Page 2 of 12
OR5.1 | Inflammatory Polyarthritis Clinical Approach — SDL Guide (Part 2)
Ankylosing Spondylitis: Pathogenesis and Tissue Lesions
Ankylosing spondylitis (AS) is the prototype of the seronegative spondyloarthropathies (SpA) — a group of conditions united by the absence of RF, the presence of axial inflammation, and a strong association with HLA-B27. AS predominantly affects young men (male:female ratio approximately 3:1) with onset typically in the second and third decades. Its name from the Greek ankylos (bent/fused) and spondylos (vertebra) accurately describes its end-stage.
HLA-B27 — an MHC class I allele present in approximately 8–10% of the Indian general population — is found in 90–95% of AS patients. Despite this strong association, only a minority of HLA-B27-positive individuals develop AS, indicating additional genetic and environmental factors are required. The leading hypothesis is the arthritogenic peptide hypothesis: HLA-B27 presents specific endogenous or microbial peptides to CD8+ cytotoxic T cells at the entheses (the insertions of ligaments, tendons, and joint capsules into bone), triggering an inappropriate immune response. Enthesitis — inflammation at the enthesis — is the pathological hallmark of the spondyloarthropathies, distinguishing them fundamentally from RA where synovitis predominates.
The inflammatory process starts at the sacroiliac joints (sacroiliitis is the earliest and most consistent finding) and ascends through the spine. Enthesitis at the discovertebral junction leads to squaring of vertebral bodies (loss of the normal anterior concavity); formation of syndesmophytes — bony bridges from ossification of the outer annulus fibrosus (Sharpey's fibres); and ultimately fusion producing the 'bamboo spine' on plain X-ray. Inflammation also affects costovertebral joints (limiting chest expansion — a key clinical sign) and the hip and shoulder joints (root joints, affected in severe disease).
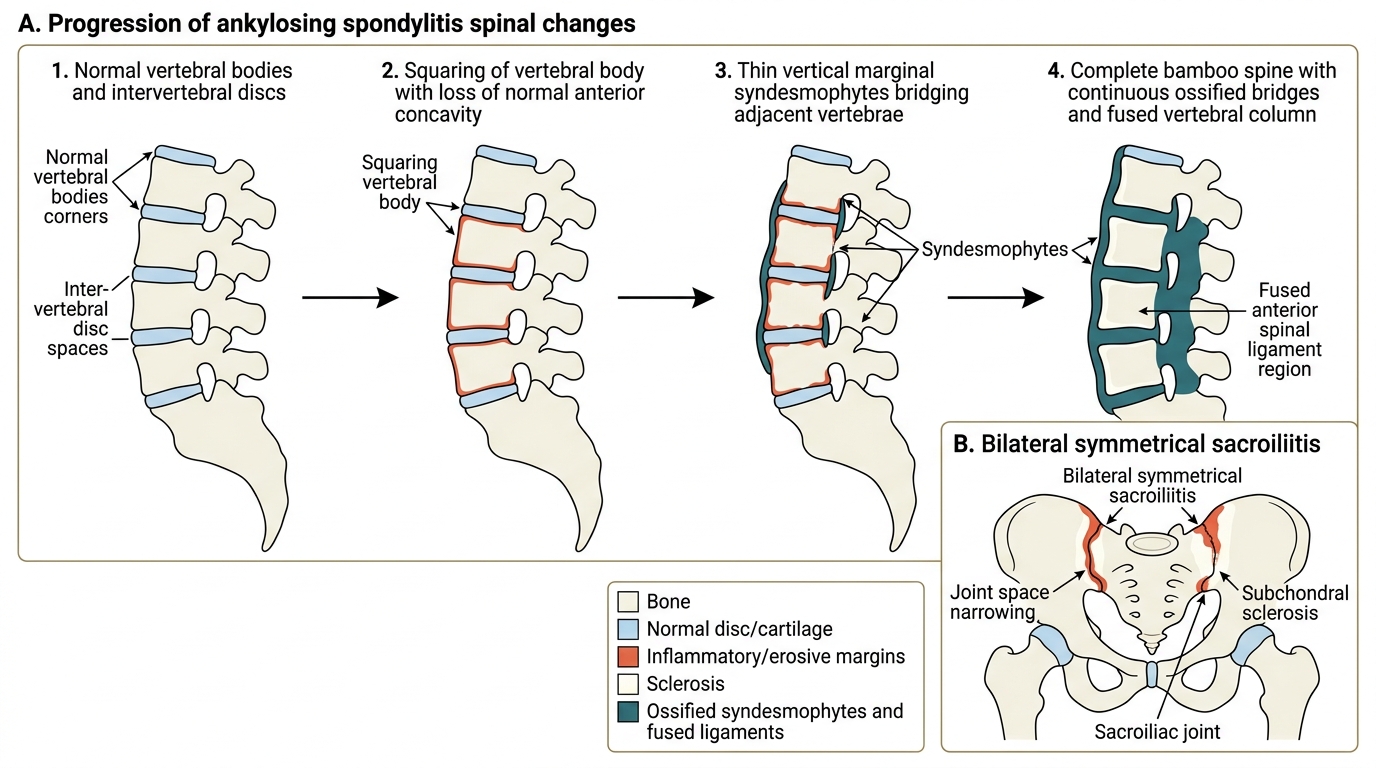
Ankylosing Spondylitis: Spine Progression and Sacroiliitis
Psoriatic Arthritis: Pathogenesis and Distinct Joint Patterns
Psoriatic arthritis (PsA) is a seronegative inflammatory arthritis associated with psoriasis — a chronic autoimmune skin disease characterised by well-demarcated erythematous plaques with silvery scales, most commonly on the extensor surfaces of elbows, knees, scalp, and the periumbilical region. PsA affects approximately 20–30% of psoriasis patients, and in 10–15% arthritis precedes the skin disease. The joint disease is driven by psoriatic plaques releasing inflammatory cytokines — particularly IL-17 and IL-23 — that reach the joint via the circulation, producing a distinct form of enthesitis and synovitis.
Whereas RA attacks the synovium and spares the DIPs, PsA is distinctive in attacking multiple compartments. It has five recognised clinical patterns (Moll and Wright classification): (1) DIP involvement predominant — pathognomonic of PsA, as pure DIP arthritis is not seen in RA or AS; (2) asymmetric oligoarthritis — most common at presentation; (3) symmetric polyarthritis resembling RA but RF-negative; (4) axial involvement resembling AS but with asymmetric sacroiliitis and non-contiguous syndesmophytes; (5) arthritis mutilans — the most destructive form, with resorption of phalanges producing the 'pencil-in-cup' deformity.
The two pathognomonic clinical features of PsA are dactylitis and nail changes. Dactylitis ('sausage digit') refers to diffuse swelling of an entire finger or toe from simultaneous flexor tenosynovitis and small joint synovitis — it is essentially absent in RA. Nail changes in PsA include pitting (small pits on the nail surface), onycholysis (separation of nail plate from nail bed — yellowish-white discolouration), subungual hyperkeratosis, and oil-drop discolouration. Nail changes are more numerous when DIP joints are involved, since the nail root is anatomically adjacent to the DIP joint enthesis.
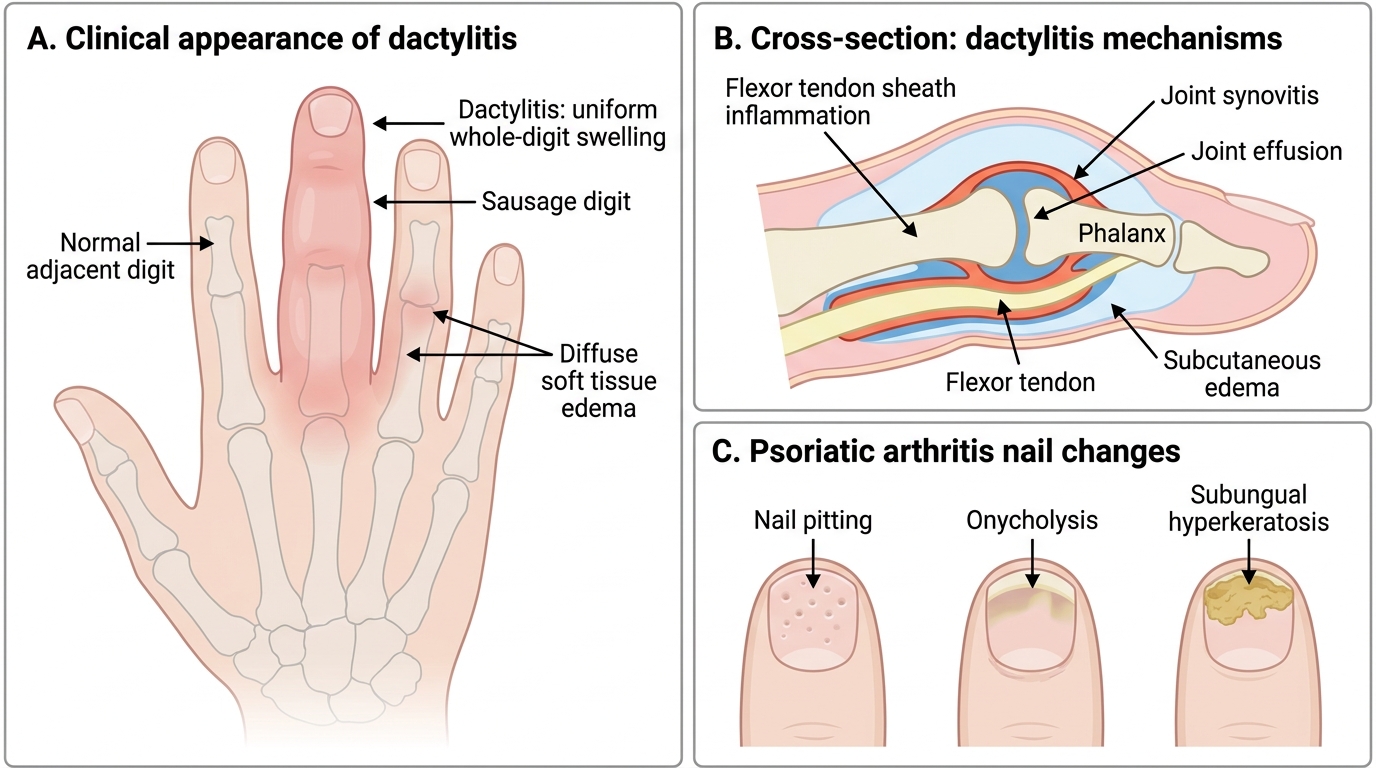
Dactylitis and Nail Changes in Psoriatic Arthritis
SELF-CHECK
A 42-year-old woman with 2-year history of symmetric polyarthritis (MCPs, PIPs, wrists) has RF positive but anti-CCP negative. Which statement about her serology is correct?
A. Anti-CCP negativity rules out RA
B. RF alone is highly specific for RA at over 95%
C. Anti-CCP is more specific for RA than RF; RF-positive and anti-CCP-negative patients tend to have less erosive disease
D. RF and anti-CCP have equal sensitivity and specificity for RA
Reveal Answer
Answer: C. Anti-CCP is more specific for RA than RF; RF-positive and anti-CCP-negative patients tend to have less erosive disease
Anti-CCP antibody has a specificity of ~95% for RA compared to ~80% for RF. RF is positive in chronic infections, hepatitis C, Sjögren's syndrome, and other conditions. Patients who are RF-positive but anti-CCP-negative generally have less erosive disease. Anti-CCP negativity does not exclude RA — approximately 30% of RA patients are seronegative (anti-CCP-negative).
Rheumatoid Arthritis: Examination, Investigations, and Imaging
The clinical presentation of RA builds insidiously. The classic triad at presentation is symmetrical polyarthritis involving MCPs, PIPs, and wrists, prolonged morning stiffness (>1 hour), and systemic upset (fatigue, low-grade fever, weight loss). Crucially, DIP joints are spared in RA — this immediately distinguishes RA from osteoarthritis (which preferentially attacks DIPs with Heberden's nodes) and from psoriatic arthritis (which can involve DIPs). Examination reveals boggy, warm, non-erythematous synovial thickening (as opposed to the bony, hard enlargement of OA nodes), positive MCP squeeze test (pain on lateral compression of the MCP row), and reduced grip strength. In established disease the deformities appear: ulnar deviation, Boutonnière, and swan-neck as described above.
Extra-articular manifestations reflect systemic autoimmune activity: rheumatoid nodules (firm subcutaneous nodules over the olecranon and finger dorsum — present in ~20% of seropositive patients); pulmonary involvement (interstitial lung disease, pleuritis); cardiac (pericarditis); ocular (scleritis, episcleritis); and Felty's syndrome (RA + splenomegaly + neutropenia). Cervical spine involvement — especially atlantoaxial subluxation — is a serious, potentially cord-compressing complication in advanced RA.
Investigations follow logically: RF (positive in ~70% of RA; specificity ~80%); anti-CCP (sensitivity ~70%, specificity ~95% — the more specific test; positive anti-CCP predicts more erosive disease); ESR and CRP (monitor disease activity); FBC (normocytic normochromic anaemia, thrombocytosis); and most importantly plain X-rays of hands and feet — the sequence from periarticular osteoporosis → soft-tissue swelling → juxta-articular erosions → joint space narrowing → subluxation/deformity is the radiological narrative of progressive RA. The 2010 ACR/EULAR classification criteria for RA score joint involvement, serology, acute-phase reactants, and symptom duration — a score ≥6/10 classifies definite RA.
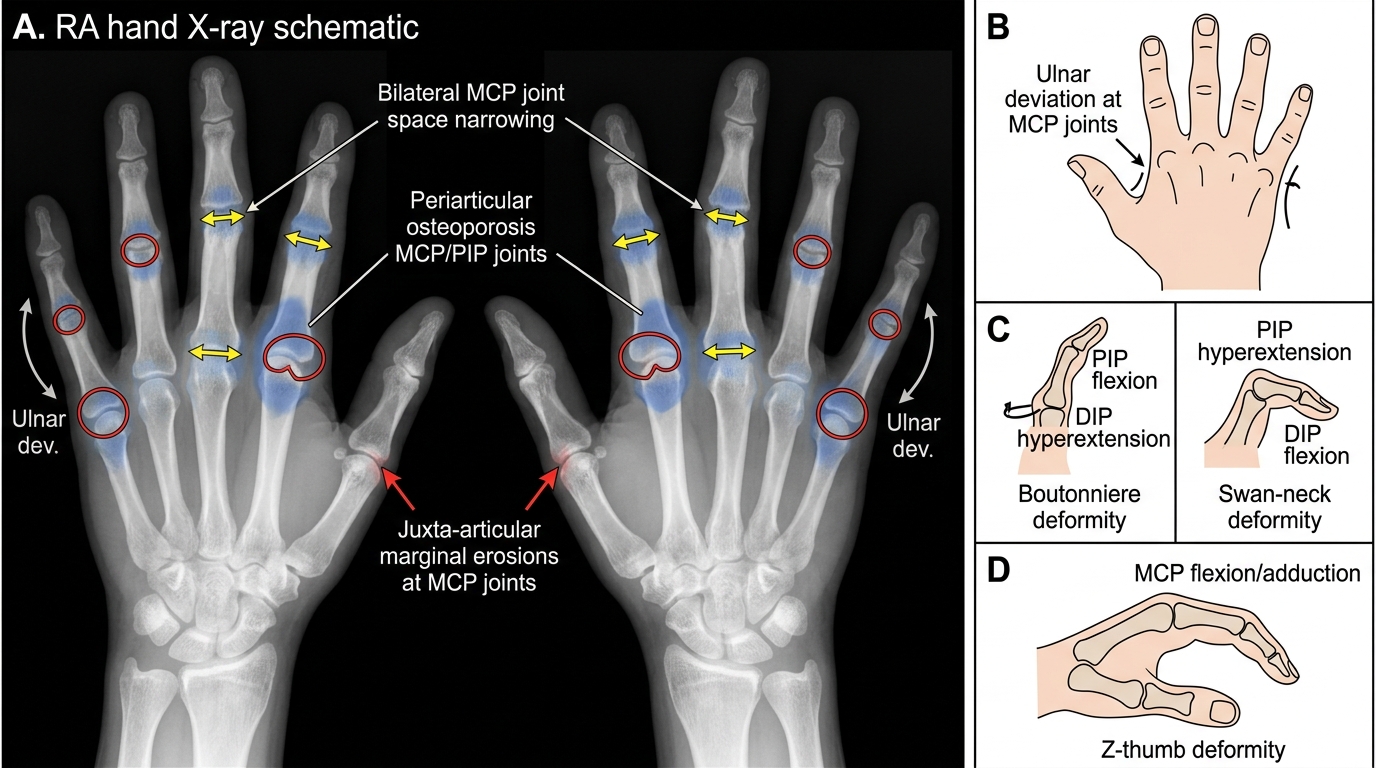
Rheumatoid Arthritis: Hand X-ray Changes and Deformities
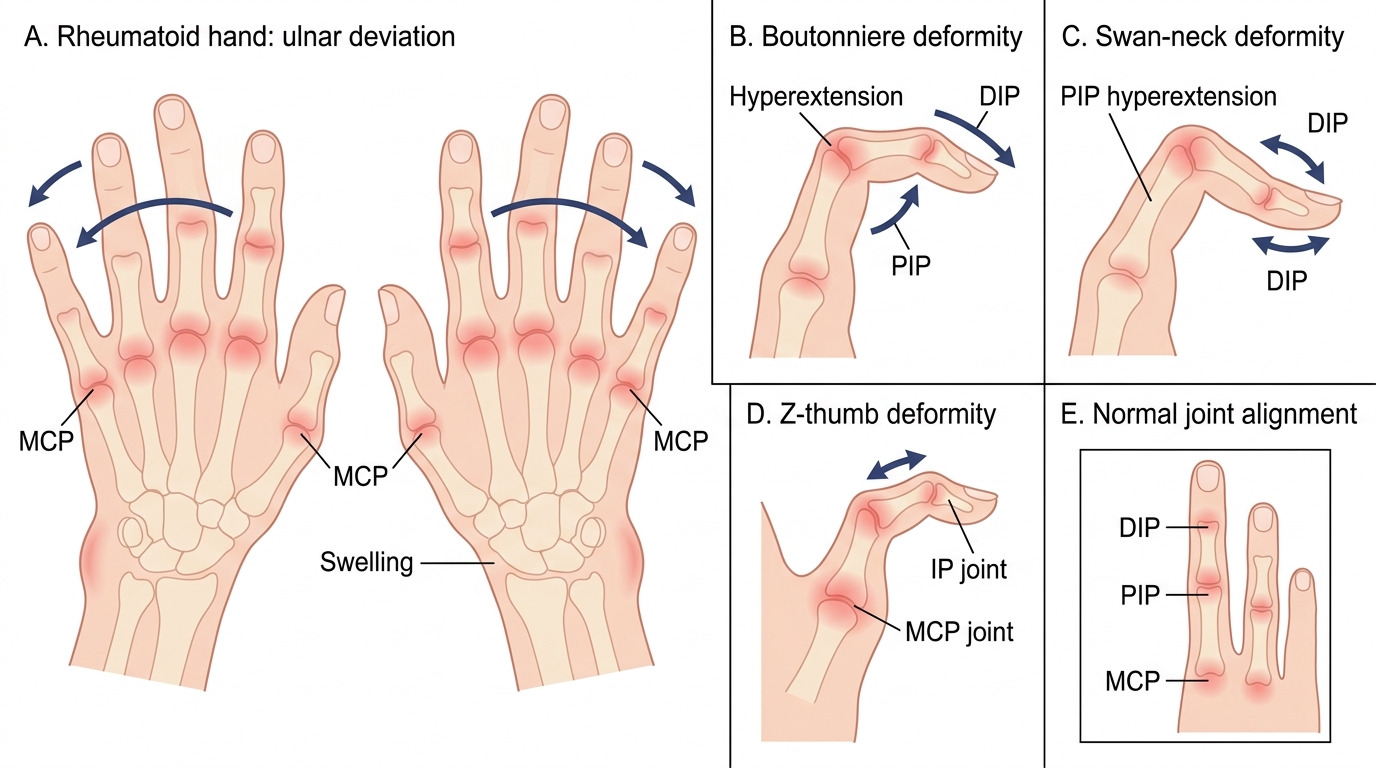
Rheumatoid Arthritis Hand Deformities