Page 7 of 17
EN4.5 | Ear Discharge — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with ear discharge, identifying features that distinguish its source and significance
- Describe the clinical features and otoscopic findings distinguishing safe (tubotympanic) from unsafe (atticoantral/cholesteatoma) chronic suppurative otitis media
- Choose appropriate investigations for ear discharge, including audiometry and CT temporal bones
- Describe the principles of medical and surgical management of the major causes of ear discharge
INSTRUCTIONS
Ear discharge (otorrhoea) is one of the most common ENT presentations globally and is the leading cause of preventable hearing loss in developing countries. The safe versus unsafe distinction in chronic suppurative otitis media is the single most important diagnostic judgment in ENT practice — it separates patients who can be managed medically from those who require surgery to prevent potentially fatal intracranial complications. This module gives you the conceptual framework and clinical tools to make this distinction reliably.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat, 8th ed., Ch. 9–11: Diseases of the Middle Ear, CSOM (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat and Head-Neck Surgery, 3rd ed., Ch. 9: Chronic Suppurative Otitis Media (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 3, Ch. 243–245: CSOM and Cholesteatoma (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-year-old boy is brought to your clinic by his mother with a six-month history of intermittent right ear discharge. He has had this problem since early childhood, she says, and it always gets better with eardrops. On this visit you note a small, foul-smelling crust in the postero-superior margin of the right pars tensa. You clean it and see a small marginal perforation with glistening white pearly debris visible behind it. His hearing test shows a 40 dB conductive hearing loss on the right. You diagnose CSOM and prescribe more ear drops. Six weeks later, his mother rushes him back — he has developed a facial palsy and is confused. A CT scan shows temporal bone erosion and an extradural abscess. Emergency surgery is performed that night. What was the critical missed diagnosis at the first consultation?
WHY THIS MATTERS
Chronic suppurative otitis media (CSOM) is the most prevalent chronic ear disease in developing countries, with an estimated 65–330 million people affected worldwide and a disproportionate burden in South Asia and Sub-Saharan Africa (Dhingra). In India, CSOM is the leading preventable cause of childhood hearing loss, with sequelae affecting education, communication, and employment across a lifetime. The two types of CSOM — tubotympanic ('safe') and atticoantral ('unsafe') — look superficially similar: both produce chronic ear discharge and hearing loss. However, the underlying pathology, the risk profile, and the management are fundamentally different. The unsafe (atticoantral) type, driven by cholesteatoma, erodes bone relentlessly, destroying the ossicular chain, the facial nerve canal, the semicircular canals, the dural plates, and the lateral sinus. Its complications — facial palsy, labyrinthitis, meningitis, brain abscess, lateral sinus thrombosis — are life-threatening. The NMC EN4.5 competency requires you to take a structured history, demonstrate clinical features, choose investigations, and describe management for ear discharge — and the safe-versus-unsafe distinction is the heart of that competency.
RECALL
Recall from your anatomy sessions the tympanic membrane (TM): it is divided into the larger central portion called pars tensa (in contact with the handle of the malleus, tightly stretched) and the smaller superior portion called pars flaccida or Shrapnell's membrane (in the attic, above the lateral process of the malleus, loosely attached). This anatomical distinction is the single most important landmark for classifying CSOM: a central perforation in the pars tensa (not reaching the annulus — the fibrocartilaginous rim of the TM) indicates tubotympanic disease; an attic perforation in the pars flaccida or a marginal perforation in the posterosuperior pars tensa (reaching the annulus) indicates atticoantral disease and suggests or confirms cholesteatoma. Also recall that the middle ear is bounded medially by the promontory (over the cochlea), the oval window (leading to the vestibule), and the round window; the facial nerve canal runs in the medial wall of the middle ear and over the oval window — explaining why cholesteatoma eroding the tegmen or medial wall can produce a facial palsy.
Clinical Presentation of Ear Discharge
A thorough clinical history for ear discharge requires characterising six dimensions of the discharge itself and then systematically asking about associated symptoms that reveal the extent of disease and any complications. This two-part structure is not merely a habit of thoroughness; it is the framework that generates the safe-versus-unsafe CSOM distinction at the bedside before any investigation is performed. An examiner who records only "ear discharge for months" and proceeds straight to the otoscope is operating without the contextual scaffolding that makes otoscopic findings interpretable. The character of the discharge, its associated features, and the patient's risk profile all combine to produce the pre-examination hypothesis that the otoscopic finding then confirms or refutes.
Characterising the discharge — six dimensions:
1. Duration and pattern: Acute otitis media resolves or perforates within days to weeks; CSOM by definition lasts longer than three months, often with a pattern of intermittent discharge. A pattern of discharge recurring every time the patient catches a cold or bathes (water entering via the perforation) strongly suggests CSOM tubotympanic type.
2. Character and consistency:
- Mucoid-purulent (stringy, yellowish): middle ear origin, mucosal disease — tubotympanic CSOM. The discharge arises from the hyperplastic middle ear mucosa.
- Foul-smelling, thick, cheesy or 'pearlescent': cholesteatoma — the foul odour is from the accumulation and breakdown of keratin debris; this combination of foul smell and thick discharge in the context of CSOM is the single most important red flag for unsafe disease.
- Watery, thin, scanty: otitis externa in its early stages, or — crucially — CSF otorrhoea after head trauma (especially if the patient also has anosmia or Battle's sign).
- Blood-stained: trauma, granulation tissue in chronic OE or unsafe CSOM, glomus jugulare tumour, or (rare and important) carcinoma of the middle ear.
- Thick white/black debris + pruritus: otomycosis (fungal OE) — the discharge is actually fungal mats, not true purulent discharge.
3. Laterality: Bilateral ear discharge is more likely to represent external ear disease or systemic conditions; unilateral chronic discharge points to a single anatomical site.
4. Associated hearing loss: Present in CSOM (conductive loss from TM perforation ± ossicular erosion). Sensorineural component in labyrinthitis complicating unsafe CSOM.
5. Associated otalgia: Pain is notably ABSENT in uncomplicated CSOM (both safe and unsafe) — this is a classic distinguishing feature. Onset of pain in a patient with established CSOM should immediately raise suspicion for a complication (extradural abscess, lateral sinus thrombosis, perilymph fistula).
6. Associated neurological symptoms: Vertigo (labyrinthine fistula or labyrinthitis), facial weakness (facial nerve erosion by cholesteatoma), headache and altered consciousness (intracranial extension — meningitis or brain abscess). Any of these in the context of ear discharge = neurosurgical emergency.
Key social history: nutritional status and socioeconomic background (CSOM is strongly associated with childhood malnutrition, overcrowded housing, and recurrent upper respiratory infections); previous ear surgery; swimming habits (water entry through perforation exacerbates discharge).
Anatomy and Pathophysiology of Ear Discharge
The type and significance of ear discharge are determined by which anatomical structure is generating it. This is not a theoretical point: the anatomy of the tympanic membrane directly predicts which kind of discharge the patient will have, whether bone erosion is occurring, and how dangerous the underlying process is. A clinician who understands the pathophysiology of pars tensa versus pars flaccida disease does not need to memorise the safe-versus-unsafe distinction as an isolated fact; they deduce it from first principles at the bedside. This section builds that pathophysiological understanding from structural anatomy upward, so that the clinical patterns described elsewhere in this module have a rational foundation rather than being a set of unconnected rules to memorise.
Tympanic membrane anatomy and CSOM type:
The TM comprises a peripheral fibrocartilaginous ring (annulus) and two distinct zones:
- Pars tensa: the larger central zone, bordered by the annulus, consisting of three layers: an outer squamous epithelial layer, a middle fibrous layer (the lamina propria), and an inner mucosal layer. The pars tensa is tightly stretched and has structural rigidity.
- Pars flaccida (Shrapnell's membrane): the small triangular area above the lateral process of the malleus, in the attic (epitympanum). It lacks the middle fibrous layer and is consequently loose and flaccid.
The pathological significance of this anatomy: perforation of the pars tensa results in exposure of the middle ear mucosa to the external environment → recurrent bacterial infection of the middle ear mucosa → tubotympanic CSOM (mucosal disease). The middle ear mucosa responds with hypertrophy and hypersecretion (hence the mucoid-purulent discharge), but cholesteatoma does not form from mucosal disease.
Why pars flaccida perforation leads to cholesteatoma:
The pars flaccida, being lax, may retract medially into the attic under negative pressure (caused by poor Eustachian tube function). As it retracts, it forms an attic retraction pocket lined by squamous epithelium. Squamous epithelium normally migrates laterally (self-cleaning), but in a deep retraction pocket, the desquamated keratin cannot escape — it accumulates as a cholesteatoma. A cholesteatoma is therefore an accumulation of desquamated stratified squamous epithelium (keratinous debris) within a sac of squamous epithelial lining in the middle ear or mastoid. It is not truly a tumour but behaves destructively via two mechanisms: (1) enzymatic bone erosion — the desquamating epithelium releases collagenase and other enzymes that directly erode adjacent bone; (2) pressure erosion from the expanding mass. This bone erosion destroys the ossicular chain (causing conductive hearing loss), the tegmen (roof of middle ear), the facial nerve canal, the semicircular canals, and the lateral sinus plate — leading to the potentially fatal complications.
CSF otorrhoea — different mechanism entirely:
Following a basal skull fracture involving the temporal bone (longitudinal temporal bone fracture is the commonest type), the cerebrospinal fluid can leak through the fracture line and the torn dural sleeve into the middle ear, and from there through a TM perforation or the Eustachian tube into the external ear or nasopharynx. This CSF otorrhoea appears as clear, watery fluid. The halo ring sign — applying the discharge to filter paper and seeing an outer ring of clear watery fluid around a central blood stain — suggests CSF contamination. The definitive diagnostic test for CSF otorrhoea is detection of beta-2 transferrin (a protein exclusive to CSF and not found in other body fluids except vitreous humour) by electrophoresis.
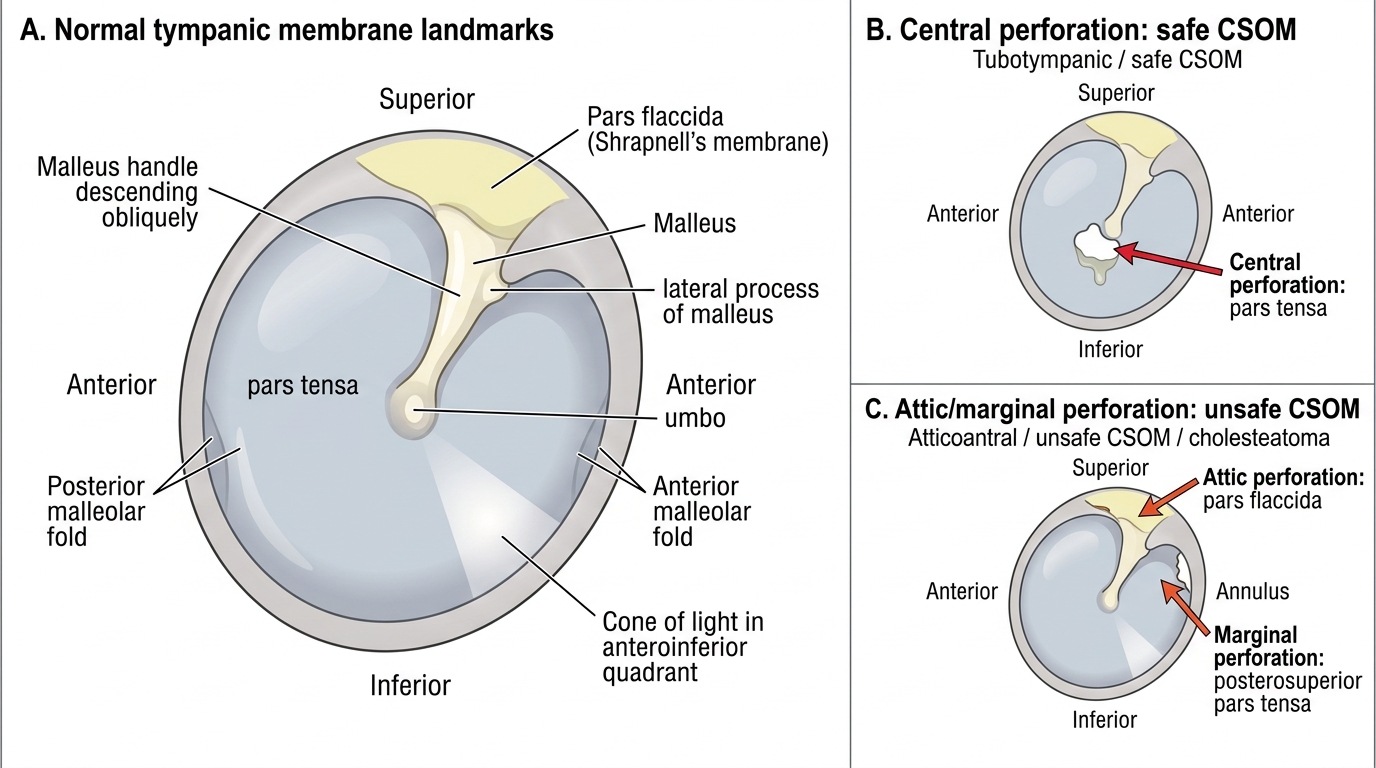
Tympanic Membrane Landmarks and CSOM Perforation Sites
SELF-CHECK
A 35-year-old man presents with a 10-year history of left ear discharge. Otoscopy shows a central perforation in the pars tensa with mucoid-purulent discharge. There is no attic crust, no foul odour, and no facial palsy. Audiometry shows a 35 dB conductive hearing loss. The most appropriate classification and initial management is:
A. Atticoantral (unsafe) CSOM: urgent mastoidectomy
B. Tubotympanic (safe) CSOM: aural toilet and topical antibiotics; surgical option is tympanoplasty when ear is dry
C. Acute otitis media: systemic antibiotics for 7–10 days
D. Cholesteatoma: CT temporal bones then surgical excision
Reveal Answer
Answer: B. Tubotympanic (safe) CSOM: aural toilet and topical antibiotics; surgical option is tympanoplasty when ear is dry
Central pars tensa perforation + mucoid-purulent discharge + no attic crust + no foul odour + no bone erosion signs = tubotympanic (safe/mucosal) CSOM. Initial management is conservative: aural toilet under microscopy to clean the canal, followed by topical antibiotic drops (ciprofloxacin drops are used in perforated ears — gentamicin drops are ototoxic in perforated ears). When the ear is brought to a dry state, elective tympanoplasty (Type I — myringoplasty alone) can repair the perforation and improve hearing. Mastoidectomy is not indicated for uncomplicated tubotympanic CSOM. CT is indicated for suspected unsafe CSOM or complications, not for straightforward safe CSOM.
ENT Examination and Investigation of Ear Discharge
The examination of a patient with ear discharge must be systematic, thorough, and conducted under good illumination — ideally using an oto-microscope or a headlight and pneumatic speculum. An examiner who relies on a hand-held auriscope alone may miss an attic crust or a small marginal perforation, and that missed finding can mean a missed cholesteatoma.
Examination sequence:
Step 1 — Inspect the auricle and post-auricular region:
Look for post-auricular swelling, tenderness, redness, or scar from previous surgery. A fluctuant post-auricular swelling in the context of CSOM = post-auricular abscess (extradural or subperiosteal), requiring urgent referral. Note if the pinna is displaced forwards and downwards (subperiosteal abscess from mastoiditis).
Step 2 — Otoscopy — the critical step:
Perform systematic otoscopy. First, clean the canal of any discharge or debris using a dry cotton wool carrier on a Jobson Horne probe, or microsuction. A canal obscured by discharge cannot be adequately assessed. After cleaning:
- Inspect the TM in all four quadrants. Identify the pars flaccida (attic) separately from the pars tensa.
- Look specifically in the postero-superior quadrant of the pars tensa (site of marginal perforations) and in the attic (pars flaccida) for crusting, retraction pockets, or pearly white debris (cholesteatoma matrix).
- Identify the perforation site (central pars tensa vs attic/marginal), its size and margins.
- Look for polyps (aural polyp arising from granulation tissue in CSOM) and granulation tissue.
- Test for fluctuation in an attic retraction pocket using a pneumatic speculum — a pocket that moves freely on positive pressure is a retraction pocket; one that does not suggests adhesion.
Step 3 — Cranial nerve examination:
Test facial nerve function (HB grading — forehead wrinkle, eye closure, smile, nasolabial fold, corner of mouth). Any facial nerve weakness in the context of CSOM = cholesteatoma eroding the facial nerve canal until proven otherwise → urgent surgical referral.
Step 4 — Tuning fork tests (512 Hz):
- Rinne test: negative (BC > AC) in conductive hearing loss from TM perforation or ossicular discontinuity.
- Weber test: lateralises to the affected ear (worse-hearing ear) in unilateral conductive hearing loss; lateralises to better ear in sensorineural hearing loss.
Investigations:
- Pure tone audiometry (PTA): quantifies the degree of hearing loss; distinguishes conductive (air-bone gap ≥ 15 dB) from sensorineural; essential for surgical planning. In CSOM, the air-bone gap reflects TM and ossicular chain status.
- EAC swab for culture and sensitivity: guides topical antibiotic selection in CSOM with active discharge; important to identify MRSA or quinolone-resistant Pseudomonas.
- CT scan of the temporal bones (high-resolution, HRCT): mandatory before surgery in suspected cholesteatoma — shows extent of disease, bone erosion, relationship to facial nerve canal and semicircular canals, tegmen integrity. Also indicated if complications are suspected.
- MRI with diffusion-weighted imaging (DWI): highly specific for cholesteatoma; a diffusion-restricted signal within the middle ear is virtually diagnostic. Useful for detecting residual cholesteatoma after surgery.
- Beta-2 transferrin assay: for suspected CSF otorrhoea (after head trauma or suspected meningocele).
- Biopsy: if carcinoma of the external or middle ear is suspected (blood-stained discharge, granular irregular lesion in elderly patient).