Page 2 of 10
OR4.1 | Skeletal Tuberculosis of Major Joints and Spine — SDL Guide (Part 2)
Management of Skeletal Tuberculosis
Management of skeletal tuberculosis requires a coordinated approach combining pharmacological treatment with anti-tuberculosis drugs, orthopaedic and protective measures, nutritional support, and surgical intervention when indicated. The cornerstone of treatment — and the single most important intervention for the vast majority of patients — is a complete course of anti-tuberculosis therapy (ATT). Most patients with uncomplicated skeletal TB, including hip, knee, and spinal disease without neurological deficit, respond satisfactorily to medical therapy alone if treatment is started early and completed without interruption. The response to ATT is characterised by gradual resolution of constitutional symptoms, reduction of local swelling, decreasing ESR, and eventual consolidation of destroyed bone on imaging. Surgical intervention is reserved for specific, well-defined indications and is always an adjunct to ATT, never a replacement.
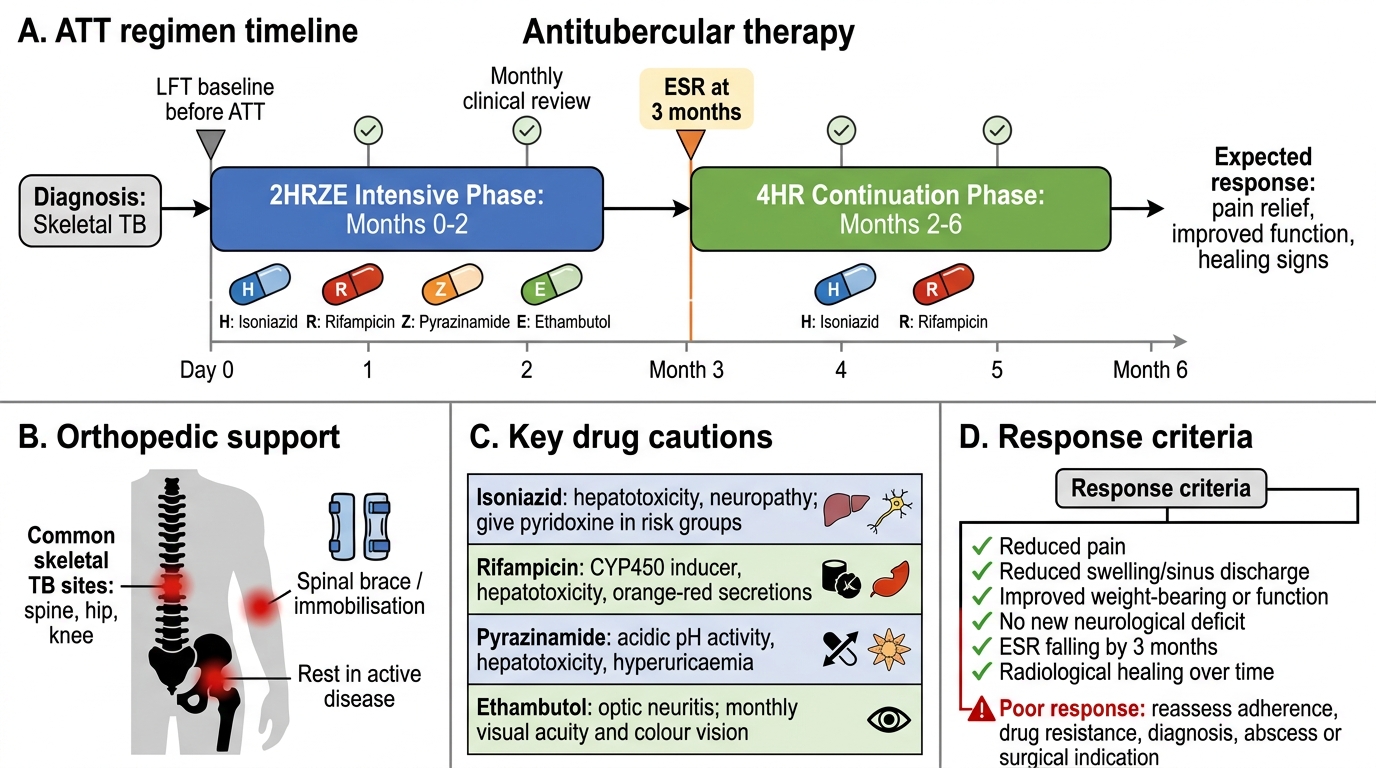
Anti-Tuberculosis Therapy (ATT) is the cornerstone of treatment for all forms of skeletal TB. The standard regimen for drug-sensitive pulmonary and extrapulmonary TB in India follows the RNTCP/National TB Elimination Programme (NTEP) guidelines:
- Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) — abbreviated 2HRZE
- Continuation phase (4 months): Isoniazid (H) + Rifampicin (R) — abbreviated 4HR
- Total duration: 6 months for most forms of extrapulmonary TB including peripheral joint TB
- Extended duration for spinal TB: Current NTEP guidelines recommend a minimum of 6 months (some centres and published guidance use 9–12 months for complicated spinal TB with neurological deficit or large abscess); follow local/institutional protocol
ATT Regimen and Monitoring in Skeletal Tuberculosis
Important pharmacological notes:
- Isoniazid — bactericidal; hepatotoxic; peripheral neuropathy (supplemented with pyridoxine/B6 in malnourished and pregnant patients)
- Rifampicin — bactericidal; powerful inducer of cytochrome P450 (drug interactions); hepatotoxic; colours urine/secretions orange-red
- Pyrazinamide — bactericidal in acidic pH; hepatotoxic; hyperuricaemia (caution in gout)
- Ethambutol — bacteriostatic; optic neuritis (check visual acuity/colour vision monthly; dose-adjusted in renal impairment)
Supportive and orthopedic measures:
- Rest and immobilisation: Reducing mechanical stress on the diseased segment prevents progressive deformity and is especially important in weight-bearing areas. The spine is protected with a spinal brace (thoracolumbar orthosis) during the active phase; hip disease may require a Thomas splint or hip spica in children. Bed rest is indicated during the active phase of disease in spinal TB with neurological deficit.
- Nutritional rehabilitation: Protein-calorie malnutrition is virtually universal in these patients; high-protein diet and correction of micronutrient deficiencies support healing and ATT tolerability.
Surgical indications in skeletal TB:
While most cases of skeletal TB respond to ATT alone, surgery is indicated in specific situations:
1. Diagnostic uncertainty — when aspiration or needle biopsy is non-diagnostic and tissue is needed for histopathology and culture
2. Large cold abscess causing symptoms — surgical drainage or aspiration (ATT alone will resorb small abscesses; large or expanding ones need evacuation)
3. Neurological deficit (Pott's paraplegia) — decompression and stabilisation are required when there is progressive neurological deficit or failure to improve on ATT; posterior laminectomy alone is INADEQUATE (removes the posterior tension band while the anterior pathology is untouched); anterior debridement and decompression with strut graft and fusion is the preferred approach
4. Spinal instability — gross vertebral collapse with kyphosis causing mechanical instability; needs spinal fusion (anterior, posterior, or combined depending on extent)
5. Joint destruction with functional disability — once disease is quiescent (confirmed by ATT, ESR normalisation, and 3–6 months of stable imaging), reconstructive surgery may be considered: arthrodesis (fusion) for painful ankylosis in a poor position; total joint replacement (arthroplasty) for selected patients with arrested disease and significant functional impairment (must be performed only after disease is declared quiescent)
6. Sinus tract — sinuses that fail to heal with ATT (secondary infection, retained sequestrum) require surgical exploration
Outcome monitoring:
- Clinical improvement (pain, fever, constitutional symptoms) typically begins within 4–6 weeks of starting ATT
- ESR should fall progressively; a rising ESR suggests drug resistance or non-compliance
- Serial imaging (X-ray ± MRI) at 3 and 6 months
- Drug-sensitive TB has a cure rate of >95% when treated with complete, uninterrupted ATT
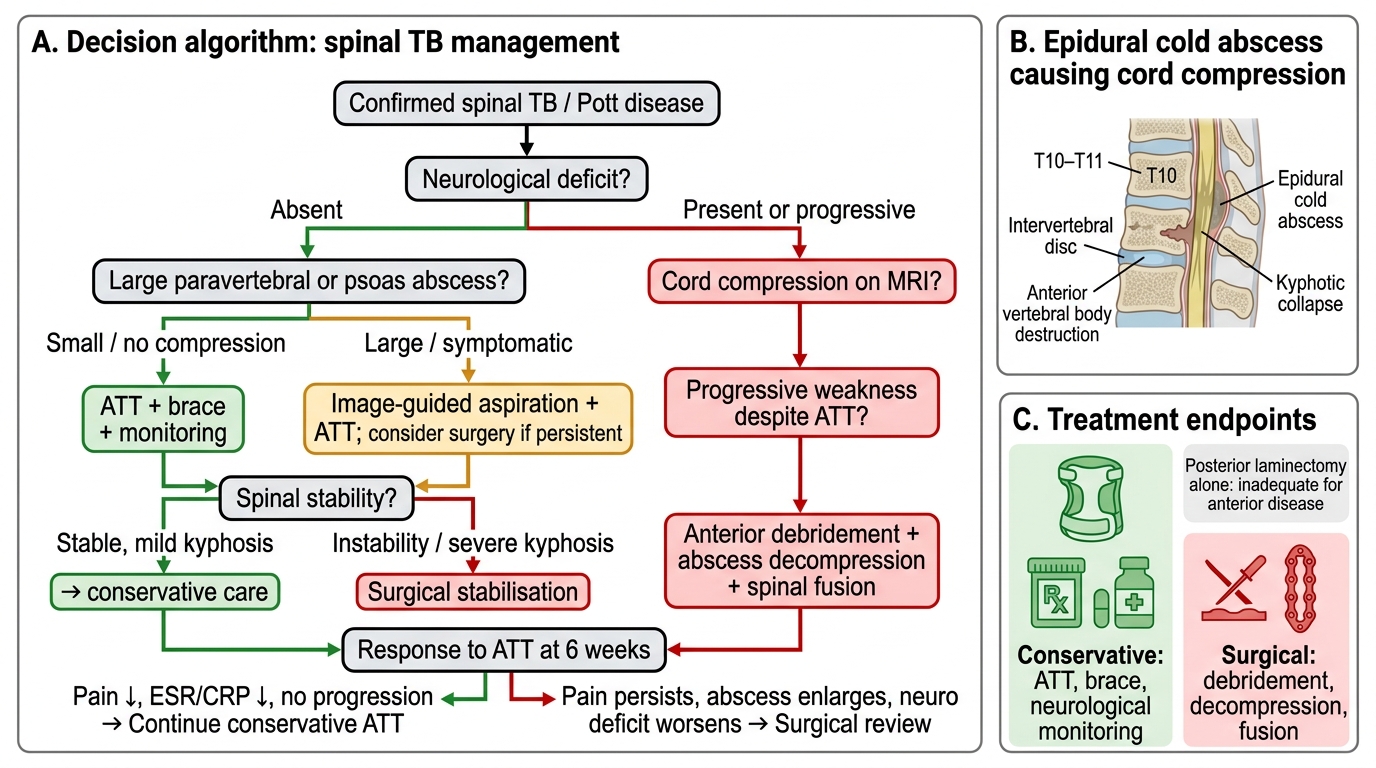
Decision Algorithm for Management of Spinal Tuberculosis
SELF-CHECK
A 45-year-old woman with Pott's disease at T10-T11 develops progressive lower limb weakness (grade 3/5 bilateral) over 4 weeks despite 8 weeks of ATT. MRI shows an epidural cold abscess compressing the cord. What is the most appropriate next step?
A. Increase the duration of ATT to 18 months and continue conservative management
B. Perform posterior laminectomy alone to relieve the compression
C. Anterior debridement, decompression of the epidural abscess, and spinal fusion
D. Physiotherapy and spinal brace without surgical intervention
Reveal Answer
Answer: C. Anterior debridement, decompression of the epidural abscess, and spinal fusion
Progressive neurological deficit due to active cord compression by an epidural cold abscess is a clear surgical indication. Posterior laminectomy alone is inadequate and potentially dangerous — it removes the posterior tension band while the anterior compressive pathology (abscess and infected bone) remains untreated, risking increased instability and kyphosis. The correct approach is anterior debridement (removal of the infected tissue/abscess), decompression of the spinal canal, and stabilisation with strut grafting and fusion. This directly addresses the source of compression and restores spinal stability, allowing neurological recovery. ATT continues throughout the perioperative and postoperative period.
SELF-CHECK
Which of the following is the MOST IMPORTANT clinical feature that distinguishes a cold abscess of skeletal TB from a pyogenic abscess?
A. The cold abscess is always larger than a pyogenic abscess
B. The cold abscess has no local warmth, redness, or tenderness; the overlying skin appears normal
C. The cold abscess contains frank pus on aspiration whereas the pyogenic abscess contains caseous material
D. Cold abscesses are always located in the inguinal region while pyogenic abscesses occur at any site
Reveal Answer
Answer: B. The cold abscess has no local warmth, redness, or tenderness; the overlying skin appears normal
A cold abscess is characterised by the ABSENCE of the classical signs of acute inflammation: the overlying skin is normal in colour (no erythema), the swelling is not warm on palpation (no local heat), and it is non-tender or only mildly uncomfortable. This is because the underlying pathology is a chronic granulomatous reaction (TB), not an acute suppurative reaction with polymorphonuclear leucocyte infiltration and prostaglandin-mediated vasodilation. The term 'cold' specifically refers to the absence of heat and redness. Pyogenic abscesses (from Staphylococcus, Streptococcus, Gram-negatives) produce the classical Celsian signs of rubor, calor, dolor, and tumor with systemic sepsis.
CLINICAL PEARL
Key distinguishing features: Skeletal TB vs Pyogenic Osteomyelitis/Septic Arthritis
The single most important clinical discriminator is TEMPO: skeletal TB is indolent (months to years of symptoms), while pyogenic bone and joint infections are acute (days to weeks, with fever, rigidity, and severe local signs). Remember: a 'cold abscess' has no heat, no redness, and no tenderness — these absent local signs are diagnostic clues.
The 6 C's of Pott's disease:
1. Chronic (insidious onset over months)
2. Cold abscess (no heat, redness, or tenderness)
3. Collapse (anterior wedging of vertebral body)
4. Cord compression (Pott's paraplegia — the emergency)
5. Commence ATT (6-month regimen, NTEP guidelines)
6. Consider surgery (progressive neurology, instability, or large abscess)
A reminder on the most common site: Pott's disease most commonly affects the lower thoracic and thoracolumbar junction (T10-L2) — not the cervical spine. The lower thoracic spine has the least mobility and is under the greatest mechanical stress, predisposing it to TB seeding.
Self-Assessment — Skeletal Tuberculosis
The following questions are designed to help you consolidate your understanding of skeletal tuberculosis and ensure you have mastered the key concepts required for your final professional examination. Skeletal TB is a high-yield examination topic because it tests your ability to integrate pathology, clinical diagnosis, and management across the musculoskeletal system, and because several aspects of its presentation run counter to first instincts: the tempo is slow, not fast; the abscess is cold, not hot; and for cord compression surgery, the approach is anterior, not posterior. Work through each question systematically, relating your answer back to the pathophysiological principles you have just studied. Where you find a gap, return to the relevant section rather than simply memorising the answer. Reflect on the clinical cases used throughout this module — they represent real exam scenarios.
Concept check questions:
- A 12-year-old child presents with a limp and pain in the right hip for 4 months. Examination shows restriction of abduction and internal rotation with a positive Thomas test (fixed flexion deformity of 15°). ESR = 88 mm/h. Plain X-ray shows periarticular osteoporosis and marginal erosions at the femoral head. What is the diagnosis, and what investigation would you prioritise?
- Enumerate the indications for surgical intervention in Pott's disease. Which procedure is preferred for anterior cord compression, and why is posterior laminectomy alone considered inadequate?
- A patient on ATT for spinal TB has a psoas abscess that has reduced in size over 3 months but has not completely resolved. Would you recommend aspiration or surgical drainage? What factors would influence your decision?
- Define Pott's paraplegia. Distinguish between the "active" and "healed" types based on pathological mechanism and response to treatment.
- Describe the typical X-ray findings in spinal TB and explain why plain X-ray changes are late compared to MRI.
Key facts to remember for examinations:
- Most common site of skeletal TB: Spine (50% of skeletal TB cases); within the spine, the lower thoracic and thoracolumbar junction (T10-L2) is most affected
- Second most common site: Hip; Third: Knee
- Cold abscess = no local heat, redness, or tenderness
- Gibbus = angular kyphosis from anterior vertebral body collapse
- Pott's paraplegia — active type (epidural abscess/granulation tissue — potentially reversible) vs healed type (bony sequestrum — surgical)
- ATT regimen: 2HRZE/4HR (6 months); extended to 9–12 months in some protocols for complicated spinal TB
- Surgery preferred approach for anterior cord compression: anterior debridement + fusion (NOT posterior laminectomy alone)
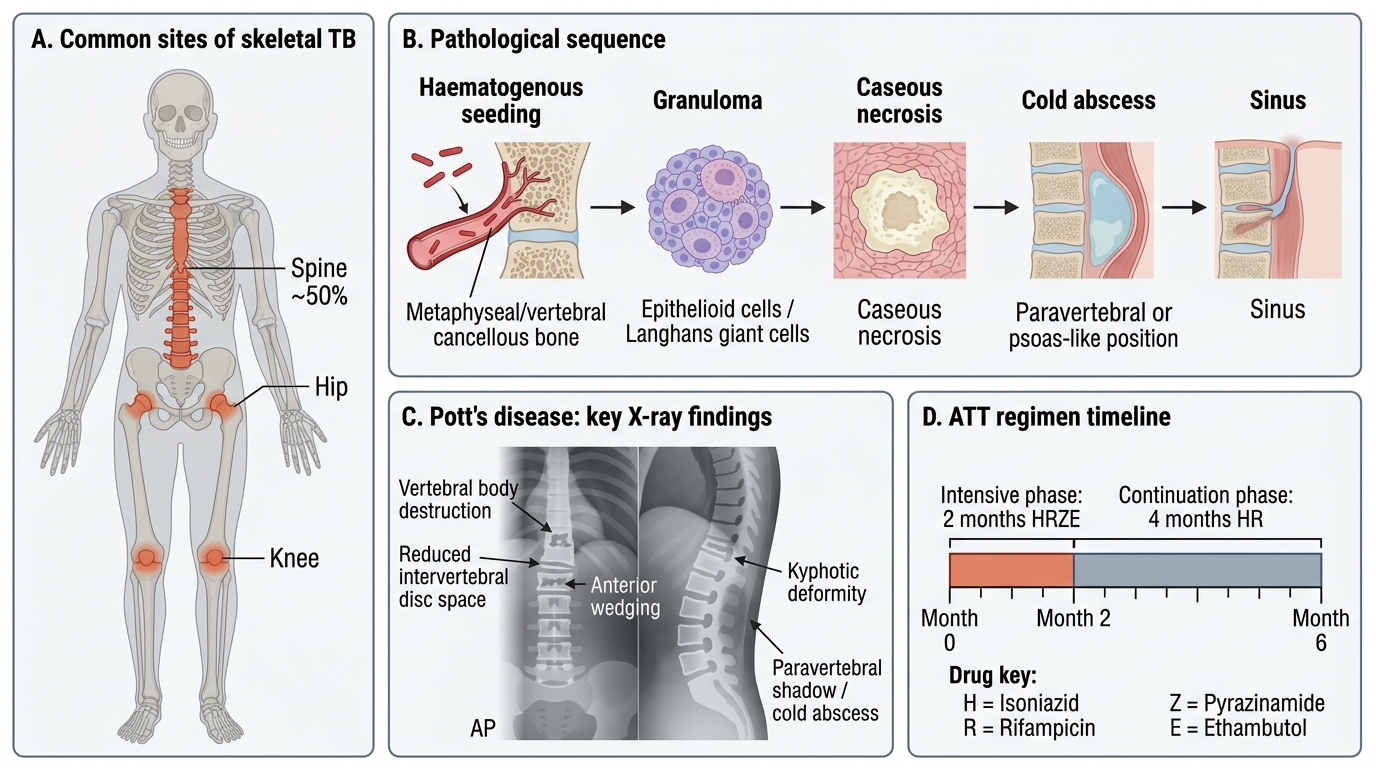
Skeletal Tuberculosis: Sites, Pathology, X-ray Findings, and ATT