Page 2 of 12
OR7.1 | Metabolic Bone Disease Assessment — SDL Guide (Part 2)
Rickets: Clinical Features, Deformities, and Radiological Signs
The clinical presentation of active rickets encompasses skeletal, muscular, and systemic features. The child is irritable, growth-retarded, and hypotonic. Systematic examination reveals a constellation of characteristic signs whose anatomical locations correspond to the sites of most rapid bone growth and highest metabolic demand. At the cranium: craniotabes (ping-pong ball sensation on pressing the occipital and posterior parietal bones — due to demineralised skull) is the earliest sign in infants; frontal and parietal bossing (squarish skull from subperiosteal osteoid accumulation) appears later. At the chest: the rachitic rosary is a beading or nodular enlargement at the costochondral junctions of ribs 3-9, palpable and sometimes visible as a row of rounded prominences along each side of the sternum — it represents widened, irregular costochondral cartilage. The chest wall may develop a Harrison's sulcus — a horizontal groove along the lower thorax corresponding to the line of diaphragm pull on softened ribs. At the wrist: widening of the metaphyses produces clinically palpable and radiologically visible widened, cupped, and frayed (irregular) metaphyseal flaring at the distal radius and ulna — the rachitic wrist is a pathognomonic sign. At the lower limbs: genu varum (bow legs, varus knee deformity) is the classic deformity in infants who bear weight during the active phase of disease; genu valgum (knock knees, valgus) predominates in older children. These deformities are biomechanically progressive — once the bone softens, the combined forces of gravity and muscle pull incrementally worsen the angular deformity. Additional features include delayed dentition (vitamin D is required for normal odontoblast function and enamel mineralisation) and hypocalcaemic tetany in severe cases (carpopedal spasm, Chvostek's sign, Trousseau's sign).
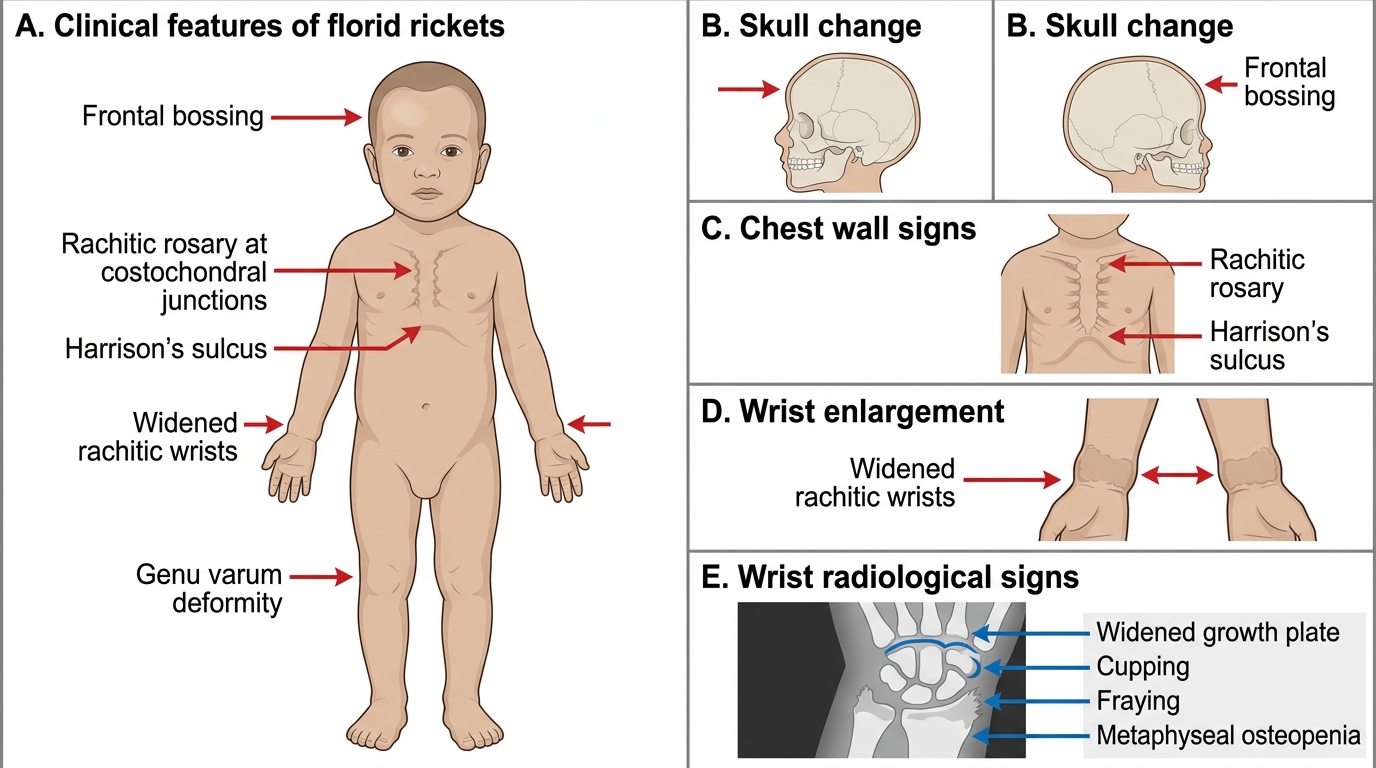
Florid Rickets: Clinical and Wrist Radiological Features
Radiological features of rickets at the wrist (the most informative site) are: widened growth plate (increased physeal width), cupped and frayed metaphysis (irregular concave metaphyseal margin replacing the normal smooth convex contour), and decreased density of metaphyseal bone. Long bones appear osteopenic with thinned cortices. Greenstick fractures through softened shafts may occur. The biochemical profile mirrors osteomalacia: low calcium, low phosphate, elevated ALP (very high — typically 3-10 times normal in active rickets), elevated PTH, and low 25-hydroxyvitamin D in nutritional vitamin D deficiency rickets.
Paget's Disease of Bone: Aetiopathogenesis and Pathophysiology
Paget's disease of bone (osteitis deformans) is a focal disorder of bone remodelling characterised by markedly accelerated and disorganised osteoclastic resorption followed by equally accelerated but structurally chaotic osteoblastic new bone formation. The result is bones that are enlarged, hypervascular, mechanically weak despite their increased mass, and prone to deformity, fracture, nerve compression, and malignant transformation. The aetiology remains incompletely understood, but current evidence supports a viral trigger (paramyxovirus, possibly measles or respiratory syncytial virus) in genetically predisposed individuals: mutations in the SQSTM1/p62 gene (sequestosome-1, an NF-kB scaffold) are found in 10-15% of familial cases and confer susceptibility by dysregulating osteoclast activation. The disease is focal — any bone can be involved, but the most common sites are the pelvis (most common, approximately 70% of cases), lumbar spine, skull, femur, and tibia. It is rare below age 40 and affects men slightly more than women. The natural history passes through three phases: an initial lytic phase (osteoclasts predominate, producing expanding lytic fronts called 'blade of grass' in long bones, or 'osteoporosis circumscripta' in the skull); a mixed active phase (simultaneous intense osteoclastic and osteoblastic activity — the most symptomatic); and a sclerotic phase (bone formation predominates, producing dense, expanded, architecturally disorganised bone with a characteristic coarsened trabecular pattern and cortical thickening).
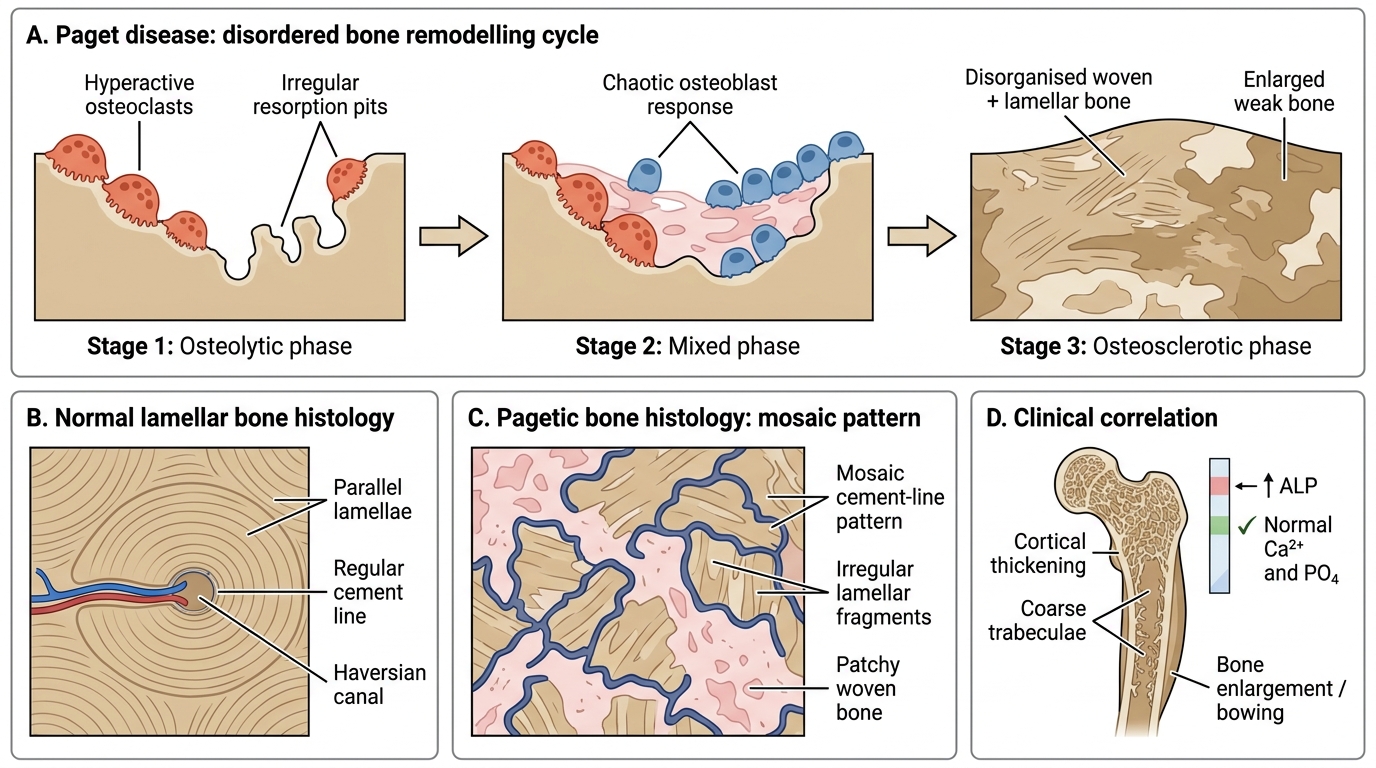
Paget Disease: Disordered Bone Remodeling and Mosaic Histology
SELF-CHECK
A 45-year-old woman has diffuse hip and thigh pain with waddling gait. Investigations show serum calcium 8.0 mg/dL, serum phosphate 2.1 mg/dL, ALP 380 U/L, PTH elevated, 25-hydroxyvitamin D 8 ng/mL. X-ray shows translucent bands perpendicular to the cortex at the medial femoral necks bilaterally. Which diagnosis fits and what are those X-ray findings called?
A. Osteoporosis — compression fractures
B. Osteomalacia — Looser's zones (pseudofractures)
C. Paget's disease — cotton-wool skull appearance
D. Primary hyperparathyroidism — subperiosteal resorption
Reveal Answer
Answer: B. Osteomalacia — Looser's zones (pseudofractures)
This is osteomalacia. The biochemical fingerprint is low Ca, low PO4, elevated ALP, elevated PTH, and very low vitamin D. The translucent bands perpendicular to cortex at sites of stress (medial femoral neck, pubic rami) are Looser's zones — pathognomonic of osteomalacia, representing accumulations of unmineralised osteoid. Osteoporosis shows normal biochemistry. Paget's shows elevated ALP with normal calcium and phosphate. Primary hyperparathyroidism shows elevated calcium, low phosphate, and subperiosteal erosions of the radial aspect of middle phalanges.
Osteoporosis: Investigations and Management
Provided image
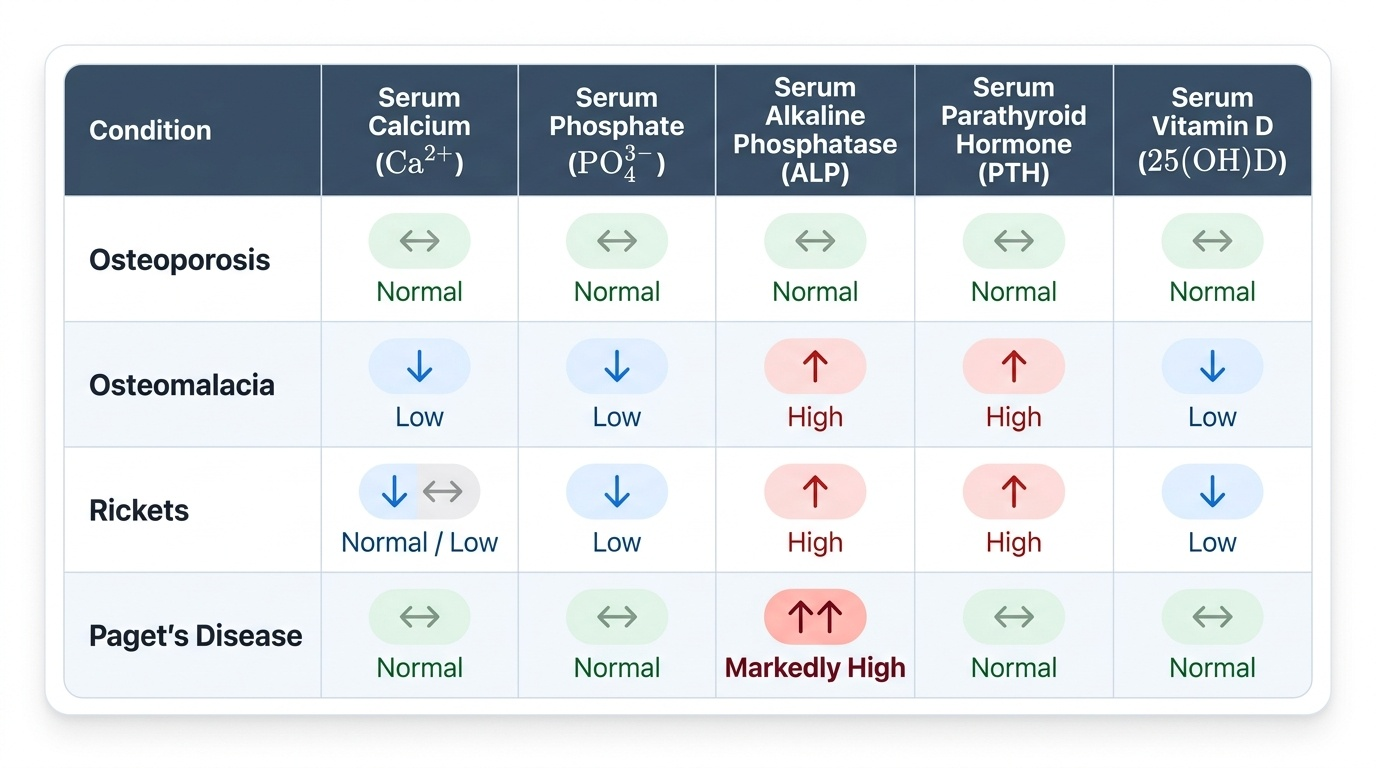
The biochemical hallmark of osteoporosis is its normalcy: serum calcium, phosphate, ALP, PTH, and vitamin D are all within normal limits in primary osteoporosis. This distinguishing feature separates it from osteomalacia (where calcium and phosphate are low and ALP is high). DEXA scanning is the investigation of choice, performed at the lumbar spine and hip (both femoral neck and total hip). The T-score at the lowest-value site is used for diagnosis. The FRAX tool (Fracture Risk Assessment Tool, WHO) integrates multiple clinical risk factors — age, sex, BMD, body mass index, prior fracture, parental hip fracture, smoking, alcohol, glucocorticoid use, rheumatoid arthritis, and secondary osteoporosis — to calculate the 10-year probability of major osteoporotic fracture and hip fracture, guiding treatment decisions. Baseline blood tests are essential to exclude secondary causes (thyroid function, parathyroid hormone, serum protein electrophoresis to exclude myeloma, testosterone in men, serum calcium and phosphate to exclude osteomalacia, renal function).
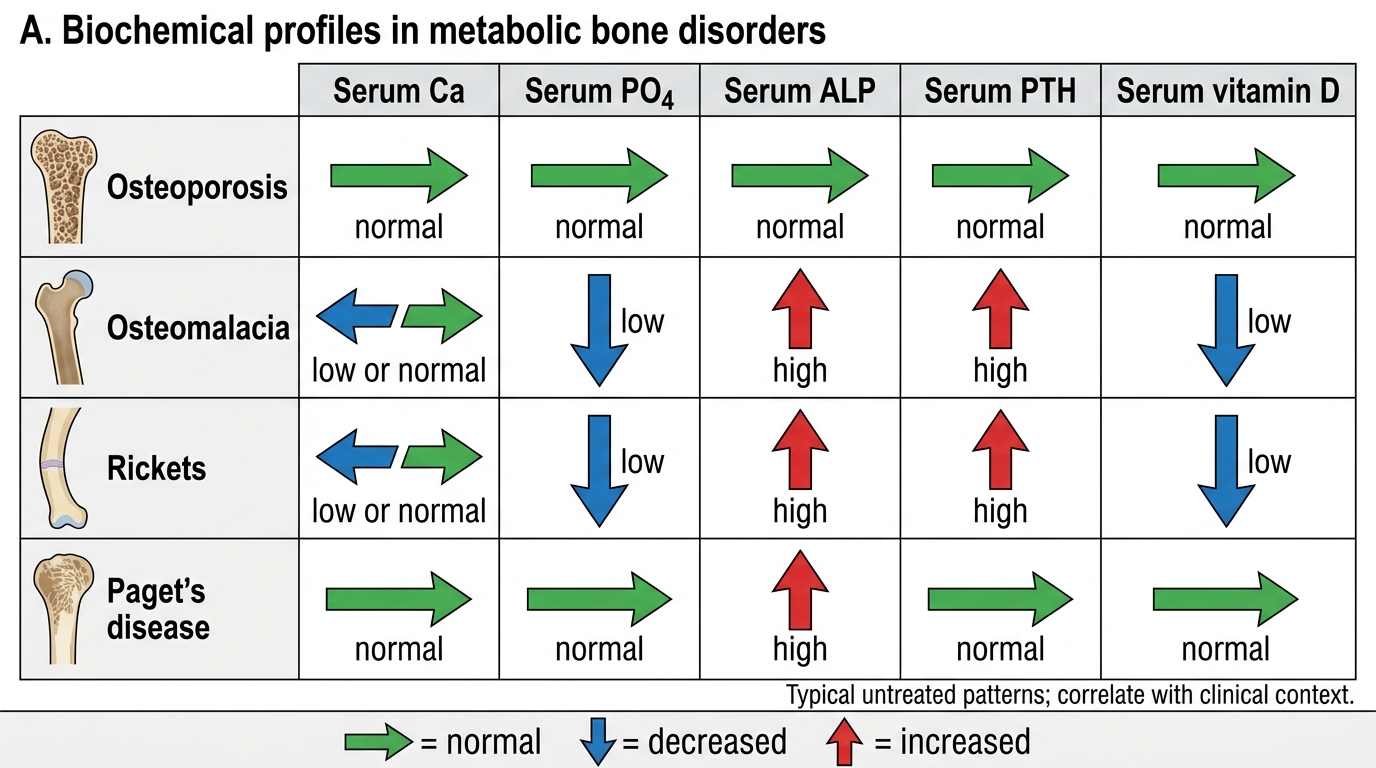
Biochemical Profiles in Metabolic Bone Disorders
Management of osteoporosis is tripartite: non-pharmacological (weight-bearing exercise, fall prevention — hip protectors, home safety modifications, balance training; adequate calcium intake 1000-1200 mg/day, vitamin D supplementation 800-1000 IU/day), anti-resorptive pharmacotherapy (bisphosphonates — alendronate 70 mg weekly orally or zoledronic acid 5 mg IV annually — are first-line; they inhibit osteoclast activity by blocking the mevalonate pathway; adverse effects include oesophagitis with oral agents, flu-like reaction with IV agents, and rare osteonecrosis of the jaw; RANKL inhibitors — denosumab 60 mg subcutaneously every 6 months — are an alternative), and anabolic agents (teriparatide, a recombinant PTH fragment, stimulates new bone formation and is reserved for severe osteoporosis with multiple fractures). Oestrogen replacement therapy is effective for prevention in post-menopausal women but carries risks of breast cancer, venous thromboembolism, and endometrial carcinoma, so is not first-line for osteoporosis alone.