Page 3 of 12
OR5.1 | Inflammatory Polyarthritis Clinical Approach — SDL Guide (Part 3)
Ankylosing Spondylitis: Clinical Examination and Diagnostic Criteria
The characteristic clinical presentation is inflammatory back pain — pain and stiffness in the lumbar and gluteal region (sacroiliac referral) that is worse in the morning (lasting >60 minutes), improves with activity and NSAIDs, and characteristically awakens the patient in the second half of the night. Young patients (under 40) with this pattern persisting more than 3 months must be investigated for AS; globally, the average delay from onset to diagnosis is 8–10 years because the condition is routinely dismissed as mechanical back pain.
Four key clinical signs quantify the disease: (1) Schober's test — marks are placed 5 cm below and 10 cm above the lumbosacral junction (L5-S1) with the patient erect; with full forward flexion the distance between marks should increase by ≥5 cm; an increment <5 cm indicates reduced lumbar mobility. (2) Chest expansion — measured at the 4th intercostal space level; normal ≥2.5 cm; reduced in AS due to costovertebral joint inflammation. (3) Occiput-to-wall distance — increases as the thoracic kyphosis becomes fixed. (4) FABER test (Flexion, Abduction, External Rotation) — pain in the SIJ region on pressing the knee toward the examination table localises the lesion to the sacroiliac joint.
Extra-articular features: anterior uveitis (acute unilateral painful red eye) occurs in 25–40% of AS patients; aortic regurgitation (late, ~1%); upper lobe pulmonary fibrosis; and cauda equina syndrome (very late, from arachnoiditis). Investigation: HLA-B27 (positive >90% of AS); X-ray sacroiliac joints — bilateral symmetrical sacroiliitis (grade ≥2 bilateral) is the cornerstone of the modified New York criteria (1984) for definitive AS; MRI sacroiliac joints (STIR sequence showing bone marrow oedema 'shining corners') detects active sacroiliitis before X-ray changes; RF and anti-CCP are negative. The ASAS criteria allow earlier diagnosis including non-radiographic axial SpA.
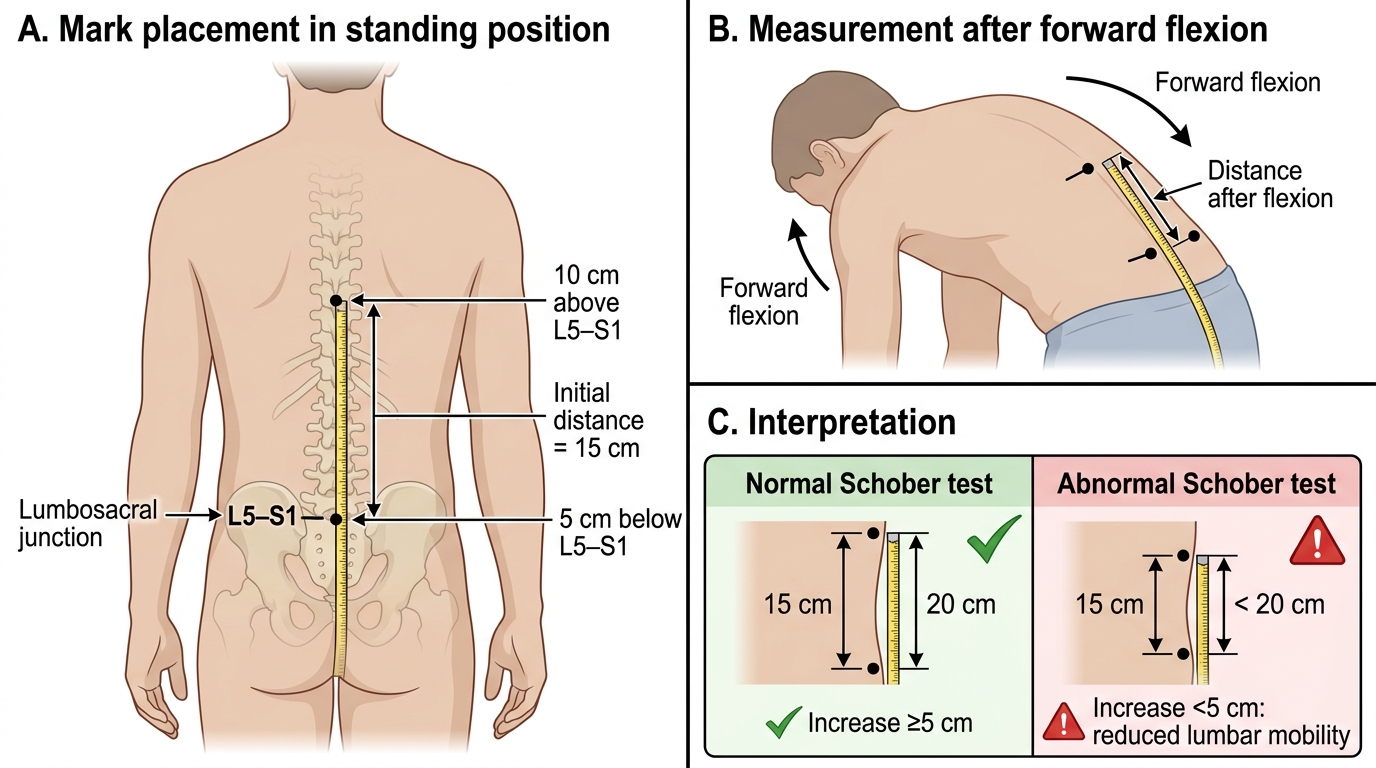
Schober's Test for Lumbar Mobility
Psoriatic Arthritis: Investigations and Radiological Hallmarks
Provided image
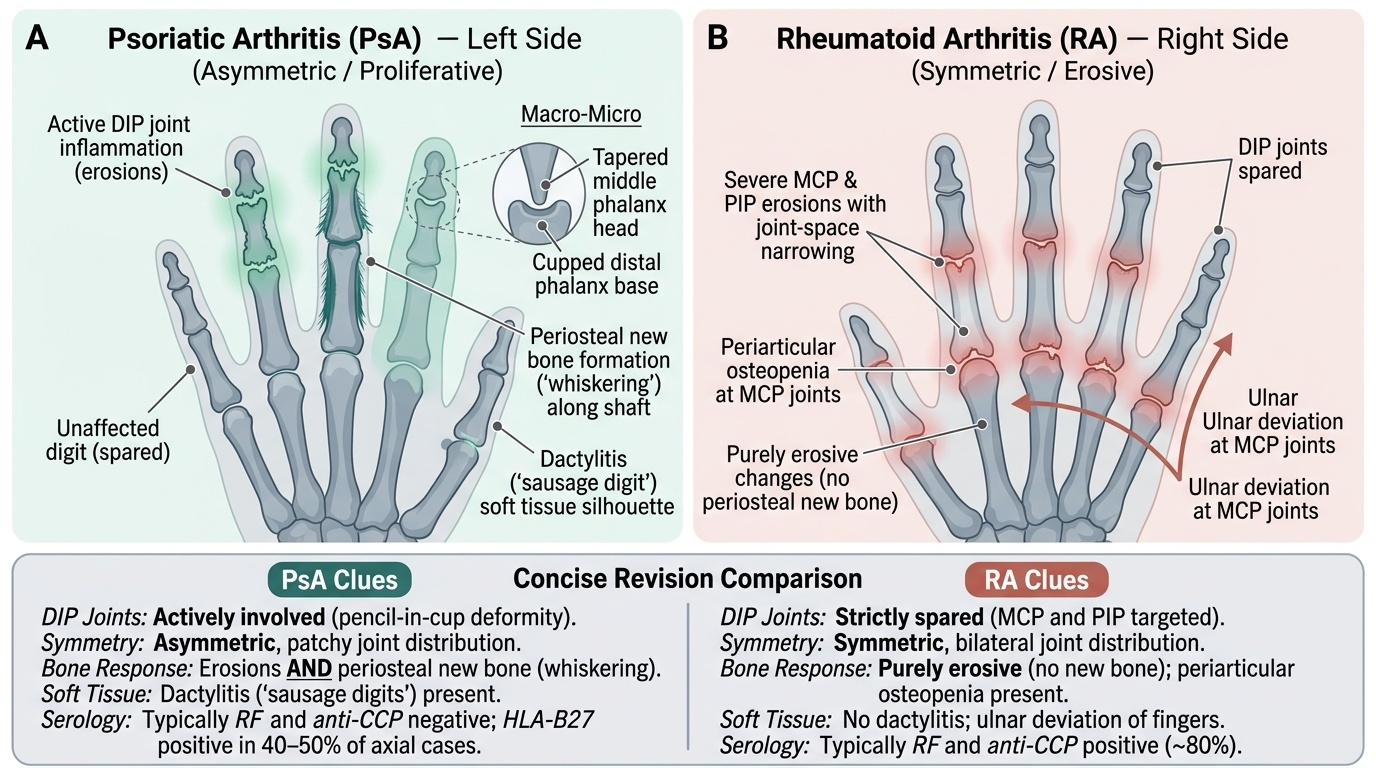
Investigations in PsA are guided by the clinical context. RF and anti-CCP are negative — seronegative status in a patient with psoriasis and arthritis essentially confirms the diagnosis. HLA-B27 is positive in 40–50% of PsA patients with axial involvement, reflecting the SpA overlap. ESR and CRP are elevated in active disease. A unique diagnostic advantage in PsA is the skin and nail examination: finding psoriatic plaques — even in hidden sites (scalp, natal cleft, umbilicus) — in a patient with arthritis immediately establishes the diagnostic context.
The radiological hallmarks of PsA are diagnostically important and distinct: (1) DIP erosions — RA does not affect DIPs; PsA uniquely does. (2) Pencil-in-cup deformity — the most recognisable PsA X-ray finding: resorption of the distal end of the phalanx creates a sharpened 'pencil point' shape fitting into a cup-shaped erosion on the base of the next phalanx. (3) Periosteal new bone formation (called 'whiskering') — PsA has both erosions AND new bone formation along the shaft, in contrast to RA which is purely erosive. (4) Asymmetric sacroiliitis — compared to the bilateral symmetric sacroiliitis of AS. (5) Non-marginal, non-contiguous syndesmophytes that skip spinal levels — unlike AS where syndesmophytes are marginal and contiguous, ascending sequentially from the sacrum.
The two clinical anchors for distinguishing PsA from RA: RA spares DIPs; PsA attacks them. Dactylitis occurs in PsA and essentially does not occur in RA. In the examination, finding dactylitis + DIP involvement + psoriatic skin changes clinches PsA without serology.
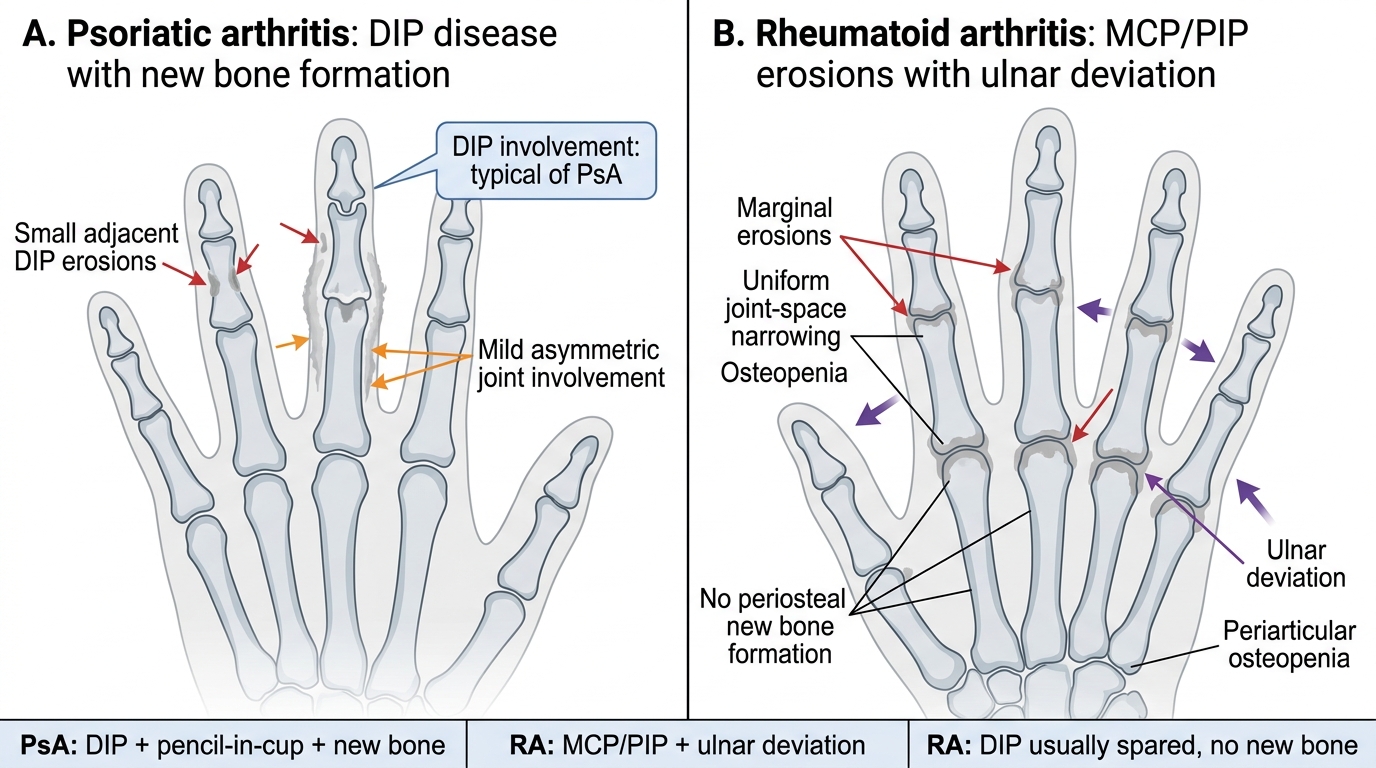
PsA versus RA: Hand X-ray Features
SELF-CHECK
A 36-year-old man presents with asymmetric arthritis: the right index finger is swollen along its entire length, the DIP joints of multiple fingers are involved, and several fingernails show pitting. Skin examination reveals erythematous scaly plaques on both elbows. What is the most likely diagnosis?
A. Rheumatoid arthritis
B. Ankylosing spondylitis
C. Psoriatic arthritis
D. Reactive arthritis
Reveal Answer
Answer: C. Psoriatic arthritis
The combination of dactylitis (entire finger swelling from flexor tenosynovitis + joint inflammation), DIP joint involvement, psoriatic nail changes (pitting), and psoriatic skin plaques is pathognomonic of psoriatic arthritis. RA does not affect DIPs and does not cause dactylitis. AS does not produce dactylitis or nail changes. Reactive arthritis can cause dactylitis but is associated with a preceding genitourinary or enteric infection and does not produce psoriatic skin plaques.
Management: NSAIDs, DMARDs, and Biologics
The central principle of management in inflammatory arthritis is that NSAIDs and analgesics treat symptoms but do not prevent joint destruction; only disease-modifying antirheumatic drugs (DMARDs) alter the disease course by targeting the underlying immune mechanism. This distinction between symptom control and disease modification is a conceptual cornerstone that every MBBS graduate must internalise.
DMARDs are categorised as: (1) Conventional synthetic DMARDs (csDMARDs): methotrexate is the anchor first-line DMARD for RA — a folate antagonist given weekly (7.5–25 mg/week orally or subcutaneously) with daily folic acid supplementation. It reduces disease activity, prevents erosions, and reduces disability. Common adverse effects include nausea, oral ulcers, hepatotoxicity (requiring periodic LFT monitoring), and bone marrow suppression. It is absolutely contraindicated in pregnancy and in chronic liver disease or heavy alcohol use. Hydroxychloroquine and sulfasalazine are alternative or adjunct csDMARDs. (2) Biologic DMARDs (bDMARDs): TNF inhibitors (etanercept, adalimumab, infliximab) are the prototype biologics for RA and SpA; IL-6 inhibitors (tocilizumab) for RA; IL-17 inhibitors (secukinumab) — first-line biologic for AS and PsA, where IL-17 is the dominant cytokine; anti-CD20 (rituximab — B cell depletion in seropositive RA). Biologics are reserved for moderate-to-severe disease failing csDMARDs. (3) Targeted synthetic DMARDs: JAK inhibitors (tofacitinib, baricitinib) for RA.
Before starting any biologic, latent tuberculosis must be screened (Mantoux/IGRA + chest X-ray) because TNF inhibitors reactivate latent TB — critically important in India's high TB-burden setting.
For AS, NSAIDs remain first-line and uniquely there is evidence that continuous NSAID use slows radiographic progression. For AS failing NSAIDs, IL-17A inhibitors (secukinumab) or TNF inhibitors are used; conventional csDMARDs do not work for axial AS. For PsA, methotrexate addresses skin and peripheral joints; IL-17 inhibitors are the preferred biologics. Treat-to-target — aiming for minimal disease activity guided by validated scores (DAS-28 for RA, ASDAS for AS, MDA for PsA) — is the modern management paradigm for all three conditions.
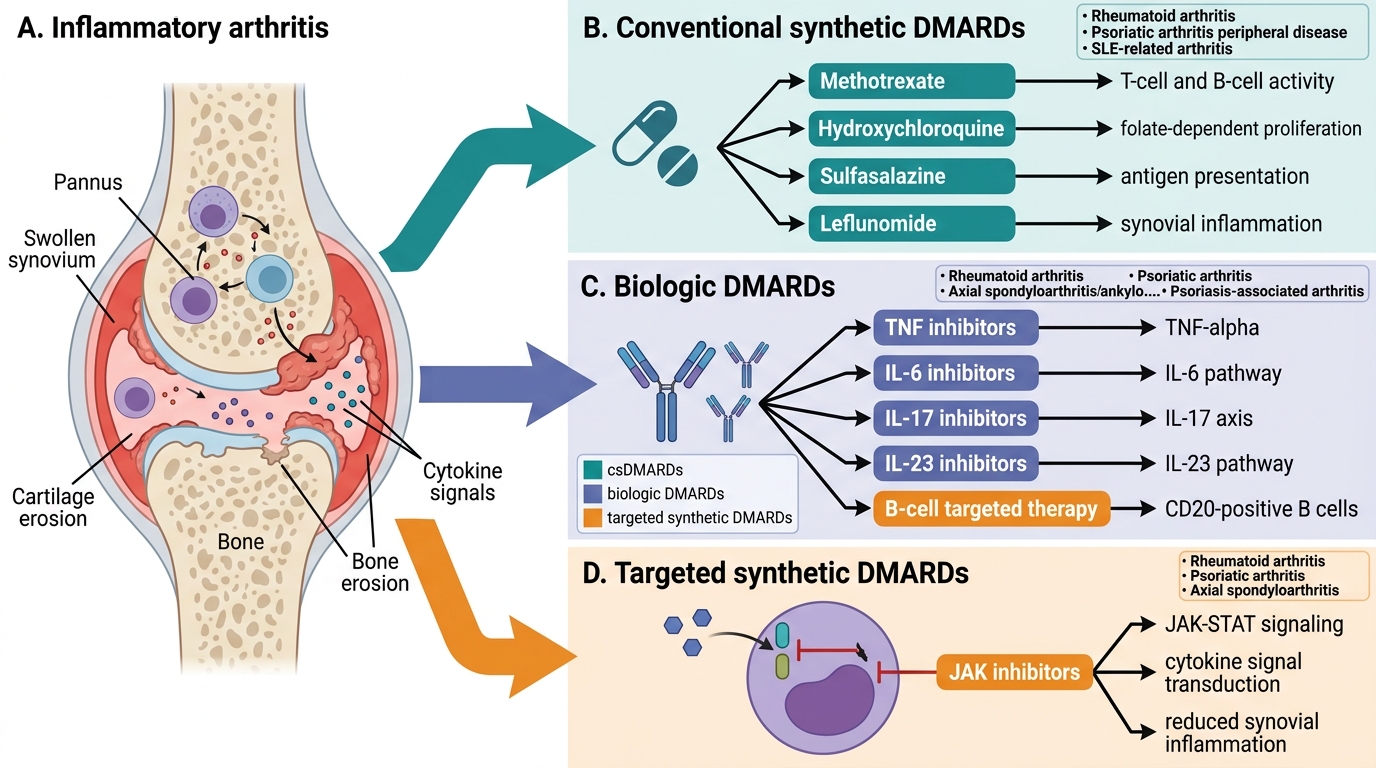
DMARD Classification and Disease Targets