Page 1 of 12
OR7.1 | Metabolic Bone Disease Assessment — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis and classify the four major metabolic bone disorders: osteoporosis, osteomalacia, rickets, and Paget's disease
- Distinguish the biochemical profiles (Ca, PO4, ALP, vitamin D, PTH) for each disorder and interpret these in clinical context
- Identify clinical and radiological features of each condition, including DEXA T-score interpretation, Looser's zones, rickets deformities, and Pagetic changes
- Outline the deformities arising in rickets (genu varum, genu valgum, rachitic rosary, widened metaphyses) and describe their orthopaedic management
- Formulate a management plan for each metabolic bone disease, including pharmacological, surgical, and preventive strategies
INSTRUCTIONS
Metabolic bone diseases are among the most prevalent musculoskeletal conditions worldwide, underpinning a major burden of fragility fractures, deformity, pain, and disability. In India, vitamin D deficiency is endemic, making osteomalacia and rickets everyday diagnoses rather than textbook curiosities. Osteoporosis silently erodes bone strength across millions of post-menopausal women and elderly men, leading to hip fractures that carry a one-year mortality comparable to many cancers. Paget's disease, though less common in Indian populations, produces dramatic radiological and biochemical changes and carries the risk of high-output cardiac failure. Understanding these four disorders — their mechanisms, their biochemical fingerprints, and their distinct management strategies — is fundamental to orthopaedic and general medical practice at the final-year level. This module uses a clinico-biochemical correlation approach: you will learn to read the Ca/PO4/ALP/PTH/vitamin D pattern as a metabolic signature that points to the correct diagnosis before imaging is even obtained.
References
- Maheshwari's Essential Orthopaedics, 5th edition, Ch 14 (Metabolic Bone Disorders) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th edition, Ch 7 (Metabolic and Endocrine Disorders) (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th edition (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 65-year-old post-menopausal woman slips on a wet floor and sustains a wrist fracture from minimal impact — an injury that would never break a healthy young bone. Her X-ray shows thinned cortices and the radiology report mentions 'osteopenic appearance.' Meanwhile, across the ward, a 2-year-old child from a rural area presents with bowed legs and enlarged wrist joints, and a 10-year-old urban child from the same community displays knock-knees with frontal bossing of the skull. In the fracture clinic, a 60-year-old man complains of severe thigh pain and a hat that no longer fits — his skull X-ray resembles 'cotton wool' and his alkaline phosphatase is ten times normal. Four patients, four mechanisms, one unifying theme: disordered bone metabolism. Today you will learn to think biochemically and radiologically about each condition so that you can read a set of lab results and immediately know which disease you are facing.
WHY THIS MATTERS
India has one of the world's highest burdens of vitamin D deficiency, estimated at 70-100% prevalence in some population groups due to dietary insufficiency, limited sun exposure in urban settings, and darker skin pigmentation that reduces cutaneous vitamin D synthesis. This means osteomalacia in adults and rickets in children are genuinely common diseases you will encounter in any district hospital or urban outpatient clinic. Osteoporosis-related hip fractures in India are projected to increase dramatically as the elderly population grows; the one-year mortality after hip fracture in elderly Indian patients exceeds 20%, placing early diagnosis and prevention at the centre of public health orthopaedics. Paget's disease, while less frequent in South Asia than in northern Europe, requires recognition because its complications — nerve compression, high-output heart failure, pathological fracture, and malignant transformation — are life-threatening. Your ability to correctly interpret a biochemical panel and request the right imaging will directly determine whether these patients receive curative treatment early or present years later with irreversible deformity or complications.
RECALL
Before exploring metabolic bone disease, recall the foundations of normal bone physiology from Year 1 Biochemistry and Physiology. Bone is a dynamic connective tissue continuously remodelled by a coupled process: osteoclasts (derived from monocyte-macrophage lineage) resorb old bone by secreting acid and proteases into a sealed resorption lacuna, while osteoblasts (derived from mesenchymal stem cells) deposit new osteoid — a collagen type I matrix — which is then mineralised by calcium hydroxyapatite crystal deposition. This coupling is regulated by the RANK-RANKL-OPG axis, parathyroid hormone (PTH), and vitamin D. Recall that PTH is secreted from the parathyroid glands in response to low ionised calcium; it raises calcium by stimulating osteoclastic resorption, increasing renal tubular calcium reabsorption, and activating 1-alpha-hydroxylase in the kidney to convert 25-hydroxyvitamin D to the active calcitriol (1,25-dihydroxyvitamin D). Calcitriol primarily acts on the small intestine to promote calcium and phosphate absorption. The result is a tightly regulated balance: when calcium falls, PTH rises, calcitriol rises, and calcium is restored. Also recall that alkaline phosphatase (ALP) is an enzyme produced by osteoblasts during bone formation; a rising ALP signals increased osteoblastic activity. These four parameters — serum calcium, serum phosphate, serum ALP, and serum PTH/vitamin D — are the biochemical compass for all metabolic bone diseases.
Osteoporosis: Definition, Epidemiology, and Aetiopathogenesis
Osteoporosis is defined as a systemic skeletal disorder characterised by reduced bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fracture. The World Health Organization (WHO) operationalises this definition using dual-energy X-ray absorptiometry (DEXA): a T-score compares the patient's bone mineral density (BMD) to that of a healthy young adult reference population at the same anatomical site. A T-score at or above -1.0 standard deviations (SD) is normal; between -1.0 and -2.5 SD is osteopenia (low bone mass, a risk state rather than disease); at or below -2.5 SD is osteoporosis. A fragility fracture — a fracture resulting from a force that would not normally break a healthy bone, such as a fall from standing height — establishes the diagnosis of established (severe) osteoporosis regardless of the T-score value. Bone mass peaks around age 25-30 years and then declines throughout adult life. In women, the accelerated phase of bone loss occurs in the five years around the menopause, driven by oestrogen withdrawal: oestrogen normally suppresses osteoclast activity via OPG upregulation, so its loss unleashes accelerated osteoclastic resorption that outpaces osteoblastic formation. The net result is an absolute loss of bony trabeculae (not simply thinning) — once a trabecular plate is perforated and resorbed, it cannot be rebuilt, explaining why early treatment matters more than late rescue. Risk factors fall into non-modifiable (female sex, advancing age, Asian or Caucasian ethnicity, family history, premature menopause before age 45) and modifiable (cigarette smoking, excessive alcohol, low calcium and vitamin D intake, physical inactivity, prolonged glucocorticoid use — the most common drug-induced cause of osteoporosis).
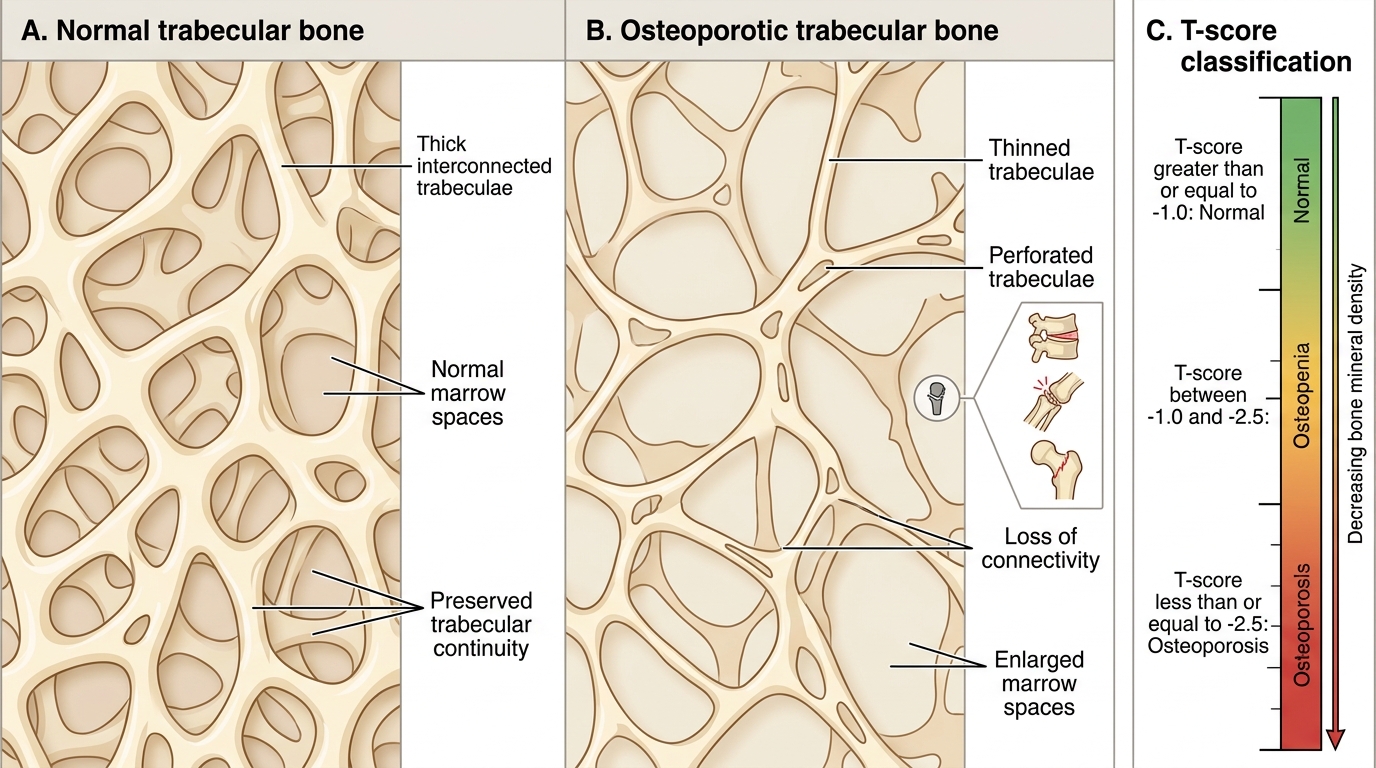
Trabecular Bone Changes and T-score Classification in Osteoporosis
The major clinical consequence of osteoporosis is fracture. Classic osteoporotic fracture sites are the vertebral bodies (compression fractures causing loss of height and kyphosis), distal radius (Colles' fracture in elderly women), and the proximal femur (hip) — the most dangerous in terms of mortality and morbidity. Vertebral fractures are frequently silent (identified only on imaging as loss of anterior vertebral height) but may present as acute severe back pain. Hip fractures require surgical fixation or replacement and carry a one-year mortality of approximately 20-30% in elderly patients due to immobility-related complications (pneumonia, DVT, pulmonary embolism, pressure sores). A key clinical sign is that the limb is shortened and externally rotated in a displaced femoral neck fracture.
Osteomalacia: Defective Mineralisation in Adults
Osteomalacia is a metabolic bone disorder in adults characterised by defective mineralisation of newly formed osteoid, resulting in the accumulation of unmineralised osteoid on bone surfaces. The fundamental abnormality is that adequate bone matrix (type I collagen) is produced by osteoblasts, but the calcium and phosphate needed to crystallise into hydroxyapatite are insufficient, either because of vitamin D deficiency (reducing intestinal Ca/PO4 absorption), hypophosphataemia (primary renal phosphate wasting as in X-linked hypophosphataemia or oncogenic osteomalacia), or rarely impaired mineralisation from drugs (e.g. aluminium toxicity, bisphosphonate overuse) or hereditary enzyme deficiencies. In India, the overwhelmingly predominant cause is nutritional vitamin D deficiency — the serum 25-hydroxyvitamin D level falls below 20 ng/mL (50 nmol/L), leading to reduced calcium absorption, compensatory PTH rise (secondary hyperparathyroidism), and increased renal calcium reabsorption with increased phosphate excretion, worsening hypophosphataemia. The net result: bone collagen is laid down normally but fails to mineralise, leaving thick seams of unmineralised osteoid and a skeleton that is soft, deformable, and prone to incomplete fractures.
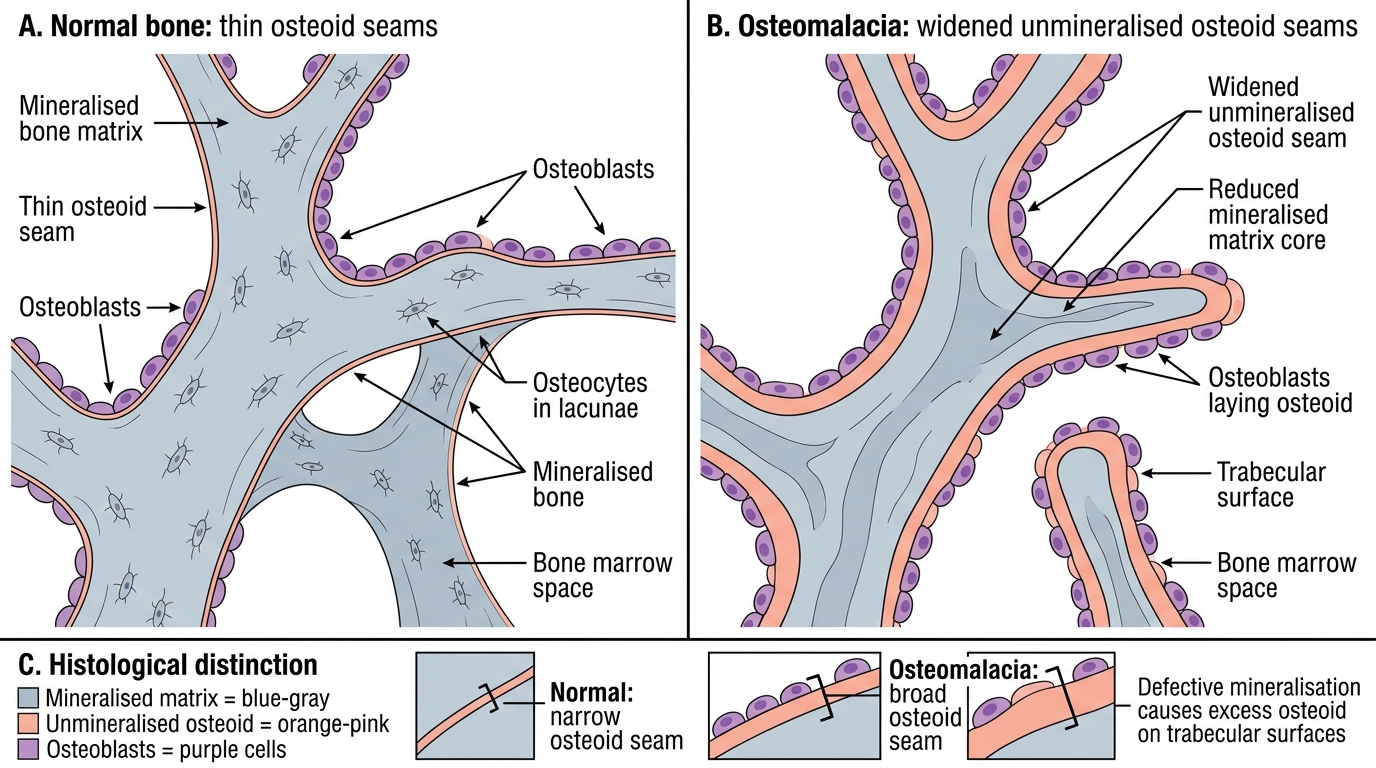
Normal Bone Versus Osteomalacic Bone
The clinical presentation of osteomalacia in adults includes diffuse bone pain and tenderness (typically proximal — pelvis, thighs, ribs), proximal muscle weakness (vitamin D has direct myotrophic effects; deficiency causes a myopathy affecting hip girdle muscles, producing a characteristic waddling gait), and pathological fractures through softened bone. The pathognomonic radiological finding is the Looser's zone (also called Milkman's fracture or pseudofracture): a narrow, ribbon-like translucent band — representing unmineralised osteoid cutting perpendicular to the cortex — seen at sites of stress, typically the medial femoral neck, pubic rami, rib margins, axillary margin of the scapula, and ulna. Looser's zones are characteristically bilateral and symmetric. Generalised radiolucency and loss of cortical definition are additional radiological features. Biochemically, osteomalacia is characterised by low serum calcium, low serum phosphate, elevated ALP (reflecting increased osteoblastic activity attempting to lay down more osteoid), elevated PTH (secondary hyperparathyroidism), and low serum 25-hydroxyvitamin D.
Rickets: Aetiopathogenesis and the Growing Skeleton
Rickets is the paediatric equivalent of osteomalacia — defective mineralisation of the growth plate and adjacent metaphyseal bone in a child with open epiphyses. The same fundamental process (inadequate calcium and phosphate for hydroxyapatite crystallisation) is at work, but the consequences are far more dramatic in the growing skeleton because the growth plate (physis) is highly metabolically active: it relies on zone-of-provisional-calcification mineralisation for normal chondroblast apoptosis and conversion to bone. When mineralisation fails, the growth plate expands irregularly and widened bands of hypertrophied, unmineralised cartilage accumulate — producing the characteristic radiological and clinical deformities. Nutritional vitamin D deficiency is the dominant cause in India (where exclusive breastfeeding without D supplementation, premature weaning onto non-fortified gruel, and minimal sun exposure combine to produce this deficiency). Other causes include calcium-deficient rickets (dietary calcium deficiency, even with normal vitamin D — common in sub-Saharan Africa and described in Indian urban children on low-calcium diets), X-linked hypophosphataemic rickets (the most common hereditary form — X-linked dominant, loss of PHEX enzyme activity leading to elevated FGF23 and renal phosphate wasting, producing hypophosphataemia without vitamin D deficiency), and vitamin D-dependent rickets types I and II (rare enzyme/receptor mutations). The age of presentation and pattern of deformity relates to the skeletal stresses applied when the disease is most active: crawling age leads to genu varum (bow legs); standing/toddling age produces variable genu varum or genu valgum; older children predominantly develop genu valgum (knock knees). This explains why the same pathology produces different deformities at different ages.
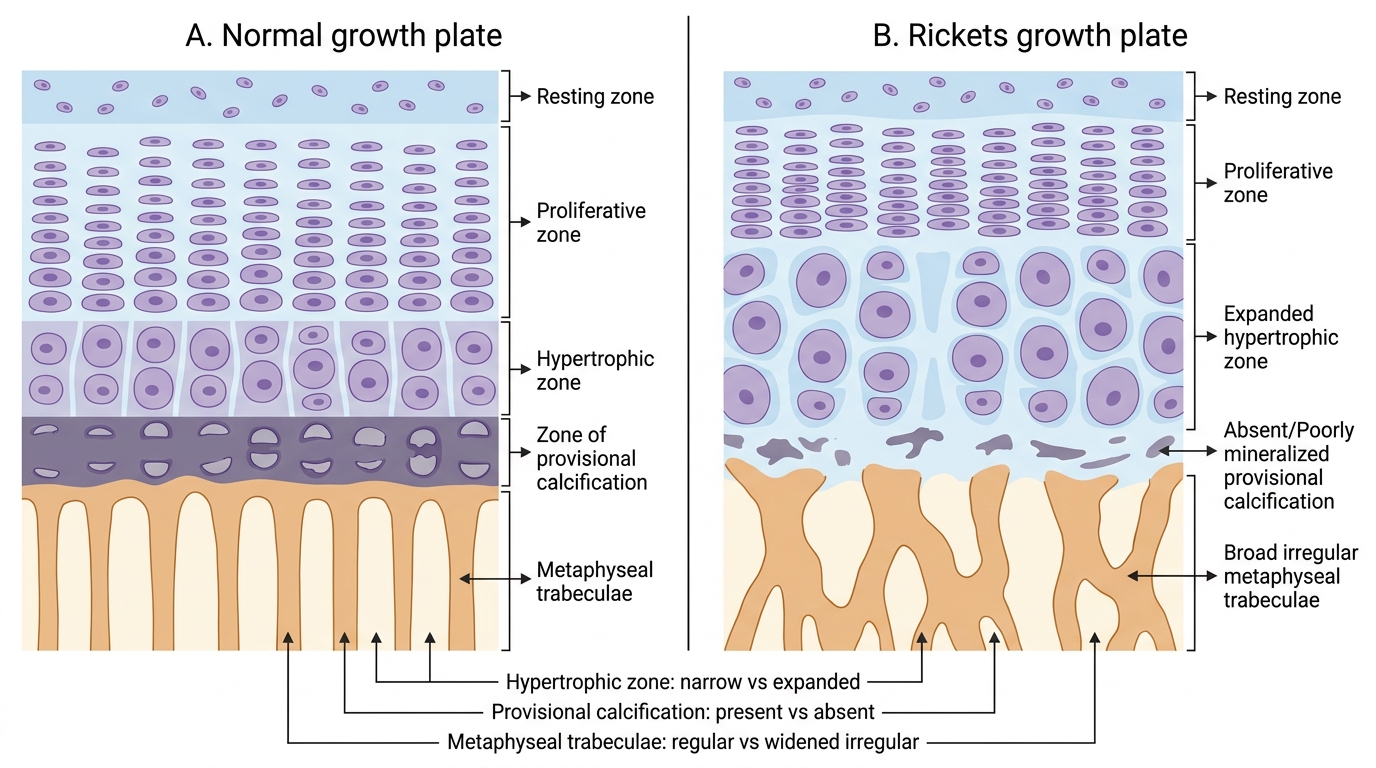
Growth Plate Histology in Rickets