Page 10 of 20
OR3.3 | Operative Source Control Assistance — SDL Guide
Learning Objectives
- Describe the indications for operative source control in musculoskeletal infection — drainage of abscess, sequestrectomy/saucerisation, and arthrotomy
- Identify the anatomical principles governing surgical access to infected bone and joints for each major operative procedure
- Explain the rationale for each operative step in drainage, sequestrectomy, and arthrotomy, and the role of dead-space management
- Describe the team-assist roles expected of a final-year student during these procedures, including instrument handling, wound irrigation, and specimen collection
- Recognise post-operative complications — wound infection, recurrence, neurovascular injury — and their early signs
INSTRUCTIONS
Operative source control is the definitive treatment for established musculoskeletal infection that has progressed beyond what antibiotics alone can manage. As a final-year student you will scrub in as a team member for abscess drainage, sequestrectomy, and arthrotomy procedures. Understanding the surgical anatomy, the rationale for each step, and your specific team role transforms you from a passive observer into an active, safe contributor. This module prepares you for theatre participation while building the conceptual framework you need to counsel patients about these procedures.
References
- Maheshwari's Essential Orthopaedics, Ch 20 — Infections of Bone and Joints (textbook)
- Apley and Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 2 — Infection (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 14-year-old boy has been admitted with chronic osteomyelitis of the right tibia. His plain X-ray shows a dense, radio-opaque bone fragment — a sequestrum — surrounded by a thickened bony shell (involucrum), with a sinus tract discharging pus to the skin for the past four months. He has been on antibiotics for six weeks with no improvement. The consultant tells the team: 'He needs theatre today.' As you scrub in as the fourth member of the operating team, the consultant asks what you know about what is about to happen and why antibiotics alone will never cure this patient. Can you explain?
WHY THIS MATTERS
Operative source control — the physical removal or decompression of infected tissue — is the principle that separates curable from incurable musculoskeletal infection. No antibiotic reaches avascular dead bone; no systemic drug can drain a walled-off abscess cavity; no conservative measure can remove the nidus of chronicity. As a future clinician managing patients with osteomyelitis, septic arthritis, or soft-tissue abscesses, you must understand not only why surgery is required but precisely what each operation achieves. This knowledge enables you to counsel patients preoperatively, participate safely in theatre, and recognise post-operative complications before they become catastrophic.
RECALL
Recall from previous modules: (1) A sequestrum is dead, avascular cortical bone — antibiotics require a blood supply to reach bacteria and cannot sterilise avascular tissue. (2) Involucrum is reactive periosteal new bone surrounding the sequestrum; cloacae are its perforations through which pus drains via sinus tracts. (3) Arthrotomy means surgical opening of a joint; the hip is the most urgent joint to open in children because raised intra-articular pressure can cause avascular necrosis. (4) Aseptic technique in theatre requires a sterile surgical field, gown, gloves, drapes, and instrument counts at the start and end of every procedure.
Indications for Operative Source Control
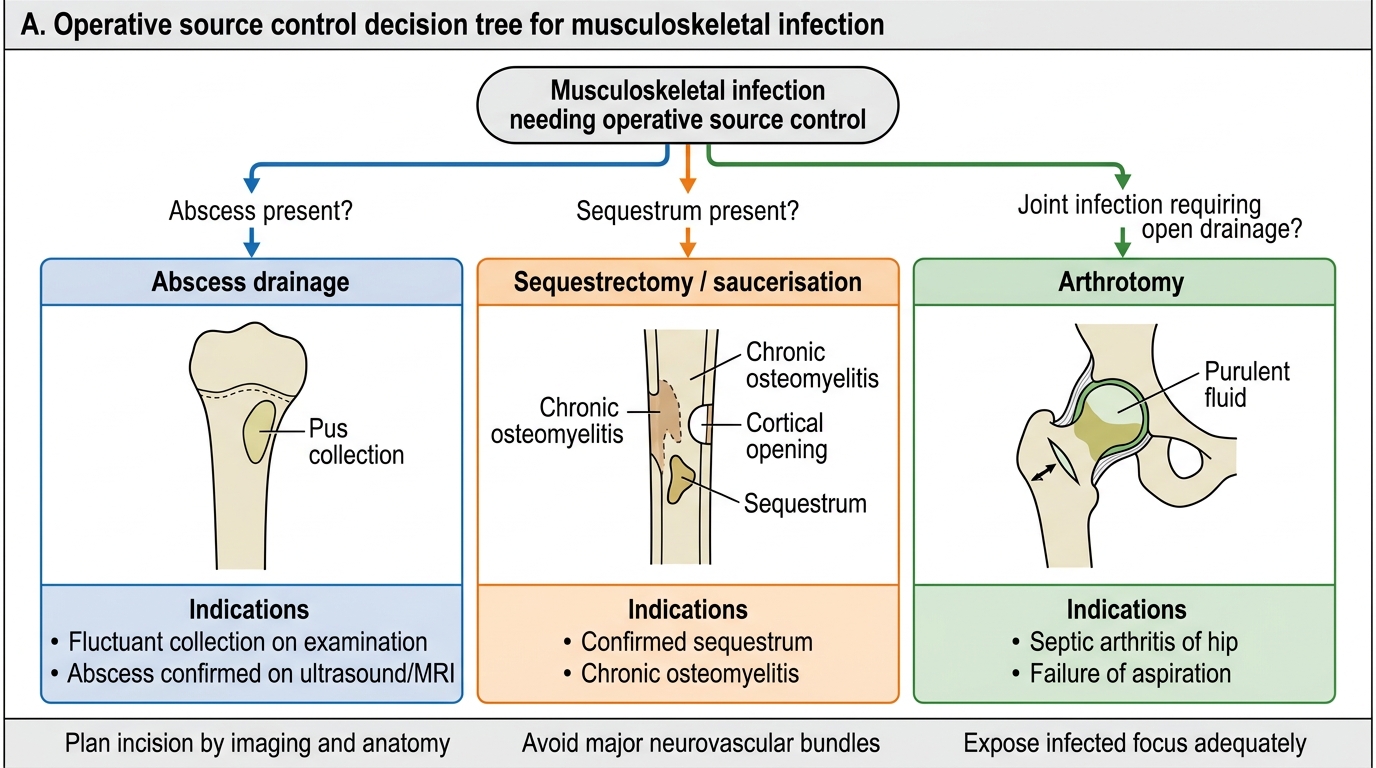
The decision to proceed to operative source control in musculoskeletal infection is driven by two fundamental principles: the inability of antibiotics to reach avascular or walled-off infection, and the urgency to prevent irreversible tissue destruction. The specific indications for each procedure are distinct and must be understood precisely.
Surgical drainage of soft-tissue and subperiosteal abscess is indicated when imaging (ultrasound or MRI) demonstrates a fluctuant collection, when there is failure to respond to 36-48 hours of appropriate antibiotics, or when clinical signs of abscess (fluctuance, pointing, skin thinning) are present. Abscess drainage is an urgent but not always emergency procedure — unless the overlying skin is thin and at risk of spontaneous rupture (which would contaminate the field), or unless the patient is septic.
Sequestrectomy and saucerisation are indicated in established chronic osteomyelitis with a radiologically visible sequestrum. The avascular sequestrum is the permanent reservoir of infection; as long as it remains, the infection will recur regardless of antibiotic duration. The indications are: (1) confirmed radiological sequestrum (on CT or MRI), (2) discharging sinus tract, (3) repeated acute exacerbations on antibiotics, and (4) Cierny-Mader Grade III-IV disease. Preoperative CT scanning is preferred over MRI for sequestrum localisation because CT better defines the extent and position of cortical dead bone.
Arthrotomy (surgical opening of a joint for washout) is indicated in septic arthritis that cannot be adequately managed by aspiration alone, or where the joint is inaccessible to needle aspiration (particularly the hip in children). The indications for arthrotomy are: (1) septic arthritis of the hip in any age group (the hip is a deep, tight joint where needle aspiration is unlikely to achieve complete evacuation), (2) failure of clinical improvement after aspiration and antibiotics within 24-36 hours, (3) loculated (multicompartment) joint infection, and (4) any septic arthritis with systemic sepsis. Arthroscopic washout (using a camera and fluid-irrigation system) is an alternative to open arthrotomy for large accessible joints (knee, shoulder) with equivalent outcomes and smaller wounds.
Operative Source Control in Musculoskeletal Infection
Anatomical Principles of Surgical Access
Understanding the surgical anatomy is essential for the team-assist member: you must know which structures the surgeon is working near, anticipate the next step, and recognise if the approach is deviating from the expected trajectory. The anatomical principles governing access to infected bone and joints prioritise minimising neurovascular injury while achieving the best possible exposure of the infected focus.
For abscess drainage in the metaphysis of long bones: The approach is dictated by the location of the abscess (confirmed preoperatively on ultrasound/MRI) and the need to avoid the major neurovascular bundles of the limb. For distal femoral metaphysis abscesses, the standard approach is through the lateral or medial aspect of the distal thigh, avoiding the femoral vessels (anteromedial) and popliteal vessels (posterior). For proximal tibial metaphysis, the approach is anterolateral or anteromedial, avoiding the anterior tibial artery (posterolateral, in the anterior compartment, supplying the tibialis anterior) and the common peroneal nerve (wrapping around the neck of the fibula).
For sequestrectomy of long bone diaphysis: The approach targets the involucrum, which has been mapped preoperatively on CT. An incision is made over the thickest part of the involucrum (typically the lateral or anterolateral cortex of the tibia or femur, avoiding the posterior neurovascular bundle). The involucrum is opened using an osteotome or gouge to create a window, exposing the sequestrum lying within the medullary cavity. This window in the involucrum effectively becomes the saucerisation — converting a closed cavity into an open, irrigated cavity.
For arthrotomy of the hip: The standard approach in children is the anterolateral (Watson-Jones) or anterior (Smith-Petersen) approach. The surgical interval for the Smith-Petersen approach lies between sartorius (femoral nerve) and tensor fasciae latae (superior gluteal nerve). The anterior capsule is incised, pus is evacuated, and thorough saline lavage is performed. The lateral circumflex femoral artery and its branches must be ligated or cauterised. The femoral nerve and femoral artery lie medially and must be protected throughout.
For knee arthrotomy: The medial parapatellar or lateral parapatellar approach is used. The patella is reflected, the joint opened, pus evacuated, and copious washout performed. The popliteal vessels lie posteriorly and are not at risk with the standard anterior approach. The infrapatellar fat pad may be excised if grossly infected to facilitate washing.
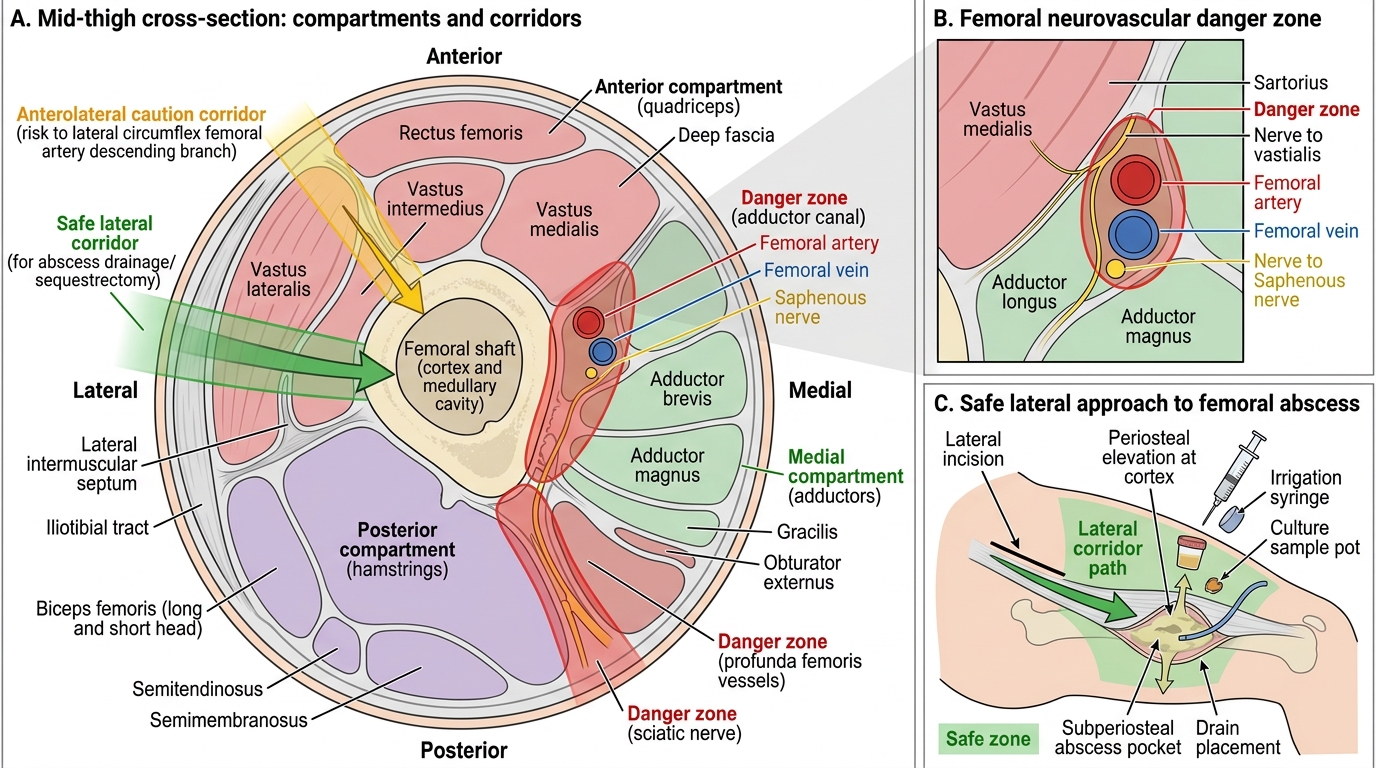
Mid-Thigh Safe Surgical Corridors for Infection Drainage
Operative Technique: Abscess Drainage
Drainage of a bone or soft-tissue abscess follows a sequence of steps that are common to all surgical drainage procedures, adapted to the specific anatomical location. The fundamental principle is: identify the abscess, enter it cleanly, evacuate all pus, debride non-viable tissue, irrigate copiously, and leave nothing behind that will perpetuate infection.
Step 1 — Incision planning. The incision is placed over the area of maximum fluctuance or directly over the subperiosteal collection as defined on MRI or ultrasound. The incision must be long enough to allow adequate access but placed along skin tension lines (Langer's lines) where possible to minimise scarring. In the distal femur, a lateral longitudinal incision is standard.
Step 2 — Dissection to the abscess. Soft-tissue planes are opened with a combination of sharp and blunt dissection. The subcutaneous fat, deep fascia, and muscle planes are divided in sequence. When the periosteum is reached (stripped and elevated by the subperiosteal pus), it is incised, and pus evacuates spontaneously under pressure.
Step 3 — Evacuation and sampling. Pus is first sampled in a sterile plain pot for culture and sensitivity (this is the definitive microbiological specimen — more reliable than the pre-operative aspirate). All pus is evacuated. Necrotic soft tissue (grey, non-bleeding, non-adherent) is debrided with sharp scissors or a curette.
Step 4 — Bone access (for intraosseous abscess). If the abscess lies within bone (intraosseous cavity), a small cortical window is drilled or chiselled to drain the cavity. Drilling provides immediate pressure relief and drainage of the medullary pus.
Step 5 — Copious irrigation. The cavity is washed with 1-3 litres of normal saline (or antibiotic-containing saline in the operating surgeon's preference). Irrigation removes residual bacteria, debris, and pro-inflammatory mediators.
Step 6 — Wound management. In early acute osteomyelitis, the wound may be closed over a drain. In established infection, the wound is left open (packed with saline-soaked gauze) to heal by secondary intention or granulation, because primary closure over a contaminated cavity risks re-accumulation. The decision is made by the operating surgeon based on the degree of contamination.
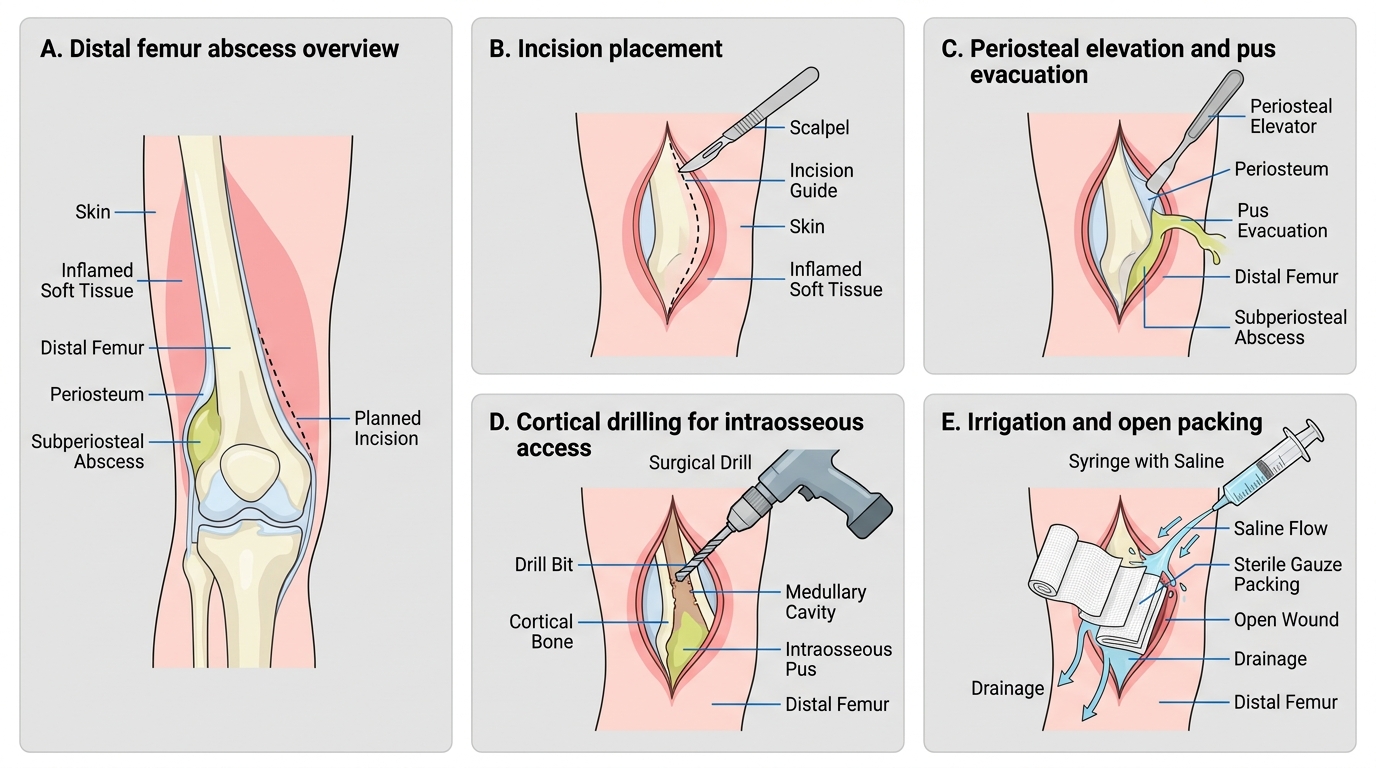
Distal Femur Abscess Drainage: Surgical Steps