Page 1 of 10
OR4.1 | Skeletal Tuberculosis of Major Joints and Spine — SDL Guide
Learning Objectives
- Describe the clinical features of skeletal tuberculosis affecting the hip, knee, and spine, distinguishing it from pyogenic infection
- Explain the pathogenesis of cold abscess formation and gibbus deformity in Pott's disease
- Outline the radiological and laboratory investigations used to diagnose skeletal TB
- Apply the principles of anti-tuberculosis therapy (ATT) and identify the indications for surgical intervention in skeletal TB
- Recognise Pott's paraplegia and describe its management principles
INSTRUCTIONS
Skeletal tuberculosis accounts for approximately 1–3% of all TB cases and is the most common cause of infectious arthritis in India and other high-burden countries. As a final-year MBBS student you will encounter patients who present with insidious joint pain, a draining sinus, or progressive spinal deformity — all potentially due to TB. Early recognition protects the patient from catastrophic complications such as spinal cord compression and permanent joint destruction. This module will equip you to differentiate skeletal TB from pyogenic bone and joint infection, interpret the relevant investigations, initiate anti-tuberculosis therapy, and counsel patients on the need for specialist referral.
References
- Maheshwari's Essential Orthopaedics, 6th ed., Ch 28 (Tuberculosis of Bones and Joints) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 2 (Infection) (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed., Ch 10 (Skeletal Tuberculosis) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old agricultural worker presents with a 6-month history of gradually worsening low back pain and stiffness, with no history of trauma. Over the last 3 weeks he has developed mild weakness in both lower limbs and difficulty walking. On examination, there is localised tenderness at the thoracolumbar junction and a subtle gibbus deformity. His ESR is 95 mm/h and he has a past history of pulmonary tuberculosis 4 years ago. What is the most likely diagnosis, and what is the next critical step to prevent permanent neurological disability? This patient's presentation captures the insidious but devastating tempo of Pott's disease — spinal tuberculosis — the most common form of skeletal TB in India. His story is your entry point into one of orthopaedics' most important differential diagnoses.
WHY THIS MATTERS
India carries the world's highest burden of tuberculosis, and skeletal TB follows pulmonary and lymph node TB as the third most common extrapulmonary site. The spine is the most frequently affected skeletal site, followed by the hip and knee. Because skeletal TB progresses slowly over months to years, patients often present late — after significant bone destruction, abscess formation, or neurological compromise has already occurred. A missed or delayed diagnosis can result in permanent paraplegia, hip joint ankylosis, or lifelong disability. As a final-year student you will be examined on distinguishing skeletal TB from pyogenic osteomyelitis and septic arthritis, and you must know the anti-tuberculosis regimen and its surgical adjuncts.
RECALL
Before proceeding, recall the following from your Year 1 and Year 2 studies:
Microbiology: Mycobacterium tuberculosis is an acid-fast bacillus (AFB) with an obligate aerobic intracellular lifestyle. It spreads haematogenously from a primary lung focus; a dormant focus can reactivate decades later.
Pathology: Granulomatous inflammation (epithelioid macrophages, Langhans giant cells, lymphocytes) with central caseous necrosis is the hallmark of TB pathology. Caseous material liquefies under proteolytic enzymes and can track along tissue planes.
Pharmacology basics: The four first-line anti-tuberculosis drugs are isoniazid (H), rifampicin (R), pyrazinamide (Z), and ethambutol (E). The standard regimen for drug-sensitive TB is 6 months (intensive phase 2 months + continuation phase 4 months). Recall these before you engage with the management section.
Clinical Presentation — Skeletal Tuberculosis
Skeletal tuberculosis typically presents in a young adult (second to fourth decade) or child with a history of prolonged, insidious-onset musculoskeletal pain, swelling, and progressive limitation of movement. The cardinal distinguishing feature from pyogenic infection is the indolent tempo: symptoms evolve over months to years rather than days to weeks. Systemic constitutional features — evening rise in temperature, night sweats, weight loss, anorexia, and malaise — are variably present and reflect the underlying mycobacterial disease burden. In children, a limp or reluctance to use a limb may be the first sign. This indolent tempo — symptoms evolving over months rather than days — is the single most important clinical clue that separates skeletal tuberculosis from acute pyogenic bone and joint infections, which present with rapid onset of local heat, erythema, and severe systemic toxicity.
Constitutional features suggestive of TB:
- Prolonged low-grade fever, characteristically in the evenings
- Night sweats and weight loss over weeks to months
- Anorexia and general malaise
- History of close contact with a known TB case, or personal history of prior TB
At the affected joint or spinal level, the patient describes a dull, aching, deep-seated pain that worsens with weight-bearing or movement and is partially relieved by rest. In contrast to septic arthritis or acute osteomyelitis, the local skin is not warm, erythematous, or acutely tender — signs that would indicate a pyogenic process. The joint may be diffusely swollen with synovial thickening palpable as a doughy consistency. Eventually a cold abscess forms — a fluctuant, non-tender, non-erythematous swelling produced by liquefied caseous pus that has tracked away from the primary focus. The skin over a cold abscess is normal in colour and temperature, hence the term "cold." If neglected, the abscess may discharge spontaneously, forming a sinus that becomes colonised with secondary organisms.
In spinal TB (Pott's disease), the presenting symptoms are back pain at the affected level, local tenderness on percussion over the spinous processes, and progressive rigidity (muscle spasm-driven protective posturing). A visible or palpable angular deformity (gibbus) may be present at advanced stages.
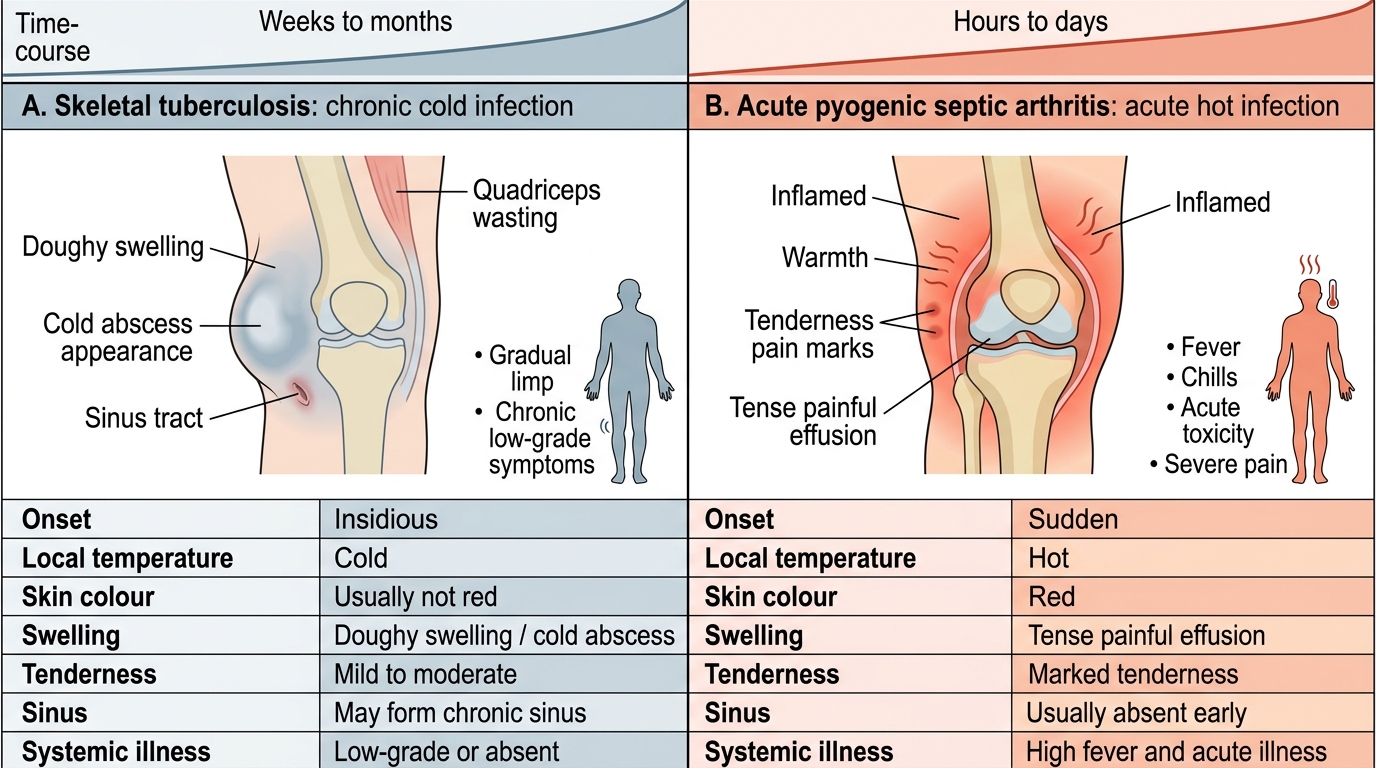
Skeletal Tuberculosis vs Acute Pyogenic Septic Arthritis
Psoas Abscess in Skeletal Tuberculosis
Site-specific presentations:
Hip TB presents with insidious hip pain, a limp (antalgic gait), and progressive loss of hip motion. The earliest movement to be lost is abduction and internal rotation. Late-stage disease produces a characteristic flexion-adduction-internal rotation deformity of the hip, and in neglected cases the joint surfaces are destroyed, leading to fibrous or bony ankylosis.
Knee TB presents with synovial thickening and effusion giving a diffusely swollen "doughy" knee. Wasting of the quadriceps is prominent even early in the disease (Spindle-shaped thigh). Pain and restriction of flexion and extension are progressive.
Spine TB (Pott's disease) classically begins in the anterior part of the vertebral body near its superior or inferior end-plate, because this area has the richest blood supply. The infection spreads beneath the anterior longitudinal ligament to involve adjacent vertebrae, resulting in anterior wedge collapse and ultimately the characteristic kyphotic angular deformity known as a gibbus.
Pathology and Mechanism of Skeletal Tuberculosis
Understanding the pathogenesis of skeletal tuberculosis explains the clinical features, radiological appearances, and complications seen in this disease. Mycobacterium tuberculosis reaches the skeleton almost exclusively by haematogenous spread from a primary pulmonary focus or from reactivation of a dormant metastatic focus seeded during primary bacteraemia. The bones are seeded during episodes of mycobacteraemia, with bacilli lodging preferentially in regions of rich vascularity — the cancellous bone of the epiphysis and metaphysis in long bones, the vertebral body end-plates in the spine, and the synovial membrane of joints.
Granuloma formation and caseous necrosis: The hallmark of TB pathology at any site is the formation of granulomas — discrete collections of epithelioid macrophages and Langhans' giant cells, surrounded by lymphocytes and fibroblasts, with a central zone of caseous necrosis. In bone, this process is accompanied by progressive resorption of the surrounding trabeculae (TB does NOT produce reactive new bone formation, unlike pyogenic osteomyelitis), leading to the radiological appearance of bone rarefaction and eventual lytic destruction.
The caseous necrotic material is initially solid but, under the influence of proteolytic enzymes liberated by macrophages, it liquefies to form pus. Because the surrounding tissue reaction is granulomatous rather than acute suppurative, this pus lacks the heat, redness, and exquisite tenderness of a pyogenic abscess — hence the designation cold abscess. Liquefied caseous material spreads along paths of least resistance: beneath fascial planes, along muscle sheaths, and eventually to the skin surface where it may discharge as a sinus tract.
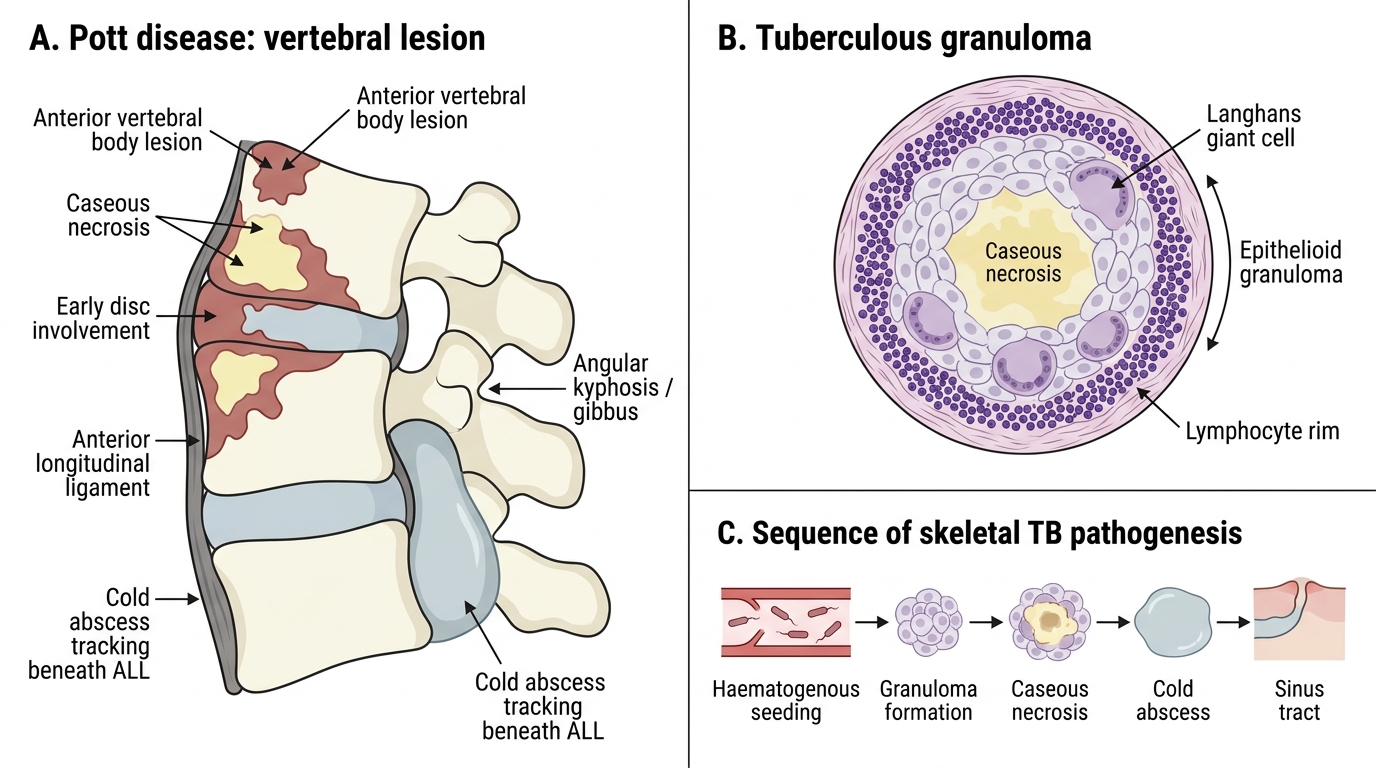
Tuberculous Vertebral Lesion in Pott Disease
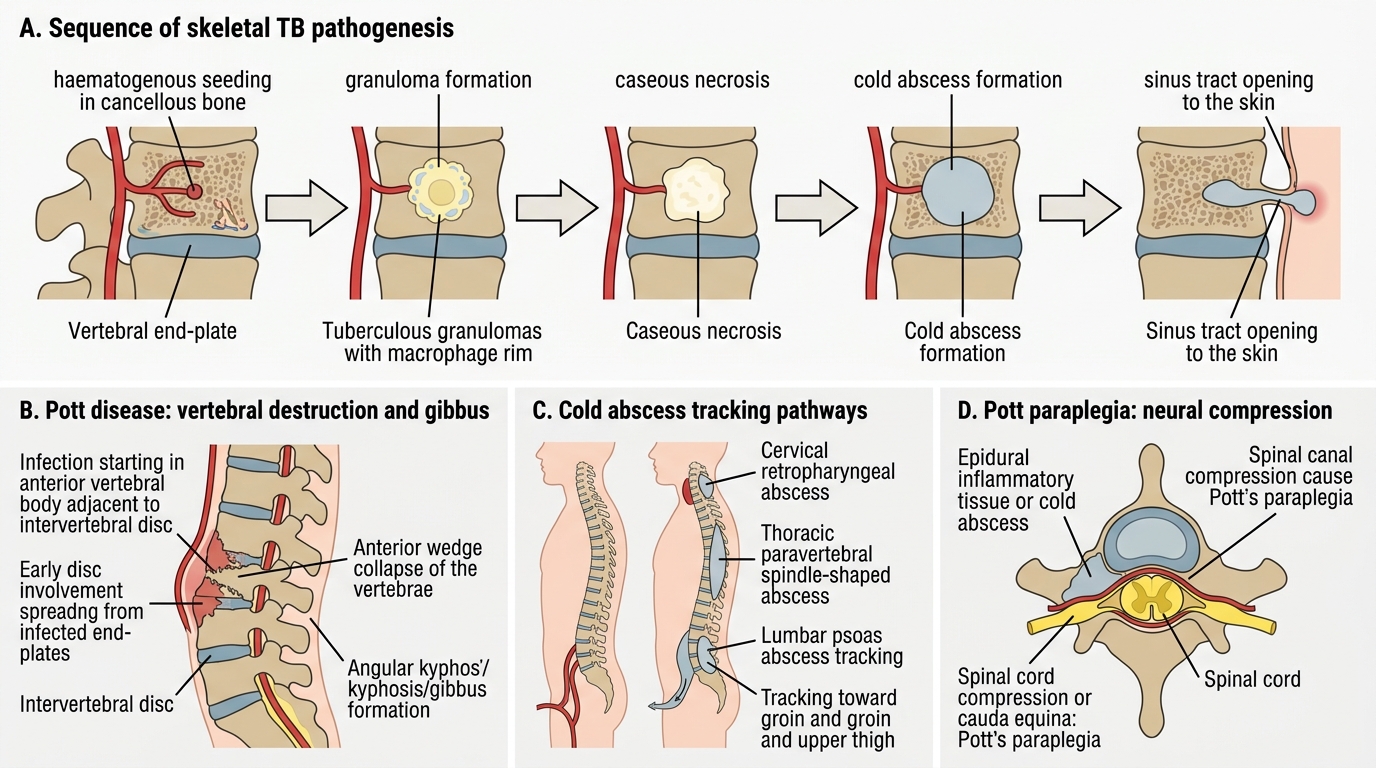
Pathogenesis and Spinal Spread of Skeletal Tuberculosis
Spinal pathology in Pott's disease: Infection typically begins in the anterior part of the vertebral body, adjacent to the disc. Disc involvement occurs early because the avascular disc is invaded from adjacent infected vertebral end-plates — this is distinct from pyogenic discitis, which also destroys the disc, but distinguishable by tempo and organism. As infection spreads, anterior vertebral body substance is destroyed and the normal anterior height is lost, producing anterior wedge collapse. When two or more adjacent vertebrae are involved, the resulting kyphotic deformity is sharply angular (a gibbus), in contrast to the smooth, gradual kyphosis of degenerative disease.
The cold abscess in spinal TB tracks within predictable anatomical pathways:
- Cervical spine: retropharyngeal abscess (present as dysphagia or dyspnoea)
- Thoracic spine: paravertebral abscess forming a fusiform "spindle" shadow on X-ray; may track to intercostal spaces or posteriorly
- Lumbar spine: abscess tracks into the psoas sheath (psoas abscess), may present in the groin, upper thigh, or even below the inguinal ligament
Neurological complications — Pott's paraplegia: Perhaps the most feared complication, Pott's paraplegia refers to spinal cord or cauda equina compression in the context of spinal TB. It may occur by two mechanisms:
1. "Active" (early): Mechanical compression by epidural cold abscess, caseous granulation tissue, or sequestrum directly compressing the cord or its blood supply. This is potentially reversible with adequate ATT or surgical decompression.
2. "Healed/Late" (inactive): Bony compression by sequestra, internal gibbus (bony ridge projecting into the canal), or fibrous tissue after healing. This is less responsive to medical therapy and often requires surgical decompression.
For hip and knee TB, the joint pathology progresses through stages described by Girdlestone:
- Stage 1 (Synovitis): Synovial membrane is inflamed and thickened; joint space is relatively preserved; bone is not yet involved
- Stage 2 (Early arthritis): Marginal erosions appear; periarticular osteoporosis on X-ray
- Stage 3 (Advanced arthritis): Significant cartilage and bone destruction; subluxation may occur
- Stage 4 (Healing/Ankylosis): Fibrous or bony ankylosis following disease arrest or treatment
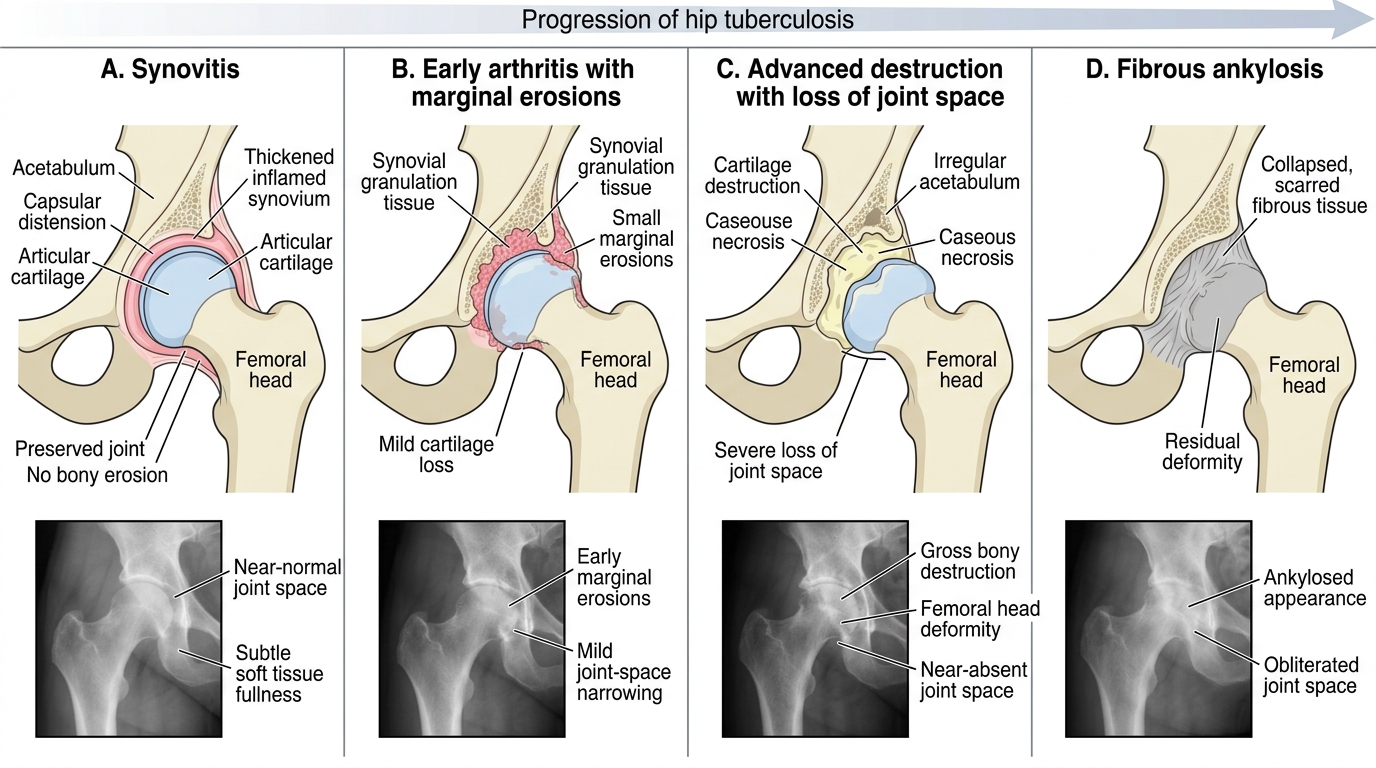
Girdlestone Stages of Tuberculosis of the Hip
SELF-CHECK
A 30-year-old man has a swelling in the right groin that is fluctuant, non-tender, and the overlying skin is normal in colour and temperature. X-ray of the lumbar spine shows anterior wedge collapse at L2-L3 with disc space narrowing. What is the swelling, and what is the mechanism by which it reached the groin?
A. Inguinal hernia — bowel herniation through the deep inguinal ring
B. Psoas abscess from lumbar spinal TB — caseous pus tracking along the psoas sheath
C. Septic arthritis of the hip — haematogenous spread with abscess formation in the joint capsule
D. Femoral hernia — peritoneal contents herniating through the femoral canal
Reveal Answer
Answer: B. Psoas abscess from lumbar spinal TB — caseous pus tracking along the psoas sheath
This is a psoas abscess, the classic presentation of cold abscess from lumbar spinal tuberculosis. Caseous pus formed by liquefaction of the granulomatous exudate at the L2-L3 level tracks inferiorly along the fascial sheath of the psoas major muscle, which runs from the lumbar transverse processes to the lesser trochanter of the femur. The abscess is 'cold' — no local heat or erythema — because the tissue reaction is granulomatous, not acute suppurative. It is non-tender because there is no acute inflammatory mediator release. The L2-L3 vertebral wedging and disc narrowing confirm the source.
Examination and Investigations in Skeletal Tuberculosis
A systematic clinical examination combined with targeted investigations is required to confirm the diagnosis of skeletal tuberculosis, determine the extent of disease, and exclude pyogenic infection as the cause. The clinical assessment begins with a thorough general examination looking for systemic signs of tuberculosis — constitutional features, lymphadenopathy, and evidence of pulmonary disease — before focusing on the affected musculoskeletal region. The examination must be methodical because skeletal TB presents with subtle signs that evolve slowly over months, and the absence of acute inflammatory signs (warmth, redness, extreme tenderness) is itself diagnostically important. A targeted neurological assessment is mandatory in all cases of spinal TB to document any motor, sensory, or reflex deficits that would indicate cord or cauda equina involvement.
Clinical examination:
General examination may reveal evidence of constitutional TB: cachexia, anaemia, low-grade fever. Axillary or cervical lymphadenopathy and pulmonary signs may be present. At the affected joint:
- Spinal TB: Inspect for gibbus deformity (angular kyphosis) and paravertebral muscle spasm. Palpate for spinous process tenderness. Perform a Psoas test (hip extension with patient prone increases lumbar pain in paravertebral abscess). Assess lower limb neurology — motor power (Medical Research Council grading), sensation, and reflexes — to document cord/cauda involvement.
- Hip TB: Observe gait (antalgic limp). Measure range of motion — Thomas test reveals a fixed flexion deformity; abduction and internal rotation are reduced earliest. Late disease: the flexion-adduction-internal rotation deformity pattern is pathognomonic.
- Knee TB: Effusion (fluctuation, patellar tap), synovial thickening (doughy feel), quadriceps wasting, and restricted range of motion. A limb in apparent normal position but with restricted end-range flexion is typical early.
Laboratory investigations:
- ESR and CRP: Elevated but non-specific. ESR often in the range 60–120 mm/h. Useful for monitoring treatment response.
- Mantoux test (TST): Induration ≥10 mm at 48–72 hours is positive in immunocompetent patients. A negative result does NOT exclude TB (anergy in malnutrition/HIV). Not diagnostic but supportive.
- Complete blood count: Lymphocytosis; anaemia of chronic disease; normal or mildly elevated WBC (in contrast to pyogenic infection where leukocytosis is marked).
- Serum proteins: Hypoalbuminaemia in chronic disease.
Microbiological confirmation:
- Aspiration of abscess/joint fluid: The most important bedside procedure. Aspirated material should be sent for:
- AFB smear (Ziehl-Neelsen stain): Rapid, cheap, but low sensitivity (20–40%) in skeletal TB due to paucibacillary nature.
- Mycobacterial culture (Löwenstein-Jensen medium): Gold standard for diagnosis and drug sensitivity; takes 6–8 weeks.
- CBNAAT/GeneXpert MTB/RIF: Rapid molecular test (result in 2 hours); detects M. tuberculosis DNA and rifampicin resistance simultaneously; preferred in high-burden settings for early confirmation.
- Histopathology: Biopsy of synovium or bone showing caseating granulomas with AFB is diagnostic.
- Interferon-Gamma Release Assay (IGRA): ELISA-based test on blood (QuantiFERON-TB Gold). More specific than Mantoux in BCG-vaccinated individuals; does not distinguish active from latent TB.
Imaging:
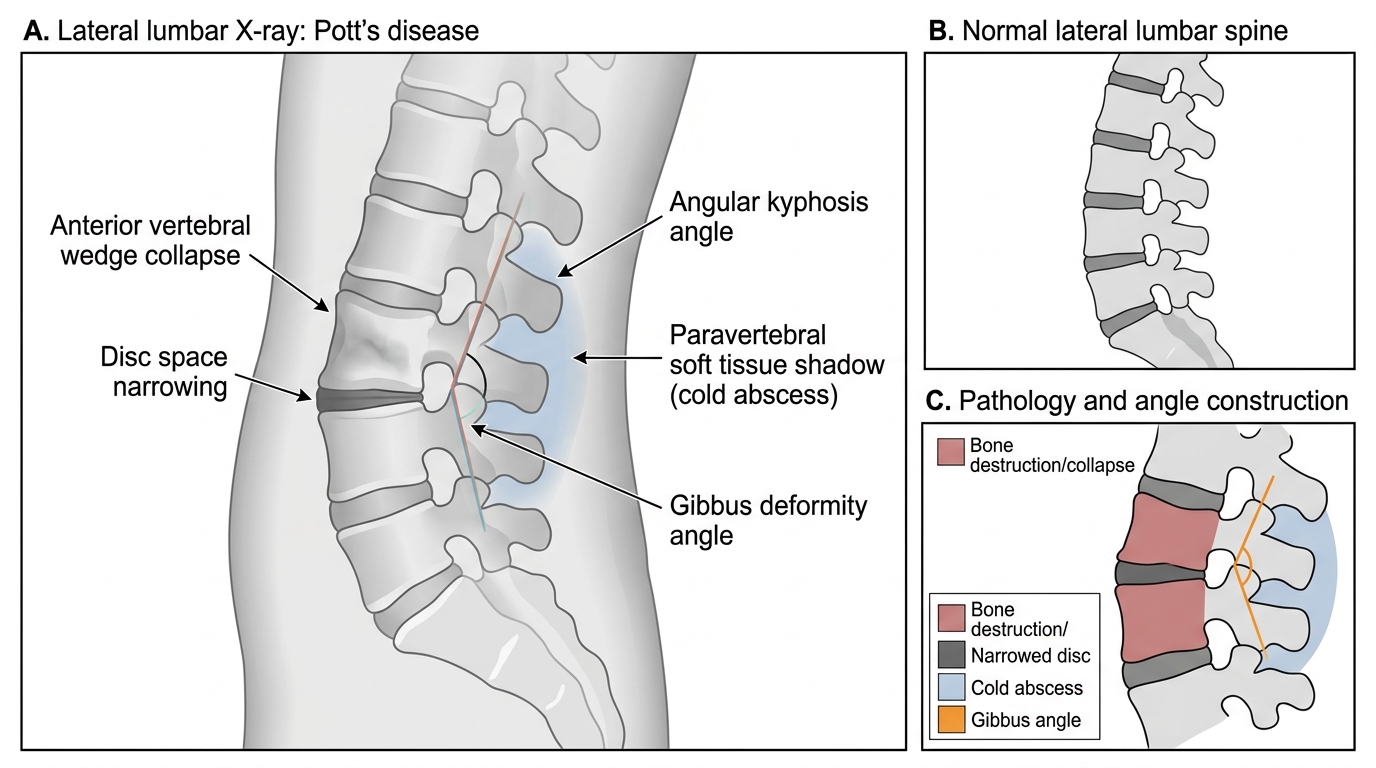
Lateral Lumbar X-ray Findings in Pott's Disease
Plain X-ray: Bone changes are late — at least 30–50% of bone mineral must be lost before plain X-ray shows lytic changes. Classic findings are:
- Disc space narrowing (early) — TB destroys the avascular disc from adjacent infected end-plates
- Anterior wedge collapse of one or more vertebral bodies (later)
- Paravertebral soft tissue shadow — fusiform, bilateral in thoracic, unilateral in lumbar (psoas abscess)
- Gibbus (angular kyphosis) on lateral view
- In joints: periarticular osteoporosis, marginal erosions ("rat-bite" appearance), eventual joint space obliteration
- Relative preservation of the disc early is seen in purely intraosseous lesions before disc invasion
MRI spine (investigation of choice for spinal TB): MRI detects early marrow changes, disc involvement, epidural cold abscess, and extent of cord compression far earlier than plain X-ray or CT. Characteristic features: hypointense vertebral body on T1, hyperintense on T2/STIR sequences; disc involvement; epidural soft tissue compressing the dural sac. Essential for surgical planning.
CT scan: Excellent for bone detail — shows sequestra, extent of vertebral destruction, and guides CT-guided needle aspiration of deep paraspinal abscesses.
Ultrasound: Identifies and guides aspiration of a psoas abscess or superficial joint effusion.
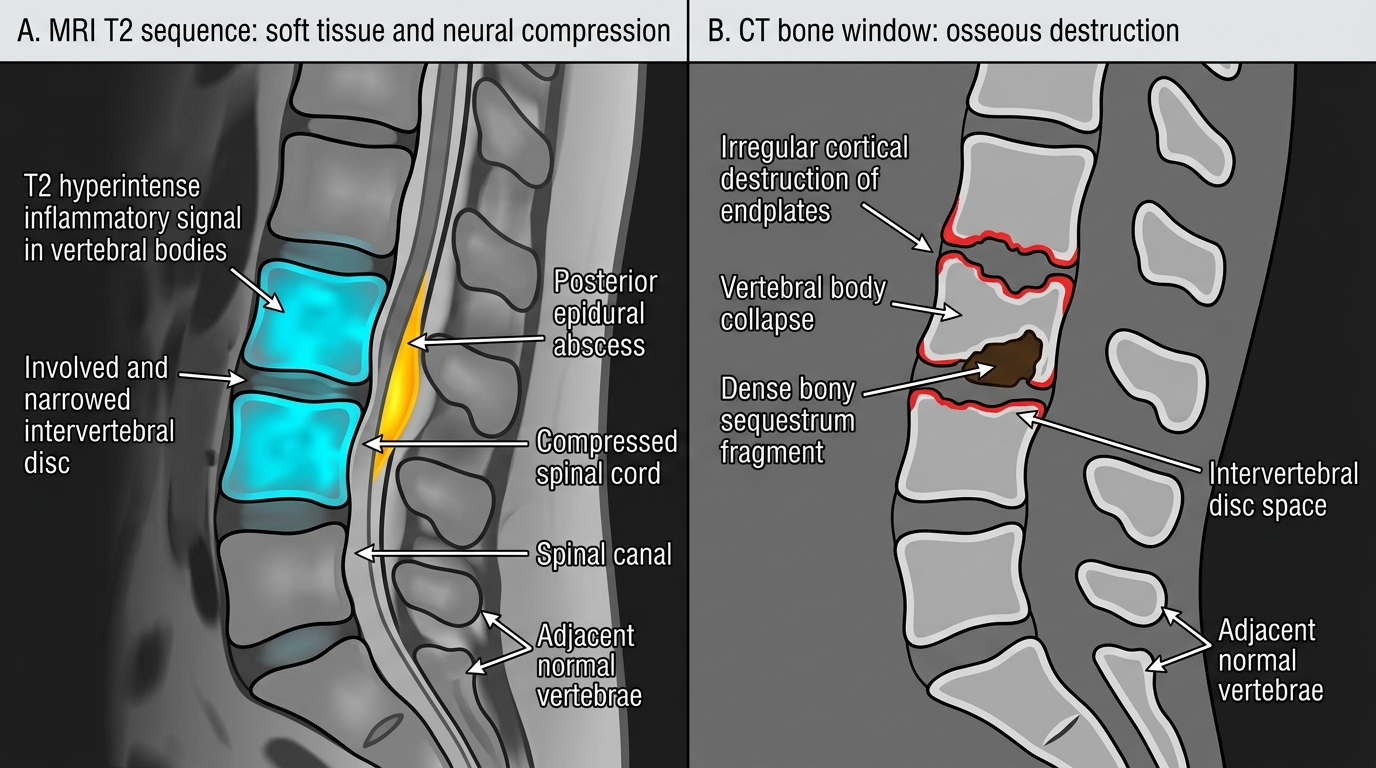
MRI versus CT Features of Pott's Disease