Page 11 of 20
OR3.3 | Operative Source Control Assistance — SDL Guide (Part 2)
Operative Technique: Sequestrectomy and Saucerisation
Sequestrectomy and saucerisation are the definitive surgical procedures for chronic osteomyelitis. They must be performed together — removing the sequestrum without creating an adequate open cavity (saucerisation) leads to dead-space accumulation and re-infection; saucerisation without complete sequestrectomy leaves the bacterial nidus in place. The two procedures are therefore inseparable in concept and in practice.
Preoperative preparation for sequestrectomy requires: CT imaging to map the exact position, extent, and number of sequestra (there may be more than one fragment); preoperative culture of sinus tract discharge (though this is unreliable — intraoperative bone biopsy is more accurate); templating of bone defect size to plan dead-space management; and patient optimisation (nutritional status, diabetes control, smoking cessation) because compromised hosts have impaired wound healing.
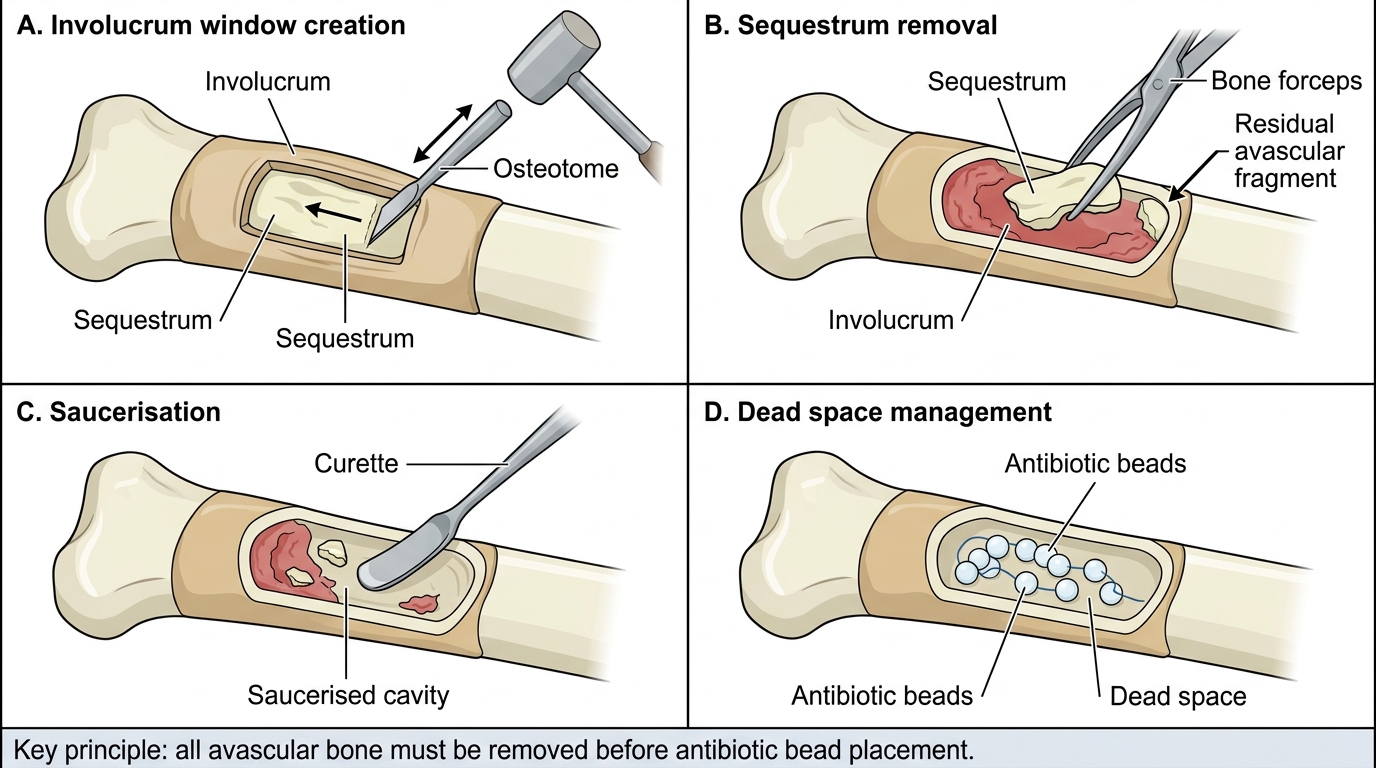
Step 1 — Approach and involucrum window. An incision is made over the involucrum, exposing the thickened periosteal new bone shell. Using an osteotome, bone nibbler (Kerrison rongeur), or an oscillating saw, a window is cut through the involucrum directly over the sequestrum. The window must be large enough to allow complete access — inadequate windows leave sequestrum fragments behind.
Step 2 — Sequestrum removal. The sequestrum is identified (pale, avascular, separated from the surrounding involucrum by a layer of granulation tissue and pus), grasped with bone-holding forceps, and removed in as few fragments as possible. Completeness is critical — even a 1-2 cm residual fragment of avascular bone will perpetuate infection. The cavity is explored with a curette to ensure all fragments are removed.
Step 3 — Saucerisation of the cavity. Using a curette, bone gouges, or a high-speed burr, the walls of the involucrum cavity are trimmed to create a smooth, gently concave (saucer-shaped) open cavity. Infected, sclerotic, poorly vascularised bone is removed; viable, bleeding bone is preserved. The goal is a cavity whose walls are composed of healthy, vascular bone that will support granulation tissue ingrowth.
Step 4 — Dead-space management. Options: (a) pack with antibiotic-impregnated PMMA beads (gentamicin or tobramycin) as a temporary spacer, then second-stage bone grafting; (b) immediate cancellous bone graft if the cavity is small and well debrided; (c) muscle flap transposition for large defects in the tibia where skin coverage is poor; (d) Ilizarov ring fixator for segmental bone loss with planned bone transport.
Step 5 — Wound closure. In a staged approach, the wound is left open after bead insertion and closed at the second stage. After bone grafting, a drain is placed and the wound closed in layers.
Sequestrectomy and Saucerisation in Chronic Osteomyelitis
SELF-CHECK
During sequestrectomy, the surgeon removes what appears to be the sequestrum but the scrub nurse notes a small pale fragment still visible at the cavity's edge. What is the correct action?
A. Close the wound over a drain — the remaining fragment will be absorbed by the body
B. Irrigate with antibiotic solution and close — residual fragments are acceptable if small
C. Remove the residual fragment completely — any avascular bone left behind perpetuates infection and will cause recurrence
D. Pack with gentamicin beads over the residual fragment — this will sterilise it in situ
Reveal Answer
Answer: C. Remove the residual fragment completely — any avascular bone left behind perpetuates infection and will cause recurrence
Completeness of sequestrum removal is the single most critical determinant of outcome in sequestrectomy. Even a small avascular bone fragment is inaccessible to antibiotics and will act as a continued bacterial nidus, causing recurrence. The surgeon must explore the entire cavity with a curette to confirm no fragments remain. Antibiotic beads manage dead space but cannot sterilise avascular bone.
Operative Technique: Arthrotomy and Joint Washout
Provided image
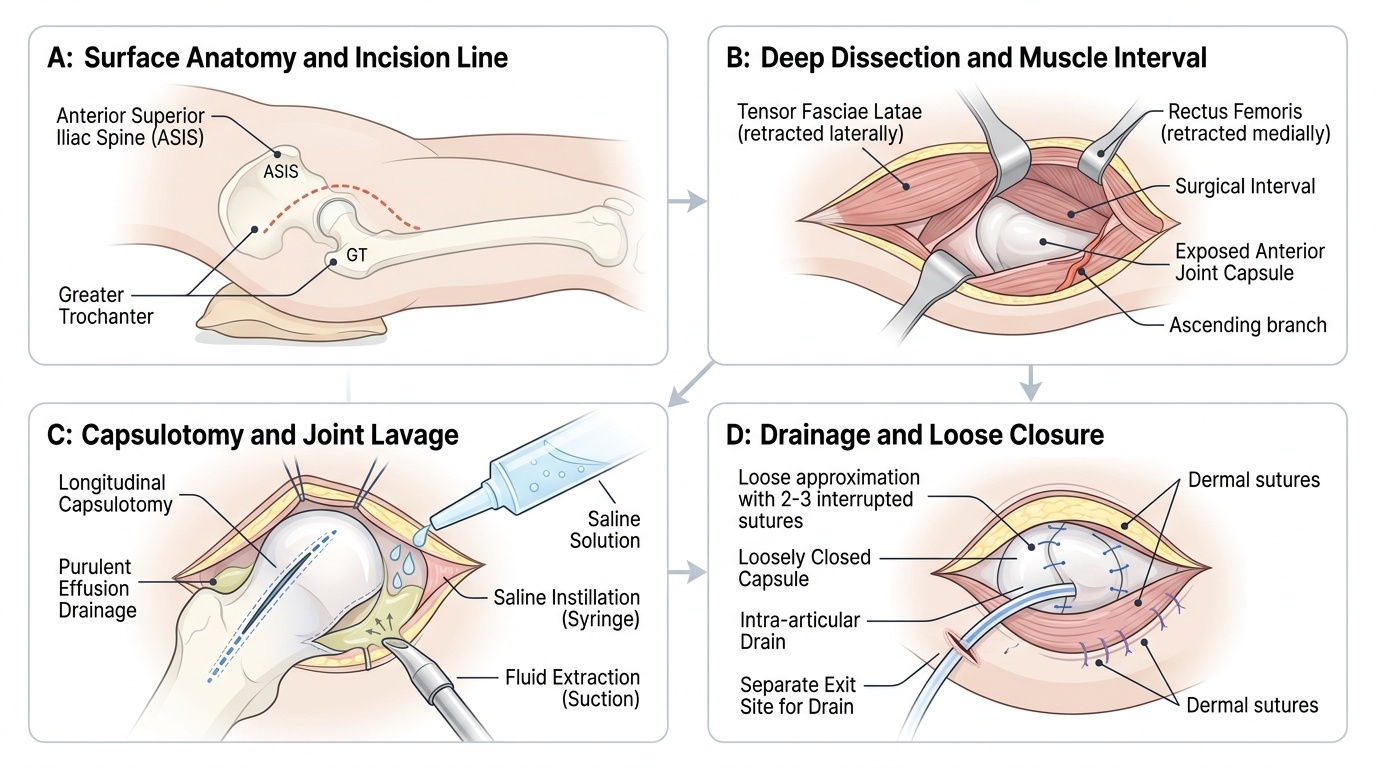
Arthrotomy for septic arthritis is performed as an emergency or urgent procedure because delay directly correlates with joint destruction and, in the hip, with avascular necrosis. The objectives of arthrotomy are: evacuate all pus, debride necrotic synovium and fibrin, achieve copious joint lavage, and allow the joint to decompress postoperatively via a drain.
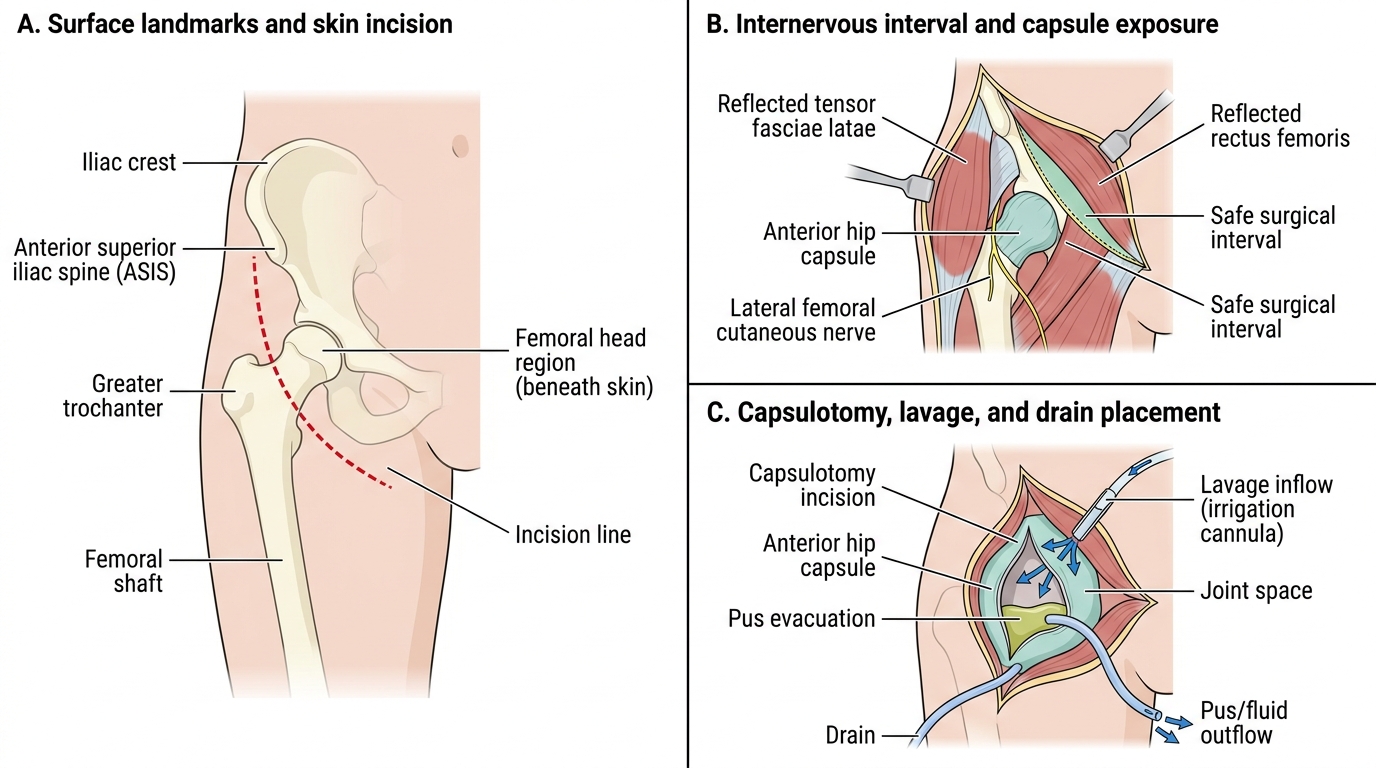
Hip arthrotomy (anterolateral approach in children): With the patient supine and a sandbag under the ipsilateral hip, the incision is made from just anterior to the greater trochanter toward the anterior superior iliac spine. Tensor fasciae latae is reflected, the fascia of the rectus femoris is opened, and the anterior hip capsule is exposed. The capsule is incised longitudinally and the pus evacuated. The volume and character of pus are noted (frank pus vs turbid fluid). The joint is washed with 2-3 litres of normal saline, using a syringe and suction alternately to flush all recesses of the joint. The capsule is closed loosely (or left open in severe cases) and a drain inserted.
Knee arthrotomy (medial parapatellar approach): With the patient supine, the incision runs from 3-5 cm above the superolateral pole of the patella, around the medial border of the patella, and 2-3 cm below the tibial tubercle. The patella is everted (flipped laterally), exposing the entire joint. Pus is evacuated, fibrinous deposits and necrotic synovium are debrided, and the joint is washed with 3-5 litres of saline. A drain is placed intra-articularly and the wound closed in layers. The knee is splinted in extension postoperatively.
Arthroscopic washout (knee and shoulder): Using two portals and a continuous saline inflow-outflow system, the joint is inspected with a 4mm arthroscope. Pus and fibrin are lavaged, infected synovium debrided, and loculations broken down. Arthroscopic washout is as effective as open arthrotomy for uncomplicated septic arthritis of the knee and shoulder, with the advantage of smaller wounds and faster recovery. It is NOT suitable for the hip in children (too small) or for severely infected joints with thick fibrinous deposits that require direct manual removal.
Postoperative care: The drain is removed when output is minimal (typically 24-48 hours). The limb is elevated to reduce oedema. IV antibiotics are continued until clinical and laboratory improvement (CRP falling), then switched to oral for 3-6 weeks total. Passive range-of-motion exercises begin as soon as pain allows to prevent adhesion formation; active physiotherapy follows.
Anterolateral Hip Arthrotomy for Septic Arthritis
Intraoperative Findings: Interpretation and Documentation
The ability to interpret intraoperative findings is a core component of operative competence that distinguishes a knowledgeable team member from a passive bystander. In operative source control for musculoskeletal infection, the surgeon and the team must assess the nature of the infected tissue at the time of surgery, because these findings directly modify the operative plan and determine subsequent management. Documenting these findings accurately in the operative note is a mandatory medico-legal and clinical responsibility.
Pus characteristics and what they indicate: When the abscess or joint is opened, the character of the pus provides immediate diagnostic information. Frankly purulent, thick, creamy, yellow pus suggests acute staphylococcal infection (S. aureus). Thin, watery, odourless fluid may suggest a less virulent organism or early infection. Foul-smelling, dark pus with gas suggests anaerobic infection (rare in bone but occurs in diabetics and crush injuries). Caseous, cheese-like, pale material is pathognomonic of tuberculosis — if this is found unexpectedly in a patient being operated for assumed pyogenic infection, the procedure shifts immediately: collect tissue for ZN stain, histopathology, and TB culture; obtain a Heaf/Mantoux history; and involve a physician.
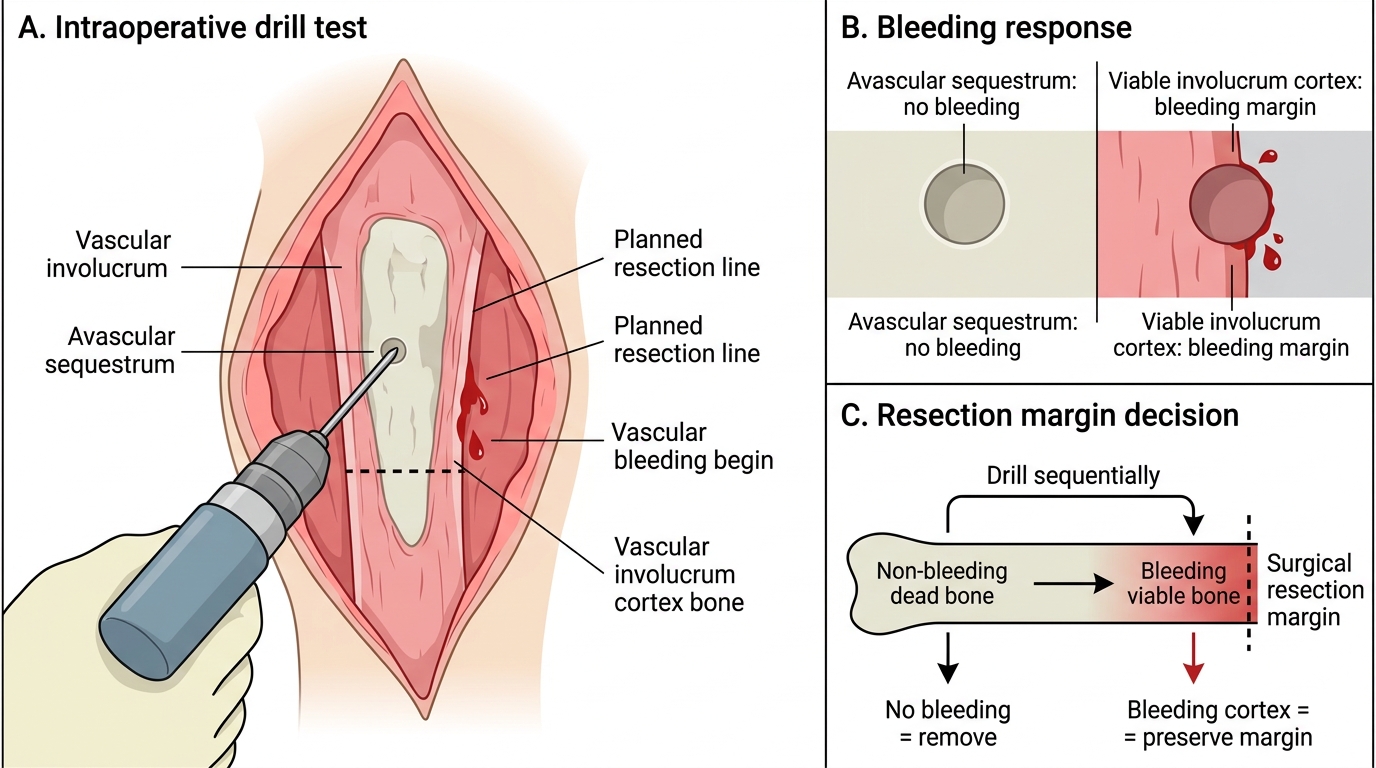
Sequestrum characteristics: The sequestrum appears pale or white (in contrast to the pink-red of living bone), does not bleed when drilled with a Kirschner wire (the "drill test" — living bone bleeds, avascular bone does not), and is often surrounded by a layer of granulation tissue and pus. The boundary between sequestrum and viable involucrum must be identified precisely. Viable bone bleeds freely; sclerotic but potentially vascular bone may bleed after the first millimetre is drilled. The surgeon uses both visual appearance and the drill test to define the resection margin.
Joint appearances in septic arthritis: On entering a septic joint, the surgeon assesses: (1) pus volume (document in mL), (2) joint lining (hypertrophied, haemorrhagic, or friable synovium indicates more severe infection), (3) articular cartilage surface (intact, fibrillated, or denuded — cartilage loss is irreversible and predicts secondary osteoarthritis), and (4) fibrin deposits (thick loculated fibrin requires manual removal with forceps, not just irrigation). A joint with denuded cartilage at the time of surgery carries a poor functional prognosis and the family must be counselled accordingly postoperatively.
Specimen documentation: Every operative specimen must be logged with: specimen type (pus aspirate, bone biopsy, synovial tissue), anatomical site, volume or size, and appearance. The request form must note the clinical diagnosis, antibiotics already given, and the suspected organism to guide laboratory prioritisation.
Drill Test for Sequestrum Resection Margin