Page 6 of 15
OR9.1 | Cerebral Palsy Orthopaedic Assessment — SDL Guide (Part 2)
Multidisciplinary Management: Physiotherapy, Spasticity Management, and Orthotics
Management of CP is lifelong, multidisciplinary, and must be matched to the child's GMFCS level, age, and the phase of the deformity spiral. The team includes the orthopaedic surgeon, paediatric neurologist, physiotherapist, occupational therapist, speech and language therapist, orthotist, and social worker. No single specialist manages CP alone; the orthopaedic surgeon's role is to address the musculoskeletal consequences of spasticity in coordination with the rest of the team.
Physiotherapy is the backbone of all levels of CP management. Goals include maintaining range of motion, strengthening functional muscle groups, preventing contracture, improving gait pattern, and maximising independence. Specific programmes — neurodevelopmental therapy (NDT/Bobath approach), task-oriented training, constraint-induced movement therapy (CIMT) for hemiplegic upper limbs — are prescribed based on GMFCS level and the child's specific deficits. Physiotherapy alone cannot reverse established spasticity or contractures, but it slows progression and maintains the gains from surgical and pharmacological interventions.
Orthotics:
- Ankle-foot orthosis (AFO): The most widely used orthosis in CP; holds the ankle at 90° to prevent equinus during stance, support the weak ankle in swing, and stretch the gastrosoleus during static standing. Polypropylene solid AFO for dynamic equinus; hinged/articulated AFO for crouch gait.
- Knee-ankle-foot orthosis (KAFO): For severe knee flexion deformities or in non-ambulatory patients for standing frame use.
- Night splints: Worn during sleep to provide prolonged stretch and slow contracture progression between physiotherapy sessions.
- Hand orthoses and upper limb splints: For hemiplegic CP — maintain wrist/thumb position, facilitate function.
Botulinum toxin A (BoNT-A) injections: The single most important pharmacological tool in ambulatory CP management. BoNT-A, injected intramuscularly under EMG or ultrasound guidance, temporarily blocks acetylcholine release at the neuromuscular junction, producing a focal chemical denervation that reduces spasticity for 3–6 months. Key uses:
- Gastrocnemius (dynamic equinus) — the most common indication
- Hip adductors (scissor gait / hip at risk)
- Hamstrings (crouch gait)
- Upper limb (wrist/thumb flexors in hemiplegic CP)
Prerequisites for BoNT-A success: dynamic (not fixed) deformity; child ambulatory or with some functional goal; combined with physiotherapy and orthotics post-injection. Repeated injections every 3–6 months in growing children buy time before irreversible structural changes mandate surgery.
Oral spasticity medications (less commonly used in CP): Baclofen (GABA-B agonist — muscle relaxant, sedating), diazepam (useful in dystonic crisis), tizanidine. Intrathecal baclofen (ITB) pump delivers baclofen directly into the cerebrospinal fluid via an implanted pump, producing profound spasticity reduction with less systemic sedation — reserved for severe spastic or mixed CP (GMFCS IV–V).
Selective dorsal rhizotomy (SDR): A neurosurgical procedure (performed by the neurosurgeon) that selectively cuts afferent sensory rootlets of the lumbosacral spinal cord that are generating the abnormal stretch reflex drive. Produces permanent, irreversible reduction of lower limb spasticity. Strict criteria: spastic diplegia, GMFCS II–III, age 4–7 years, adequate strength and selective motor control, no fixed contractures. Must be followed by 12–24 months of intensive physiotherapy.
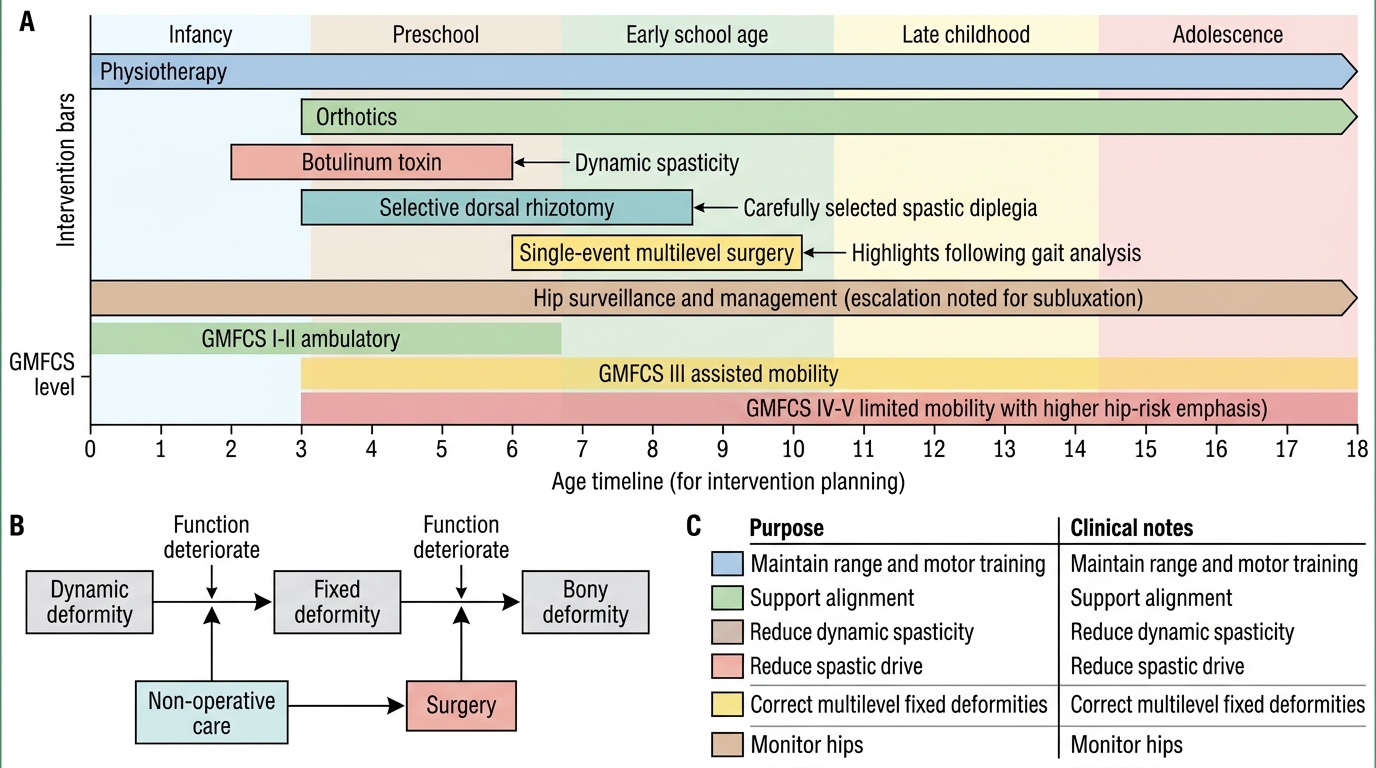
Intervention Timeline in Cerebral Palsy
Orthopaedic Surgery in CP: Soft-Tissue Procedures, Osteotomies, and Hip Management
Provided image
Orthopaedic surgery in CP is indicated when non-operative measures (physiotherapy, orthotics, botulinum toxin) fail to prevent fixed deformity, when fixed deformities produce functional deterioration, or when bony deformities (torsion, coxa valga, hip subluxation) require correction. The modern surgical philosophy for ambulatory CP is single-event multilevel surgery (SEMLS) — correcting all functional deformities in one anaesthetic episode (typically age 6–10 years, after gait analysis), rather than staged serial operations that interrupt schooling and rehabilitation.
Surgery is classified by level and by type: soft-tissue (lengthening, transfer) versus bony (osteotomy, arthrodesis). In CP, unlike PPRP, the goal of tendon surgery is usually LENGTHENING of an overactive spastic muscle, not transfer of a weak one — the neurological problem is excess tone, not paralysis. The muscle-bone mismatch (bone grows faster than spastic muscle) is corrected by lengthening the musculotendinous unit to restore normal length-tension relationships.
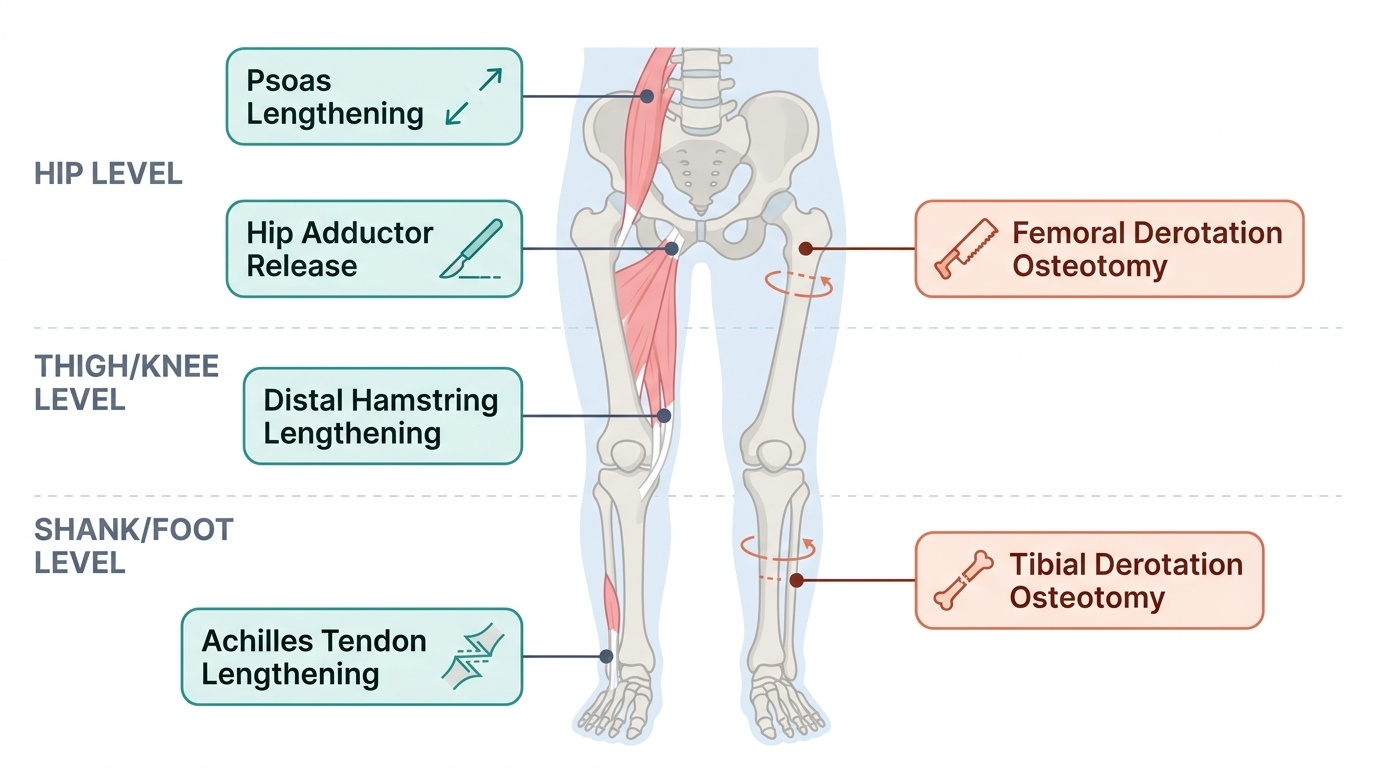
Lower-limb soft-tissue procedures:
- Achilles tendon lengthening (TAL) / gastrocnemius recession: For fixed equinus contracture — Achilles tendon lengthening (Hoke, Vulpius) or Strayer gastrocnemius recession. Risk of over-lengthening producing calcaneus and crouch gait — use judiciously, measure carefully
- Hip adductor release: Adductor longus tenotomy ± gracilis release for scissor gait, hip at risk, or after hip reduction
- Psoas (iliopsoas) lengthening: For hip flexion contracture causing anterior pelvic tilt and crouch gait
- Distal hamstring lengthening: For knee flexion deformity / crouch gait; medial hamstring release ± gracilis and sartorius
- Rectus femoris transfer: Rectus femoris detached from patella and transferred to sartorius or gracilis — converts a knee extensor that fires in swing (producing stiff-knee gait) into a hip flexor
Bony procedures:
- Derotation osteotomy of femur: Corrects femoral anteversion (internal rotation gait); performed at subtrochanteric level with plate fixation
- Derotation osteotomy of tibia: Corrects tibial torsion (usually external in CP) — supramalleolar osteotomy
- Foot osteotomies: Calcaneal lengthening (Evans) or medialising calcaneal osteotomy for valgus flatfoot; lateral column lengthening for severe pes planovalgus
- Bony hip procedures: Varus derotation osteotomy (VDRO) of the femur to correct coxa valga and reduce hip; Dega / Pemberton acetabuloplasty to redirect the acetabulum for better coverage
Hip dislocation management in non-ambulatory CP (GMFCS IV–V):
The hip at risk must be caught early using surveillance X-rays (every 6–12 months). A migration percentage of 25–50% warrants soft-tissue releases (adductor, psoas). Migration >50% warrants bony reconstruction (VDRO + acetabuloplasty). Complete dislocation with pain warrants either reconstruction (if feasible) or salvage procedures (Schanz osteotomy, proximal femoral resection) for pain relief.
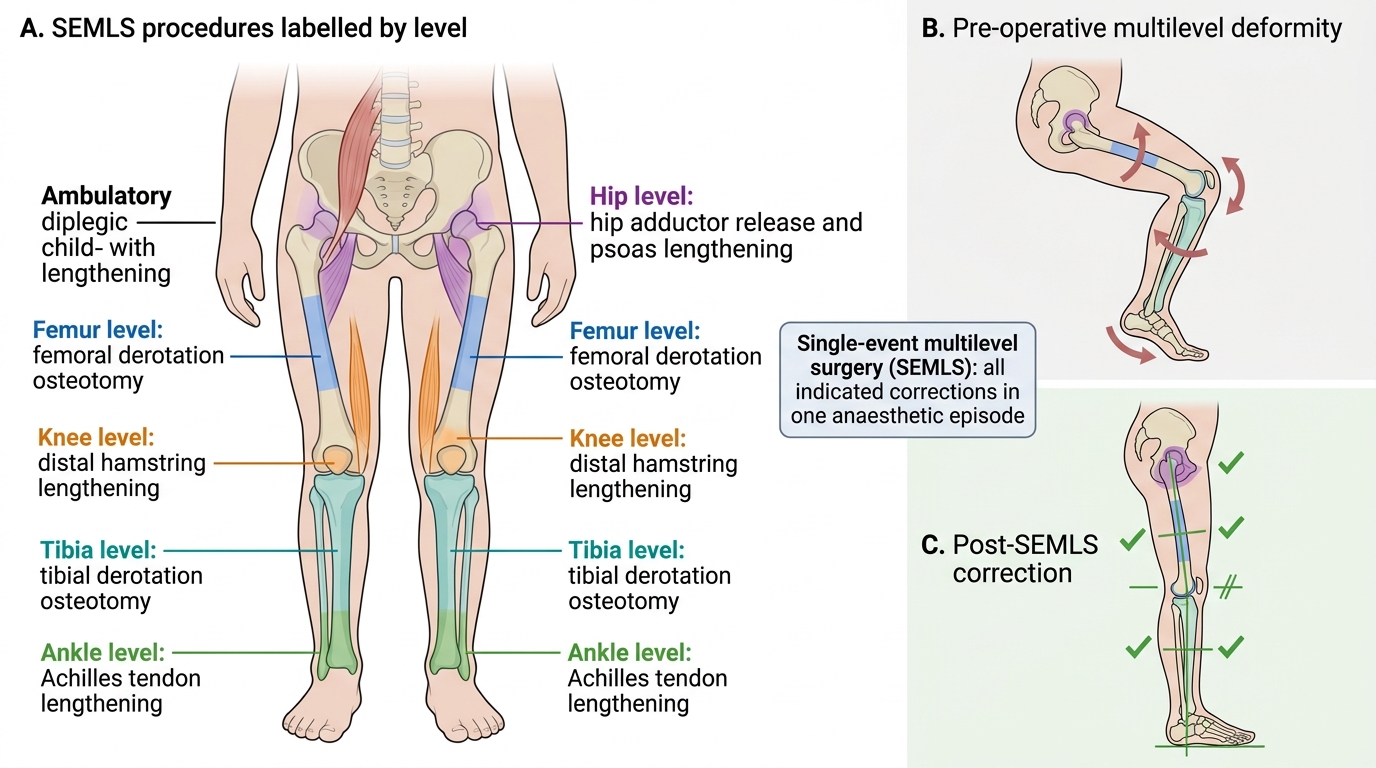
Single-Event Multilevel Surgery in Diplegic Cerebral Palsy
SELF-CHECK
An 8-year-old boy with spastic diplegia (GMFCS level II) is assessed with gait analysis. He has femoral anteversion 40°, hip adductor spasticity MAS 2, knee crouch with popliteal angle 50°, and dynamic equinus that has progressed to a 10° fixed equinus contracture. Botulinum toxin has been used 3 times over the past 4 years with diminishing effect. What is the most appropriate next step?
A. A fourth botulinum toxin injection — the previous injections were adequate management
B. Single-event multilevel surgery (SEMLS) — correcting all functional deformities simultaneously
C. Selective dorsal rhizotomy — this child's spasticity has not responded to BoNT-A
D. Intrathecal baclofen pump implantation — the most appropriate escalation in GMFCS II
Reveal Answer
Answer: B. Single-event multilevel surgery (SEMLS) — correcting all functional deformities simultaneously
This child now has multiple fixed structural deformities (fixed equinus, femoral anteversion) alongside dynamic deformities and crouch gait, and BoNT-A effect is waning — a signal that structural change has outpaced spasticity management. SEMLS is the standard surgical approach at this age (6–10 years) for ambulatory diplegic CP when multiple levels require correction: all procedures are performed in a single anaesthetic, minimising cumulative rehabilitation time and school disruption. SDR is not indicated here — this child is 8 years old (past the 4–7 year window), and has fixed contractures that would need to be addressed regardless. Intrathecal baclofen is reserved for GMFCS IV–V non-ambulatory patients with severe spasticity.
LMN versus UMN Paralysis: PPRP and CP Contrasted
The comparison between post-polio residual paralysis (LMN disease) and cerebral palsy (UMN disease) is a high-yield examination topic and a fundamental clinical distinction that changes every aspect of assessment and management. Understanding both conditions deeply is the goal of the neuromuscular cluster, and this contrast table consolidates the key differences.
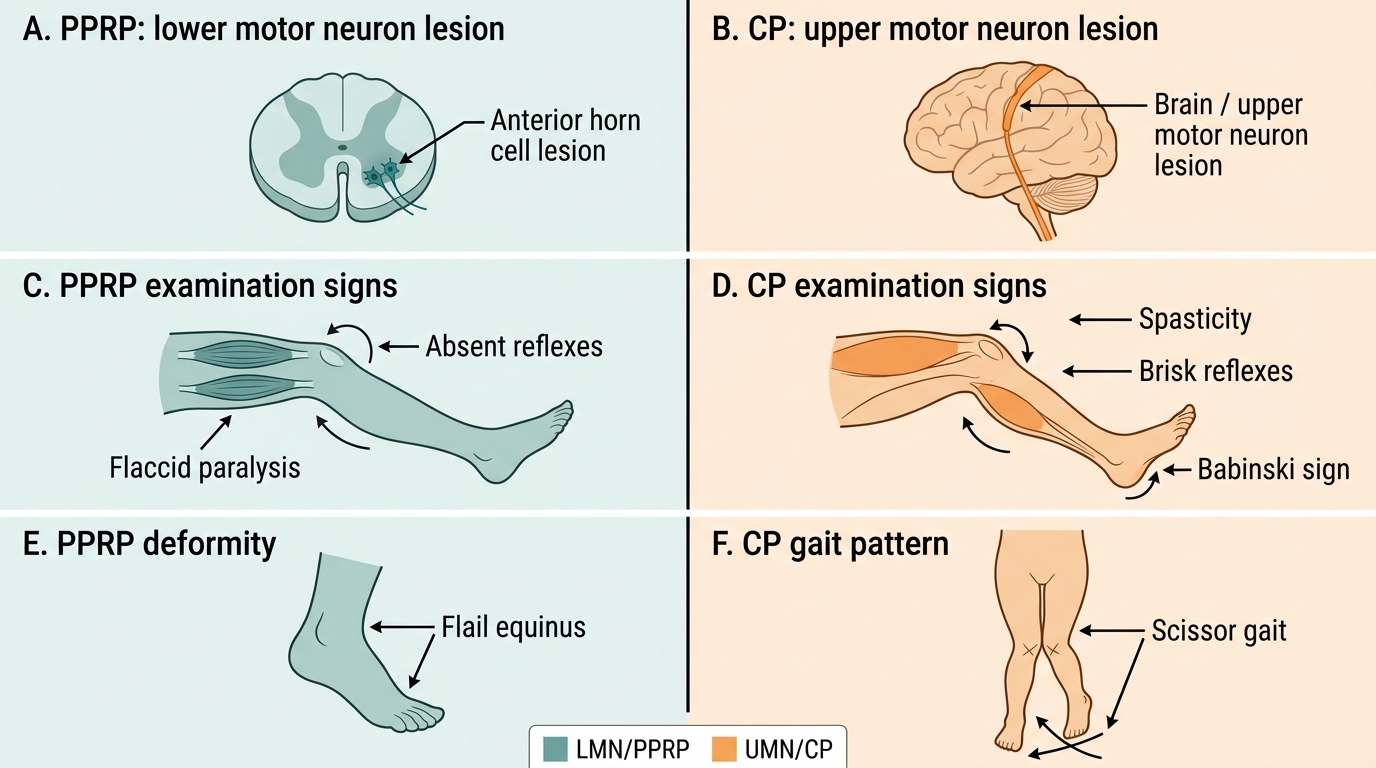
At the pathophysiological level, PPRP arises from destruction of the anterior horn cell (the lower motor neurone itself), whereas CP arises from damage to the upper motor neurone pathways in the brain before they reach the anterior horn cell. In PPRP, the motor neurone is destroyed and the muscle is denervated; in CP, the motor neurone and muscle are intact but are released from the normal supraspinal inhibitory control that suppresses reflexes and modulates tone.
Clinical examination findings differ sharply. In PPRP, tone is flaccid or absent; reflexes are absent because the efferent arc of the stretch reflex (the anterior horn cell and its axon) is destroyed; the plantar response is absent or flexor; and the affected limb shows prominent wasting because denervated muscle atrophies. In CP, tone is increased (spastic); reflexes are brisk and easily elicited; the plantar response is extensor (Babinski sign) because the corticospinal tract that normally suppresses the extensor response is damaged; and wasting is minimal because the muscle is continuously active (if over-active).
Deformity patterns also differ fundamentally. In PPRP, deformity is driven by unopposed antagonist pull into the direction of the stronger muscle (e.g. gastrosoleus intact → equinus when dorsiflexors paralysed). In CP, deformity is driven by spastic overactivity of specific muscles — the pattern is predictable from the spastic muscles, not the paralysed ones. PPRP deformities are typically flail or hypermobile joints; CP deformities are associated with stiff, spastic joints.
Management differences flow directly from these distinctions. PPRP management centres on tendon TRANSFER (moving a working muscle to substitute for a paralysed one — requires grade ≥4 donor) and arthrodesis. CP management centres on tendon LENGTHENING (releasing an overactive spastic muscle that is too short) and, in the ambulatory child, preservation of as much function as possible with the least invasive intervention that achieves the goal.
| Feature | PPRP (LMN) | Cerebral Palsy (UMN) |
|---|---|---|
| Site of lesion | Anterior horn cell (spinal cord) | Brain (cortex, white matter, BG) |
| Tone | Flaccid / absent | Spastic (increased) |
| Reflexes | Absent | Brisk, hyperreflexia |
| Plantar response | Absent / flexor | Extensor (Babinski) |
| Wasting | Prominent | Minimal |
| Sensation | Normal (motor neurone only) | Usually normal |
| Deformity driver | Muscle imbalance (paralysed vs intact) | Spastic muscle overactivity |
| Key surgery | Tendon TRANSFER (grade ≥4 donor) | Tendon LENGTHENING |
| Orthosis role | Substitutes for paralysed muscle | Holds position; stretches spastic muscle |
PPRP versus Cerebral Palsy