Page 5 of 15
OR9.1 | Cerebral Palsy Orthopaedic Assessment — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis of cerebral palsy (CP) and distinguish upper motor neurone spastic paralysis from the lower motor neurone flaccid paralysis of PPRP
- Classify CP by motor type (spastic, dyskinetic, ataxic), topographic distribution (hemiplegia, diplegia, quadriplegia), and functional severity (GMFCS levels I–V)
- Assess the orthopaedic consequences of spasticity — dynamic and fixed contractures, lever-arm dysfunction, and progressive bony deformity
- Explain the multidisciplinary management of CP including physiotherapy, spasticity management (botulinum toxin, selective dorsal rhizotomy), and orthopaedic surgery (soft-tissue releases, osteotomies)
- Distinguish dynamic (spastic) deformity from fixed structural deformity and select the appropriate intervention for each
INSTRUCTIONS
Cerebral palsy is the most common cause of motor disability in childhood worldwide, affecting approximately 2–3 per 1,000 live births. In India, with its high rate of birth asphyxia, neonatal infections, and premature deliveries, the burden is substantial. Orthopaedic management of CP is among the most complex in paediatric surgery: the primary brain lesion is static, but its musculoskeletal consequences are progressive and evolving throughout skeletal growth. As a final-year student you must understand the UMN-spastic mechanism, classify CP accurately, perform a systematic orthopaedic assessment, and know when to use botulinum toxin versus surgery versus observation. This SDL builds directly on the PPRP SDL — the contrast between LMN-flaccid (polio) and UMN-spastic (CP) is a recurring examination theme and a fundamental clinical distinction.
References
- Maheshwari's Essential Orthopaedics, Ch on Cerebral Palsy (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Ch on Cerebral Palsy (textbook)
- Ebnezar's Textbook of Orthopaedics, Ch on Cerebral Palsy (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 7-year-old boy is brought by his parents to the orthopaedic outpatient department. He was born at 32 weeks of gestation following an emergency caesarean for foetal distress, required ventilatory support for 5 days, and has been delayed in all motor milestones. He walks with a scissor gait — hips adducted and internally rotated, knees slightly flexed and crossing each other with each step, and both feet in equinus. His deep tendon reflexes are brisk bilaterally and both plantar responses are extensor. His parents have been told by a neurologist that he has 'cerebral palsy' but want to know what can be done for his walking. How do you classify his CP, assess his deformity, and plan management?
WHY THIS MATTERS
Cerebral palsy is the leading cause of childhood physical disability. Every orthopaedic surgeon in India will encounter CP patients across the full spectrum — from the ambulatory child with mild hemiplegia to the non-ambulant teenager with severe spastic quadriplegia and painful hip dislocation. The orthopaedic surgeon is a core member of the multidisciplinary team, responsible for managing the progressive musculoskeletal consequences of a static brain lesion: spastic contractures, lever-arm dysfunction, progressive joint deformity, and hip dislocation. Timely, evidence-based decisions — botulinum toxin at the right age, selective dorsal rhizotomy in the right candidate, single-event multilevel surgery at the right time — can transform a child's functional trajectory. Missing these windows condemns the child to an increasingly severe deformity spiral. This SDL also completes the neuromuscular pair by establishing the UMN-spastic contrast with the LMN-flaccid PPRP SDL.
RECALL
Before proceeding, recall the following: (1) The upper motor neurone (UMN) pathway — from the motor cortex through the internal capsule, brainstem, and corticospinal tract to the anterior horn cell — and the clinical consequences of UMN lesions: spastic tone (velocity-dependent increase in resistance to passive stretch), hyperreflexia, extensor plantar response (Babinski sign), and clonus. (2) The difference between spasticity (velocity-dependent tonic stretch reflex) and rigidity (lead-pipe, not velocity-dependent — a feature of extrapyramidal disease). (3) The concept of dynamic deformity (present only during activity, correctable at rest) vs fixed structural deformity (present at rest, not correctable passively). (4) From the PPRP SDL: LMN features — flaccid, wasting, absent reflexes, intact sensation — now contrast these directly with the UMN features of CP.
Clinical Presentation and Classification of Cerebral Palsy
Cerebral palsy is defined as a group of permanent, non-progressive disorders of movement and posture resulting from a lesion or anomaly occurring in the immature brain during fetal development, birth, or the perinatal period. The brain lesion is static — it does not progress after the initial insult — but its orthopaedic and functional consequences are dynamic and worsen through childhood skeletal growth, making CP a progressive musculoskeletal problem superimposed on a static neurological one. This distinction is essential to understand and to communicate clearly to families: when parents are told their child's CP is 'non-progressive' or 'static,' they must not conclude that the child's deformities or functional limitations will stay the same — they often worsen considerably without proactive intervention. The clinician's role is to manage the progressive musculoskeletal consequences of a brain that will not change.
Classification of CP is essential for planning management and predicting prognosis. Three axes are used:
Axis 1 — Motor type (the dominant neurological abnormality):
- Spastic CP (most common, ~75–80%): UMN lesion producing velocity-dependent increased tone (spasticity), hyperreflexia, Babinski sign, and scissor gait. The primary pathological substrate is damage to the corticospinal tracts — most commonly periventricular leukomalacia (PVL) in premature infants.
- Dyskinetic CP (~10–15%): Basal ganglia / extrapyramidal lesion producing involuntary movements — athetosis (slow writhing), chorea (rapid jerky), or dystonia (sustained abnormal postures). Often follows acute perinatal asphyxia (hypoxic-ischaemic encephalopathy, HIE) in term infants. Tone fluctuates — may be hypotonic at rest and hypertonic with effort.
- Ataxic CP (~5%): Cerebellar lesion producing incoordination, wide-based gait, intention tremor, dysmetria, and hypotonia. Often congenital cerebellar malformation.
- Mixed types: Combinations of the above, most commonly spastic-dyskinetic.
Axis 2 — Topographic distribution (which limbs are affected):
- Hemiplegia: One side (arm + leg), usually from a unilateral cortical or subcortical lesion
- Diplegia: Both legs predominantly, arms minimally — the classic pattern of prematurity-related PVL
- Quadriplegia / total body involvement: All four limbs and trunk severely affected; usually with intellectual disability, epilepsy, and feeding difficulties
- Monoplegia / triplegia: Rare variants
Axis 3 — Gross Motor Function Classification System (GMFCS I–V): Validated 5-level functional classification of real-world mobility:
- Level I: Walks without limitation
- Level II: Walks with limitations (stairs need handrail, uneven surfaces difficult)
- Level III: Walks using a hand-held mobility device
- Level IV: Self-mobility limited; powered wheelchair used
- Level V: Transported in a manual wheelchair; very limited self-mobility
GMFCS level is the single most important predictor of functional prognosis, guides surgical decision-making, and directs rehabilitation goals. GMFCS levels I–III are typically ambulatory (with or without aids); levels IV–V are non-ambulatory.
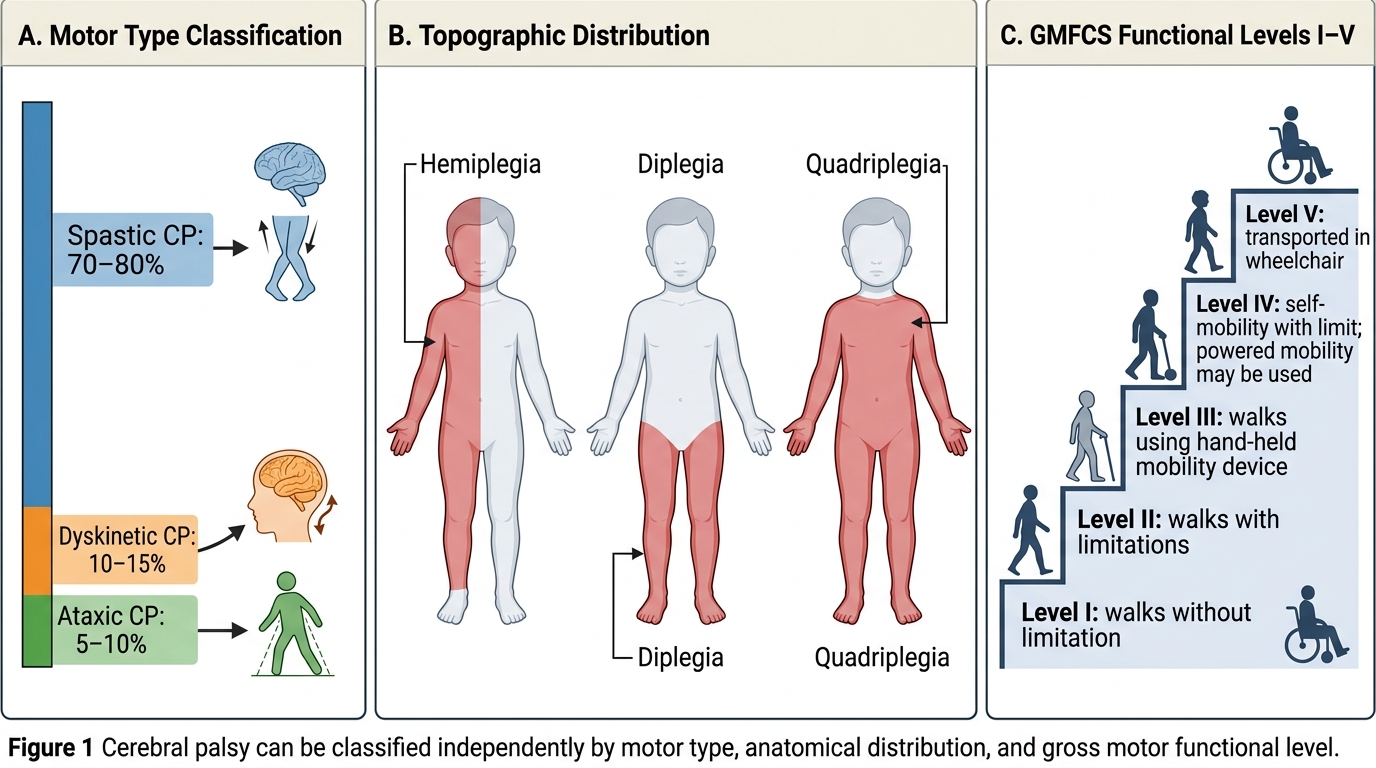
Classification of Cerebral Palsy
Aetiopathogenesis: UMN Lesion, Spasticity, and Progressive Deformity
The causal brain lesion in CP occurs during the period of brain vulnerability — from conception through approximately 2 years of age, though most clinically significant lesions occur perinatally. Three major pathological patterns are recognised, each with characteristic timing and brain substrate:
1. Periventricular leukomalacia (PVL) — the dominant lesion of prematurity: Watershed ischaemia in the periventricular white matter, particularly affecting the corticospinal fibres supplying the lower limbs (which run most medially, closest to the ventricles). This explains why premature infants develop predominantly spastic diplegia — the leg-related corticospinal fibres are disproportionately damaged. The arms are relatively spared because their corticospinal fibres lie more laterally.
2. Hypoxic-ischaemic encephalopathy (HIE) — the dominant lesion of term asphyxia: Global or watershed cortical injury in term infants following perinatal asphyxia (prolonged labour, cord prolapse, placental abruption, meconium aspiration). Basal ganglia and thalamic injury produces the dyskinetic-dystonic pattern; diffuse cortical injury produces spastic quadriplegia with associated intellectual disability.
3. Intracranial haemorrhage / infection: Periventricular haemorrhage in preterm infants; bacterial meningitis, neonatal sepsis, or viral encephalitis in the postnatal period. Unilateral lesions → hemiplegia; bilateral → diplegia or quadriplegia.
Common risk factors for CP in the Indian context include prematurity, birth asphyxia (Apgar score <3 at 5 minutes), neonatal hyperbilirubinaemia (kernicterus — classically causes dyskinetic CP), neonatal meningitis, and intrauterine infections (TORCH — toxoplasmosis, rubella, CMV, herpes).
Pathomechanism of deformity in spastic CP — the 'spasticity spiral': The primary UMN lesion releases the stretch reflex from supraspinal inhibition, producing spasticity. Sustained spasticity has two consequences: (a) during gait, the spastic muscle is continuously activated, producing dynamic deformity (e.g. equinus during swing phase); (b) over months to years, the spastic muscle grows shorter than the lengthening bone it crosses — producing a fixed contracture (structural, not correctable passively). Fixed contractures then drive secondary bony deformities: femoral anteversion, tibial torsion, coxa valga, hip subluxation, and eventually hip dislocation. This progression from spasticity → dynamic deformity → fixed contracture → bony deformity is the central concept explaining why CP management is time-sensitive and must keep pace with skeletal growth.
Critical distinction from PPRP: In CP the brain lesion produces a UMN syndrome — tone is INCREASED (spastic), reflexes are BRISK and PATHOLOGICAL (Babinski positive, clonus), and sensation is largely intact. Wasting is minimal because the lower motor neurone and muscle are intact. This contrasts sharply with PPRP where tone is absent, reflexes are absent, wasting is prominent, and sensation is normal for a different reason (the motor neurone is destroyed, not a separate sensory system).
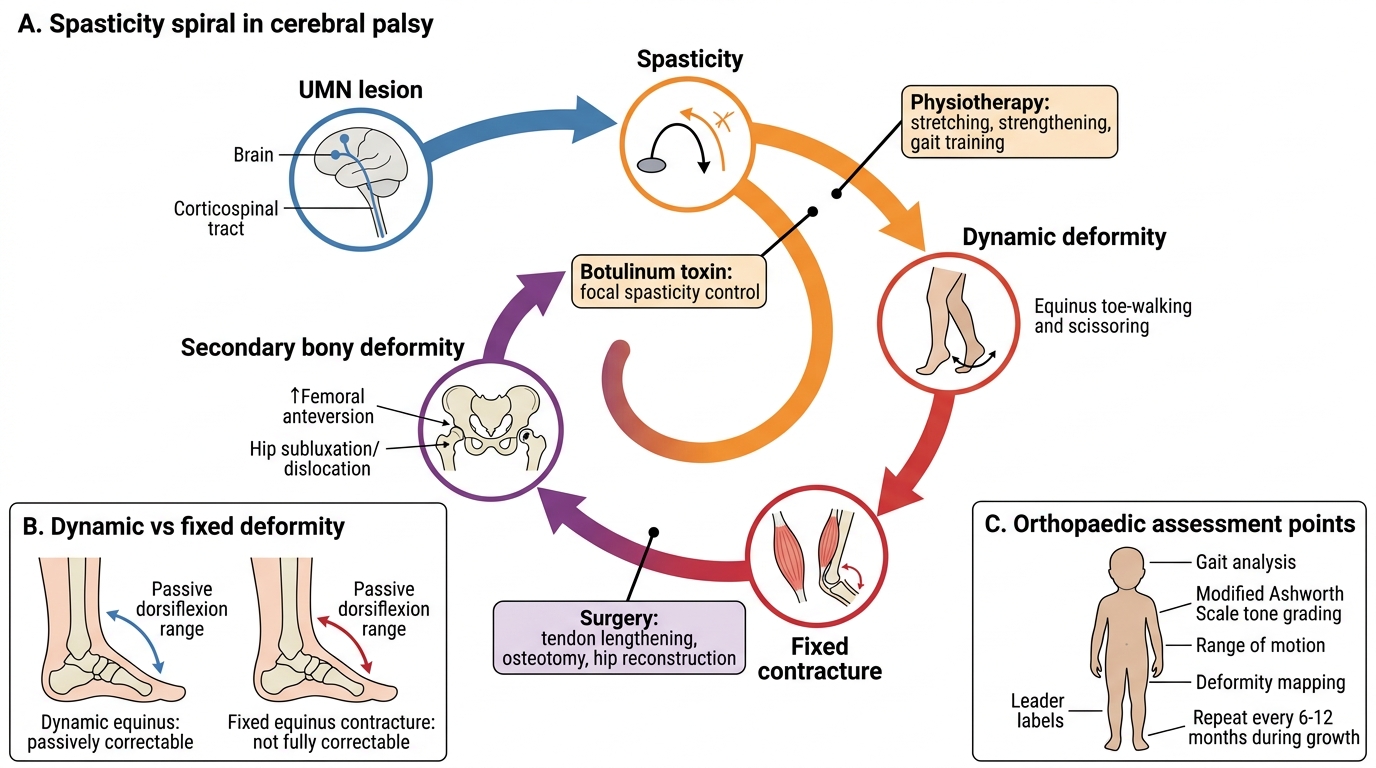
Spasticity Spiral in Cerebral Palsy
Orthopaedic Assessment: Gait Analysis, Spasticity Grading, and Deformity Mapping
Orthopaedic assessment of a child with CP must be systematic, comprehensive, and repeated at regular intervals (every 6–12 months) because the deformity picture changes with growth. The assessment addresses neurological status, muscle spasticity, joint range of motion, deformity characterisation (dynamic vs fixed), functional level, and gait pattern. This data drives the management plan.
History: Gestational age and birth history (prematurity, Apgar scores, NICU stay, jaundice, meningitis); developmental milestones (motor milestones are the most relevant — sitting, standing, walking); comorbidities (intellectual disability, epilepsy, visual/hearing impairment, feeding difficulties); prior interventions (botulinum toxin, plaster serial casting, previous surgery); current functional status and GMFCS level; school participation and activities of daily living.
Spasticity grading: The Modified Ashworth Scale (MAS) is the standard clinical tool:
- MAS 0: No increase in tone
- MAS 1: Slight increase with a catch at end of range
- MAS 1+: Slight increase through less than half the range
- MAS 2: More marked increase, but joint easily moved
- MAS 3: Considerable increase, passive movement difficult
- MAS 4: Rigid in flexion or extension
Dynamic vs fixed deformity — the critical distinction: A dynamic deformity is present during activity (gait, standing) but corrects passively at rest. It is caused by spasticity alone — the spastic muscle is overactive but not structurally shortened. A fixed deformity cannot be corrected passively under any circumstances; it results from true soft-tissue contracture or bony change. The distinction matters enormously for treatment selection: dynamic deformity responds to spasticity management (botulinum toxin, orthotics, physiotherapy); fixed deformity requires surgical correction.
Hip surveillance — essential in all CP patients: Hip displacement is the most common and most serious orthopaedic complication of CP. The spastic adductors continuously pull the femoral head out of the acetabulum. Hip migration percentage (Reimers index: percentage of femoral head uncovered by the acetabulum on AP pelvis X-ray) is the standard measure:
- <25%: Normal
- 25–50%: Hip at risk — regular surveillance, consider intervention
- >50%: Subluxation — surgical intervention
- 100%: Complete dislocation
Lower-limb deformity assessment in the ambulatory child:
- Hip: Adduction (Thomas test for flexion contracture), internal rotation (prone hip rotation — femoral anteversion), Trendelenburg test for abductor weakness
- Knee: Fixed flexion deformity (popliteal angle for hamstring tightness), recurvatum, crouch gait
- Foot and ankle: Equinus (gastrosoleus spasticity/contracture — Silfverskiöld test distinguishes gastrocnemius-only tightness from combined gastrosoleus tightness); valgus hindfoot; hallux valgus
Gait patterns in spastic CP:
- True equinus: Gastrosoleus spasticity, toe-walking throughout stance
- Jump gait: Hip flexion + knee flexion + equinus — looks 'crouched' with toe-walking
- Crouch gait: Hip + knee flexion with ankle dorsiflexion (over-lengthened Achilles or hamstring dominance) — energy inefficient
- Scissor gait: Hip adduction and internal rotation producing a cross-legged walk — hip adductor spasticity
Imaging: AP pelvis (Reimers index, coxa valga, hip dysplasia); long-leg AP (tibial/femoral torsion); foot X-rays; brain MRI to characterise the lesion (not required for orthopaedic management decisions but guides prognosis).
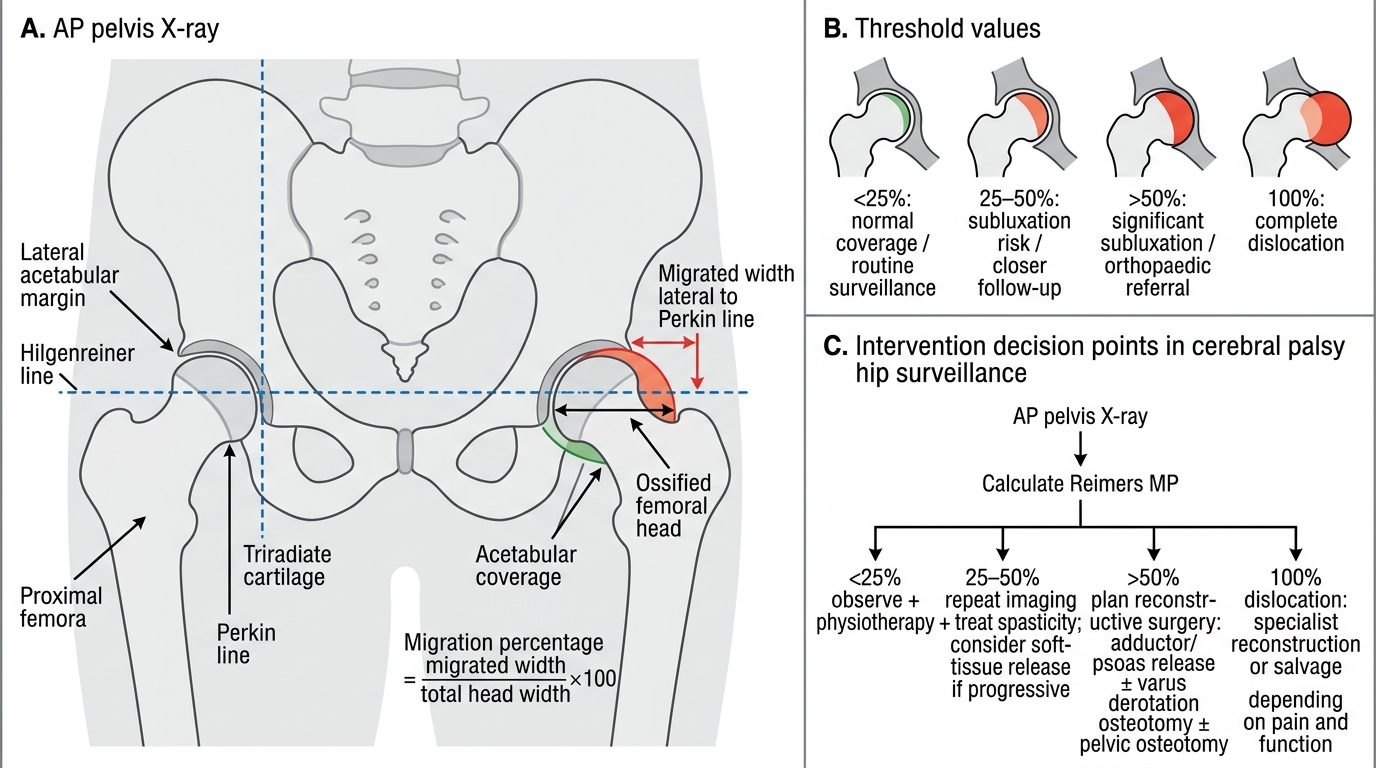
Reimers Migration Percentage on AP Pelvis X-ray
SELF-CHECK
A 5-year-old with spastic diplegia CP has dynamic equinus on gait but full passive dorsiflexion at rest with the knee extended. The gastrocnemius is spastic (MAS 2) but the soleus is not tight. The Silfverskiöld test is positive. Which intervention is most appropriate at this stage?
A. Achilles tendon lengthening (surgical) — to correct the equinus permanently
B. Botulinum toxin injection into gastrocnemius — to reduce dynamic spasticity
C. Triple arthrodesis — to stabilise the foot in plantargrade position
D. Ankle-foot orthosis alone — spasticity management is not needed yet
Reveal Answer
Answer: B. Botulinum toxin injection into gastrocnemius — to reduce dynamic spasticity
This child has DYNAMIC equinus (correctable passively at rest) caused by isolated gastrocnemius spasticity — a classic indication for botulinum toxin A injection. The Silfverskiöld test confirming isolated gastrocnemius tightness (equinus corrects with knee flexed but not with knee extended) supports targeting the gastrocnemius specifically. Surgical Achilles lengthening at age 5 risks over-lengthening and crouch gait as the child grows — it is better reserved for fixed contractures or after failed conservative management in older children. Triple arthrodesis requires skeletal maturity and is for rigid hindfoot deformity. AFO alone does not address the underlying spasticity driving the deformity.