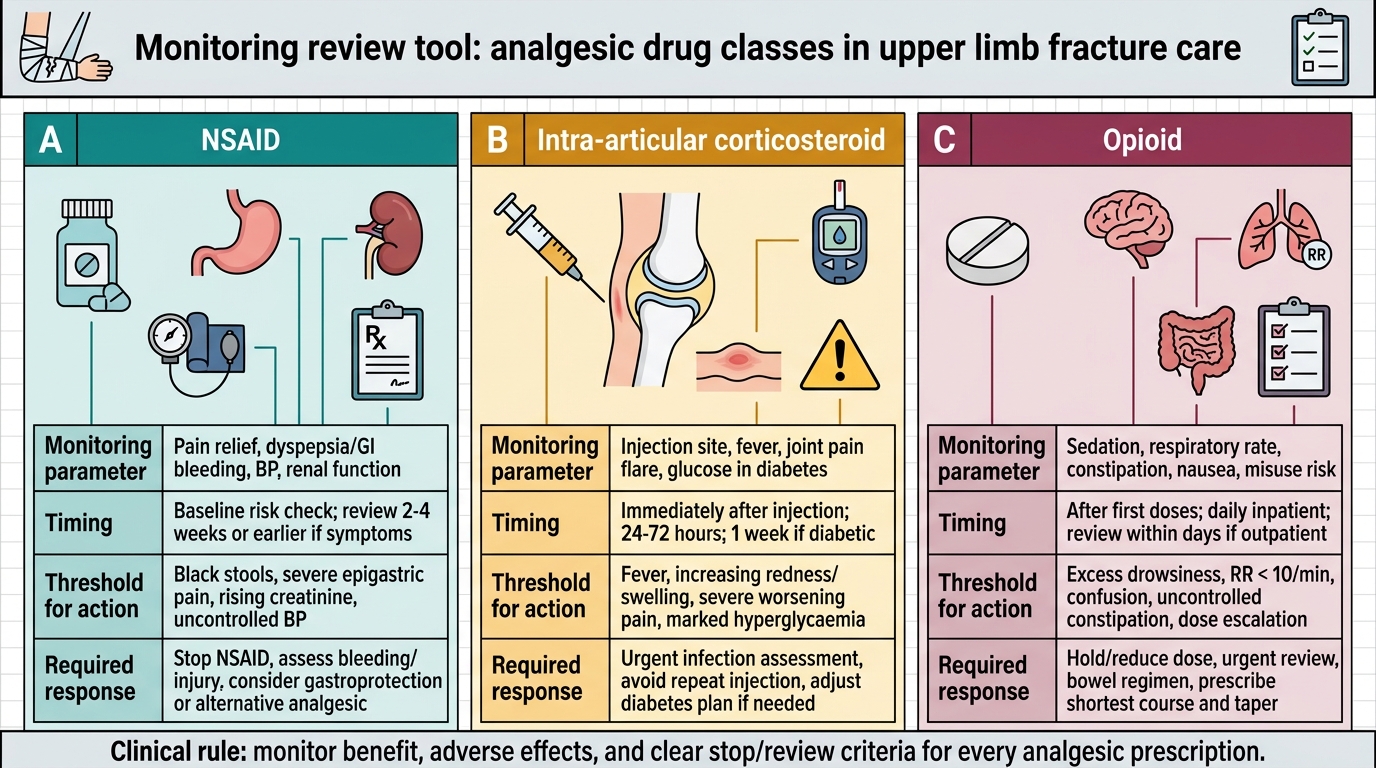
Monitoring Review Tool for Analgesic Drug Classes
Applied and Supervised Practice: Patient Communication
The communication step in OR2.3 is the most practically visible component: the ability to explain a prescribed medication to a patient in clear, non-technical language, including why it is prescribed, how to take it, what side effects to watch for, and when to seek help. This is a core clinical skill assessed in OSCEs and clinical examinations.
A structured communication template for explaining an NSAID prescription to a patient with joint pain can be practised using the following framework:
Opening -- establish understanding: 'I am prescribing you a medication called naproxen/ibuprofen, which belongs to a class of drugs we call anti-inflammatory painkillers. They work by reducing the swelling and inflammation inside your joint, which is what is causing your pain.'
How to take it: 'Take one tablet [dose] with or after food, [frequency]. Do NOT take it on an empty stomach as it can irritate the stomach lining.'
Duration and review: 'I am prescribing this for [duration -- short course preferred]. I want to see you in [2-4 weeks] to check it is working and to check your kidneys have not been affected.'
Side effects to watch for: 'The most important thing to watch for is stomach pain, heartburn, or black-coloured stools -- this can mean the drug is irritating the stomach lining. If you notice this, stop the tablet and contact me immediately. Also watch for ankle swelling or reduced urine output, which can mean the kidneys are being affected.'
Other medications check: 'Are you taking any blood thinners like warfarin, or blood pressure tablets? Some anti-inflammatory tablets can interact with these.'
Gastroprotection explanation (when co-prescribed PPI): 'I am also prescribing you a stomach-protecting tablet called omeprazole. Take this once daily in the morning before breakfast. It protects the stomach lining from the irritant effect of the anti-inflammatory.'
In the supervised practice context, a student should be able to role-play this consultation with a simulated patient, taking no more than 5 minutes, covering all four elements -- indication, instructions, side effects, monitoring.
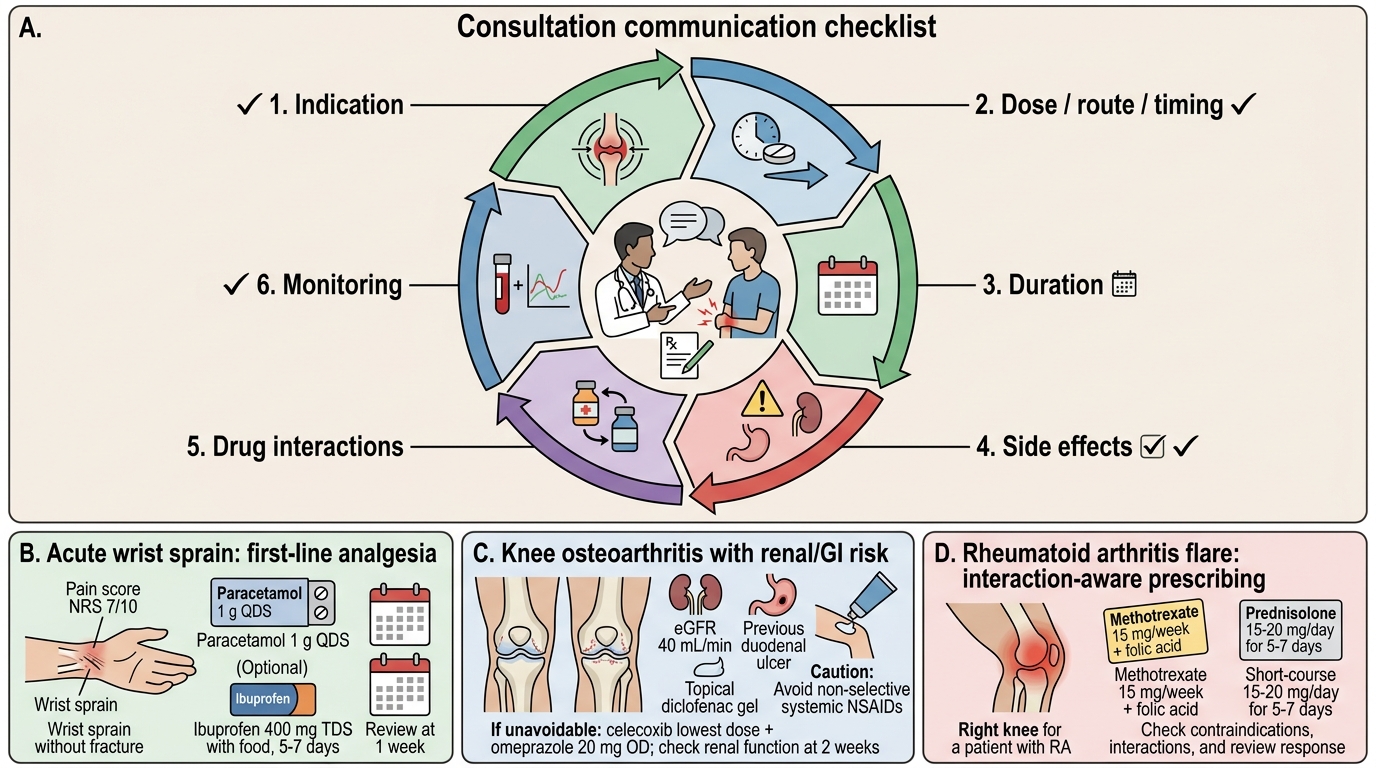
Six-Element Communication Checklist for Joint Pain Prescribing
Self-Assessment: Prescribing Scenarios
Test your prescribing decisions and communication skills with the following cases.
Scenario A: A 45-year-old healthy male with acute wrist sprain (no fracture), pain NRS 7/10, no comorbidities. Correct approach: paracetamol 1 g QDS as first-line; if inadequate, add ibuprofen 400 mg TDS with food for 5-7 days; no PPI required if short course and no GI history. Explain that the anti-inflammatory will reduce pain and swelling. Review at 1 week; if resolved, stop NSAID.
Scenario B: A 70-year-old woman with bilateral knee osteoarthritis, eGFR 40 mL/min, and previous duodenal ulcer (treated 2 years ago). Pain NRS 6/10, interfering with walking. Correct approach: paracetamol 500 mg-1 g QDS first-line; topical diclofenac gel to the knees as a low-systemic option; if systemic NSAID unavoidable -- celecoxib at lowest dose WITH omeprazole 20 mg OD; monitor renal function at 2 weeks. Avoid non-selective NSAIDs. Not a candidate for opioids as first-step therapy for chronic degenerative pain.
Scenario C: A 55-year-old with known rheumatoid arthritis has an acute joint flare in the right knee. Current medications: methotrexate 15 mg/week, folic acid. Correct approach: short course of oral prednisolone 15-20 mg/day for 5-7 days (bridge therapy during flare) OR intra-articular methylprednisolone injection into the right knee. NSAIDs are a reasonable add-on but increase GI risk with methotrexate. Ensure the joint is not infected before any steroid intervention (examination, synovial fluid WBC if any doubt).
Self-check: (1) What three comorbidities should always be screened before prescribing an NSAID? (2) Why is a PPI often co-prescribed with an NSAID? (3) What is the maximum frequency of intra-articular corticosteroid injections to avoid cartilage toxicity?
CLINICAL PEARL
The most common prescribing error in joint pain is giving an NSAID without gastroprotection to a patient with a history of peptic ulcer or on aspirin. The second most common is failing to check renal function before prescribing NSAIDs in an elderly patient or one with known CKD. A 30-second comorbidity screen (GI history? Renal function? CVD? Current anticoagulation?) before writing any NSAID prescription prevents the majority of NSAID-related hospitalisations.
SELF-CHECK
A patient on long-term diclofenac for osteoarthritis develops acute kidney injury (creatinine rise >30% from baseline). What is the immediate management?
A. Switch to a selective COX-2 inhibitor, which does not affect the kidneys
B. Reduce the diclofenac dose by half and recheck creatinine in 1 week
C. Stop the diclofenac immediately; ensure adequate hydration; recheck renal function in 48-72 hours; involve nephrology if not improving
D. Add a potassium-sparing diuretic to manage the fluid retention component
Reveal Answer
Answer: C. Stop the diclofenac immediately; ensure adequate hydration; recheck renal function in 48-72 hours; involve nephrology if not improving
All NSAIDs -- including both non-selective and COX-2 selective -- can cause renal vasoconstriction and acute kidney injury by inhibiting prostaglandin-mediated afferent arteriolar dilation. A >25-30% creatinine rise is an indication to stop the NSAID immediately. Hydration is essential. Renal function must be re-evaluated at 48-72 hours. Persistent elevation requires nephrology input. Neither dose reduction nor switching to a COX-2 inhibitor is safe until renal function has returned to baseline.