Page 8 of 17
EN4.5 | Ear Discharge — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The central diagnostic task in ear discharge is to correctly classify any case of CSOM as tubotympanic (safe) or atticoantral (unsafe/cholesteatoma), because this classification determines management. Every other diagnostic consideration — external ear causes, CSF otorrhoea, malignancy — follows secondary to this primary distinction.
Provided image
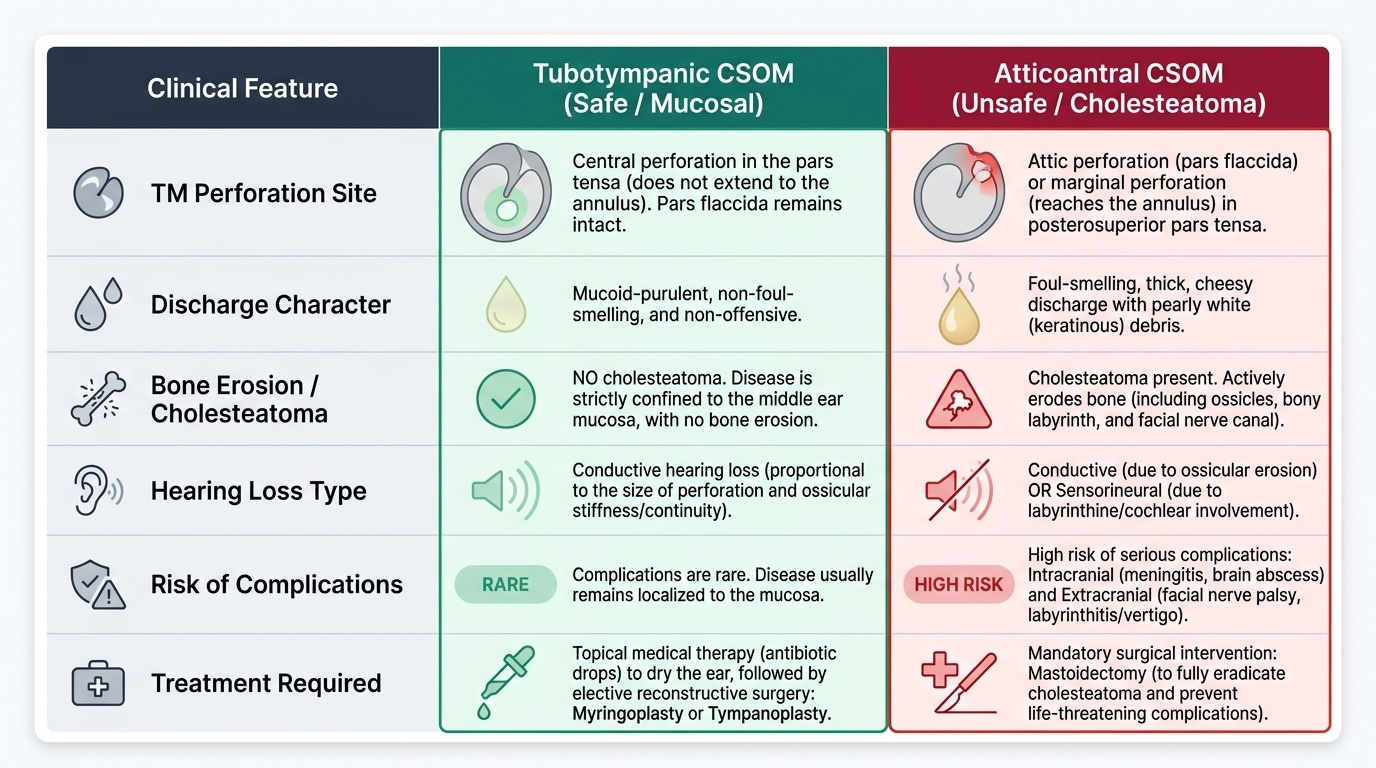
Tubotympanic (safe / mucosal) CSOM:
Characterised by a central perforation of the pars tensa — not extending to the annulus — with mucoid-purulent, non-foul-smelling discharge. The disease is confined to the middle ear mucosa. There is NO cholesteatoma. On examination, the TM shows a central hole with visible middle ear mucosa; the pars flaccida is intact; no attic crust or pearly debris is seen. Hearing loss is conductive, proportional to the size of the perforation and any ossicular involvement. COMPLICATIONS ARE RARE in tubotympanic CSOM. The condition responds partially to topical antibiotic treatment (bringing the ear to a dry state), but the perforation does not heal spontaneously. Definitive surgery: myringoplasty (Type I tympanoplasty) or Type II tympanoplasty (if ossicular reconstruction is needed).
Atticoantral (unsafe / squamosal) CSOM with cholesteatoma:
Characterised by an attic perforation (pars flaccida) or a marginal perforation in the posterosuperior pars tensa — i.e., a perforation that reaches the annulus — with foul-smelling, thick, cheesy discharge and pearly white (keratinous) debris. These findings indicate cholesteatoma. Even if the ear appears dry at one visit, the presence of an attic retraction pocket with crust should be treated as cholesteatoma until proven otherwise. This is the unsafe type because cholesteatoma erodes bone and can cause: (1) conductive hearing loss from ossicular erosion; (2) sensorineural hearing loss from labyrinthine erosion; (3) facial nerve palsy (erosion of bony facial nerve canal); (4) vertigo or labyrinthitis (semicircular canal erosion); (5) intracranial complications — meningitis, brain abscess (temporal lobe or cerebellar), extradural/subdural abscess, lateral (sigmoid) sinus thrombosis. The diagnosis of unsafe CSOM mandates surgery (mastoidectomy).
External ear discharge:
Otitis externa: EAC skin erythema, oedema, positive tragal sign, no TM perforation. Otomycosis: pruritus-predominant, fungal debris, KOH mount diagnostic. Furunculosis: localised tender boil in outer EAC.
CSF otorrhoea:
Clear, watery, profuse unilateral ear discharge after head trauma (or rarely with meningocele). Halo sign on filter paper. Beta-2 transferrin diagnostic. Associated with Battle's sign (post-auricular ecchymosis) or periorbital ecchymosis (raccoon eyes) from basal skull fracture.
Blood-stained discharge:
Trauma (temporal bone fracture — may coexist with CSF otorrhoea), granulation tissue in CSOM, glomus jugulare or tympanicum (vascular middle ear tumour — pulsatile tinnitus, otalgia), or — importantly — carcinoma of the middle ear (rare, elderly patients, blood-stained offensive discharge, granular EAC lesion, facial palsy, neck nodes; biopsy required).
SELF-CHECK
A 28-year-old woman has had left ear discharge for several years. Otoscopy after cleaning shows an attic crust in the pars flaccida region with foul-smelling whitish debris behind it. Audiometry shows a 50 dB conductive hearing loss. She has no facial palsy or vertigo. The correct management is:
A. Topical ciprofloxacin drops for 6 weeks
B. CT temporal bones followed by mastoidectomy
C. Oral amoxicillin for 2 weeks
D. Myringoplasty under local anaesthesia
Reveal Answer
Answer: B. CT temporal bones followed by mastoidectomy
Attic crust with foul-smelling debris in the pars flaccida = atticoantral (unsafe) CSOM with cholesteatoma. Management is CT temporal bones first (to define the extent of cholesteatoma and bone erosion, assess facial nerve canal and tegmen) followed by mastoidectomy (cortical, modified radical, or radical depending on CT findings and intraoperative extent of disease). Topical drops alone are not definitive for cholesteatoma — they may temporarily reduce discharge but cannot remove the cholesteatoma sac or halt bone erosion. Myringoplasty alone is only for tubotympanic CSOM after the ear is dry. This patient has unsafe CSOM and needs surgery.
Principles of Management of Ear Discharge
Management of ear discharge is driven entirely by the underlying diagnosis and follows a structured decision tree that mirrors the diagnostic framework built in the previous sections. At the first decision node: is the discharge from the external ear or the middle ear? If external, management follows the external ear disease principles. If middle ear, the second decision node is: is this safe (tubotympanic) or unsafe (atticoantral/cholesteatoma) CSOM? Safe disease allows a conservative approach with surgery reserved for elective repair of a dry ear. Unsafe disease mandates surgery regardless of the patient's preference or the apparent stability of symptoms, because cholesteatoma never becomes safer with watchful waiting; it continues to erode bone silently even between symptomatic episodes. The third and overriding decision node is: are complications present? Any complication of CSOM — intracranial extension, facial palsy, labyrinthitis, subperiosteal abscess — is a surgical emergency that must be managed urgently. The specific management strategies for each branch of this decision tree are described below.
Management of external ear discharge:
Aural toilet + topical antibiotic-steroid drops for bacterial OE; topical antifungal (clotrimazole) for otomycosis; systemic IV ciprofloxacin for malignant OE. These are covered in the External Ear Diseases module (EN4.2).
Medical management of tubotympanic (safe) CSOM:
The goal of medical treatment is to bring the ear to a dry state, which is the prerequisite for any surgical repair.
- Aural toilet under microscopy: microsuction to remove discharge and debris. This is essential before topical drops, as drops do not penetrate pus-filled ears.
- Topical antibiotic drops for active discharge: ciprofloxacin 0.3% drops (non-ototoxic, effective against Pseudomonas and Staphylococcus) are the drops of choice for perforated ears. Gentamicin and tobramycin drops are potentially ototoxic when the TM is perforated — cochlear toxicity from absorption through the round window membrane. Avoid aminoglycoside drops in perforated ears.
- Water precautions: protect the ear from water entry during bathing (cotton wool smeared with Vaseline, ear plugs). Water entering through the perforation introduces bacteria and perpetuates discharge.
- Systemic antibiotics: added for exacerbations with systemic features (fever, periauricular cellulitis) or for organisms not sensitive to topical treatment.
- When the ear is consistently dry for ≥3 months: elective surgical repair.
Surgical management of tubotympanic CSOM:
- Myringoplasty (Type I tympanoplasty): repair of the TM perforation using a graft (most commonly temporalis fascia). Closes the perforation, protects the middle ear from water and infection, and may improve hearing. Performed when the ear is dry for ≥3 months.
- Type II tympanoplasty: TM repair + ossicular chain reconstruction (if ossicular erosion has occurred). An ossiculoplasty is added to improve sound conduction.
Surgical management of atticoantral (unsafe) CSOM with cholesteatoma:
Surgery is mandatory for cholesteatoma. The goal is complete removal of the cholesteatoma sac to prevent further bone erosion and complications. Residual cholesteatoma invariably recurs and continues to erode bone.
- Cortical mastoidectomy (canal wall up): excavates the mastoid air cells while preserving the posterior bony EAC wall; requires second-look operation at 12 months to detect residual disease (as the intact canal wall prevents complete inspection). Better hearing preservation but higher recurrence.
- Modified radical mastoidectomy (canal wall down): removes the posterior EAC wall, creating an open mastoid cavity communicating with the EAC. Better access for complete cholesteatoma removal; lower recurrence rate; but creates a mastoid cavity that requires lifelong monitoring and cleaning at clinic (3–6 monthly). This is the most commonly performed procedure for unsafe CSOM in India.
- Radical mastoidectomy: removes all middle ear structures including ossicular chain and TM; reserved for extensive disease or recurrence. Results in significant conductive hearing loss; a hearing aid is usually required post-operatively.
Management of CSOM complications:
Complications of unsafe CSOM include extracranial complications (subperiosteal abscess, mastoiditis, Bezold's abscess, zygomatic abscess, petrositis, labyrinthitis, facial nerve palsy) and intracranial complications (extradural abscess, subdural abscess, brain abscess, meningitis, lateral sinus thrombosis, otitic hydrocephalus). These are neurosurgical emergencies: IV antibiotics (broad-spectrum to cover gram-negatives and anaerobes), neurosurgical or otosurgical drainage, and mastoidectomy as soon as the patient is fit for anaesthesia.
Management of CSF otorrhoea:
Head elevation, avoid nose blowing, prophylactic antibiotics are debated. Most traumatic CSF otorrhoea resolves spontaneously within 1–2 weeks. Persistent leak (>2 weeks): neurosurgical referral for intrathecal fluorescein localisation and surgical repair (duraplasty).
SELF-CHECK
In treating a patient with tubotympanic CSOM and active purulent discharge, the clinician prescribes topical drops to be instilled into the affected ear. Which of the following is the safest choice?
A. Gentamicin 0.3% drops
B. Ciprofloxacin 0.3% drops
C. Tobramycin-dexamethasone drops
D. Neomycin-polymyxin B drops
Reveal Answer
Answer: B. Ciprofloxacin 0.3% drops
In a perforated ear (as in CSOM), aminoglycoside drops — gentamicin, tobramycin, neomycin — are potentially ototoxic. They can be absorbed across the round window membrane into the inner ear and cause cochlear damage (sensorineural hearing loss) or vestibular toxicity. Ciprofloxacin 0.3% drops are safe in perforated ears, as quinolones are not ototoxic. Neomycin-polymyxin B drops are also ototoxic through the same round window route and should be avoided in perforated ears.
CLINICAL PEARL
The most dangerous mistake in CSOM management is treating an atticoantral (cholesteatoma) ear with topical drops alone and calling it 'safe CSOM.' The clues that distinguish unsafe from safe CSOM are: (1) the site of the TM perforation — attic (pars flaccida) or marginal (posterosuperior pars tensa) rather than central; (2) the character of the discharge — foul-smelling and cheesy rather than mucoid-purulent; (3) the presence of pearly white keratinous debris. Any ear with these features must be referred for CT temporal bones and surgical planning — it cannot be safely managed by topical drops alone, regardless of how long the patient has had it or how often they have been treated with drops.
Self-Assessment
The questions below target the most clinically important concepts from this module, with special emphasis on the safe versus unsafe CSOM distinction that forms the heart of the EN4.5 competency. Making this distinction correctly in a clinical examination or in clinical practice requires not just memory but structured pattern recognition: the ability to see a set of otoscopic findings and immediately categorise them into safe or unsafe disease, knowing instantly the management implications that flow from that categorisation. This module has given you the pathophysiological and anatomical foundation for that pattern recognition. The self-assessment below is designed to activate and consolidate it through retrieval practice without reference to notes. Research on deliberate practice in clinical education consistently shows that active retrieval — making a judgment, receiving feedback, adjusting the schema — is the most effective way to build reliable diagnostic judgment under the time pressure of clinical encounters. Each question below mirrors a real clinical scenario type where misclassification caused patient harm.
- What is the TM perforation site in tubotympanic CSOM? What is it in atticoantral CSOM? Why does this difference matter clinically?
- A patient with ear discharge develops a facial palsy. What does this indicate anatomically, and what is the urgent management?
- Which topical antibiotic drops are contraindicated in a perforated ear, and why? Name the specific drugs.
- What is the diagnostic test for CSF otorrhoea? What is the halo ring sign, and what causes it?
- Name three intracranial complications of atticoantral (unsafe) CSOM. Which cranial nerve is most commonly paralysed first by cholesteatoma, and why?
If you cannot name the three distinguishing features of unsafe CSOM (attic/marginal perforation, foul-smelling discharge, pearly cholesteatoma debris) you are carrying a clinically dangerous knowledge gap. Return to the diagnosis section and practice applying those three criteria to the cases in that section until they are automatic.