Page 1 of 29
EN4.12 | Acoustic Neuroma — SDL Guide
Learning Objectives
- Describe the clinical features of acoustic neuroma including the characteristic symptom sequence
- Explain the anatomy of the internal auditory canal and cerebellopontine angle relevant to acoustic neuroma
- List and interpret the investigations used to diagnose acoustic neuroma, including the gold-standard MRI
- Construct a differential diagnosis for cerebellopontine angle tumours
- Outline the three management options — observation, radiosurgery, and microsurgical excision — with their indications and outcomes
INSTRUCTIONS
Acoustic neuroma is the commonest tumour of the cerebellopontine angle and the paradigm case for unilateral progressive sensorineural hearing loss with vestibular symptoms in a young-to-middle-aged adult. This SDL is important because missing this diagnosis — attributing unilateral SNHL to ageing or noise exposure without investigating — delays treatment and risks facial nerve damage from a growing tumour. As a final-year student you are expected to recognise the presentation, know why MRI with gadolinium is the diagnostic gold standard, and understand the rationale for the three management choices.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 16 (Tumours of the Ear) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 243 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old software engineer presents to your ENT outpatient with a 2-year history of gradual hearing loss in the left ear. He had initially attributed it to stress and long hours with headphones, but is now concerned because he also has a persistent high-pitched ringing in the left ear and has noticed that he struggles on phone calls using that ear. On tuning-fork testing you find Rinne positive bilaterally, with Weber lateralising to the right. Pure-tone audiometry shows a left-sided high-frequency sensorineural hearing loss. What is the most important diagnosis to exclude, and what single investigation will confirm or exclude it?
WHY THIS MATTERS
Acoustic neuroma — more precisely called vestibular schwannoma — is the commonest tumour of the cerebellopontine angle, accounting for approximately 80% of all CPA tumours. It is a benign, slow-growing tumour, but 'benign' does not mean harmless: as it grows it can cause progressive and irreversible sensorineural hearing loss, facial nerve palsy, and eventually cerebellar and brainstem compression if untreated. The diagnosis is frequently delayed by 3–5 years because the early symptoms (unilateral tinnitus, gradually progressive unilateral SNHL) are common and often dismissed. Recognising the pattern — especially unilateral SNHL with tinnitus in a young or middle-aged adult — and requesting the right investigation (MRI with gadolinium) at the right time is one of the most important diagnostic decisions in ENT practice. Bilateral acoustic neuromas are pathognomonic of neurofibromatosis type 2 (NF2), a genetic condition with additional CNS tumour risks, making early diagnosis especially important in that context.
RECALL
Before reading further, recall the anatomy of the internal auditory canal (IAC) — a bony canal in the petrous part of the temporal bone that transmits four structures: the facial nerve (VII) anterosuperiorly, the cochlear nerve anteroinferiorly, the superior vestibular nerve posterosuperiorly, and the inferior vestibular nerve posteroinferiorly. A useful mnemonic is '7-UP, Coke-Down': VII and the cochlear nerve (the 'upper' of the hearing pair) anteriorly, vestibular branches posteriorly. Also recall the cerebellopontine angle (CPA) — the fluid-filled triangular cistern between the pons medially, the cerebellum posteriorly, and the posterior surface of the petrous bone anterolaterally. Numerous important structures pass through this cistern, including cranial nerves V, VI, VII, VIII, IX, X. Finally, recall from your tuning-fork training: in sensorineural hearing loss, Rinne is positive (AC > BC) and Weber lateralises to the better (contralateral) ear — do not invert this relationship.
Clinical Presentation of Acoustic Neuroma
The typical acoustic neuroma grows slowly — often over several years — and its symptoms reflect the progressive compression of structures within and adjacent to the internal auditory canal, followed by extension into the cerebellopontine angle. Understanding this growth sequence explains the characteristic symptom evolution that should alert a clinician to this diagnosis.
The three cardinal symptoms are: (1) unilateral sensorineural hearing loss, (2) unilateral tinnitus, and (3) vestibular disturbance. Of these, unilateral SNHL is the most common and usually the first to appear, often progressing gradually over months to years. The tinnitus is typically high-pitched, continuous, and unilateral — the unilaterality is a critical differentiating feature, as bilateral or alternating tinnitus suggests a different aetiology. Vestibular symptoms are often paradoxically mild despite the tumour's origin on the vestibular nerve; this is because slow growth allows central compensation to mask acute vertigo. Patients more commonly report vague imbalance, unsteadiness on turning, or mild disequilibrium rather than frank episodic vertigo.
As the tumour enlarges and extends into the CPA, additional cranial nerve involvement emerges. Facial nerve involvement (numbness or weakness of the face) is relatively late because the facial nerve is mechanically resilient and positioned anterosuperiorly in the IAC, away from the tumour's usual origin on the vestibular nerve. Trigeminal nerve (V) involvement produces ipsilateral facial numbness or paraesthesia and is a sign of significant CPA extension. Very large tumours compress the cerebellum (ipsilateral ataxia, dysmetria) and eventually the brainstem (long-tract signs, raised intracranial pressure with headache, diplopia). Sudden sensorineural hearing loss can rarely be the presentation — caused by tumour-related vascular compromise of the cochlear artery.
A classic examination finding is absent or reduced corneal reflex on the affected side (from V involvement before clinical facial numbness) and abnormal caloric response on vestibular testing. The audiogram typically shows high-frequency SNHL with disproportionate rollover on speech discrimination testing — the patient's speech discrimination score worsens at high intensities, which is characteristic of retrocochlear pathology and distinguishes it from cochlear disease.
Key clinical red flags for acoustic neuroma:
- Unilateral SNHL without a clear cause in a patient under 70
- Unilateral tinnitus, especially if progressive
- Asymmetric hearing loss on audiometry (>15 dB difference between ears at two or more frequencies)
- Poor speech discrimination disproportionate to the audiogram
- Absent stapedial reflex (retrocochlear pattern)
Anatomy and Pathophysiology
The term 'acoustic neuroma' is a misnomer on two counts: the tumour is not an 'acoustic' (cochlear) tumour, nor is it a true neuroma. It is correctly called a vestibular schwannoma — a benign tumour arising from Schwann cells of the vestibular division of the eighth cranial nerve, most commonly at the Obersteiner-Redlich zone, which is the transitional point between central (CNS glial) and peripheral (Schwann cell) myelin, located a few millimetres from the brainstem within the internal auditory canal. The vestibular nerve is preferentially affected over the cochlear nerve because it is more peripheral at this transition zone.
The internal auditory canal is approximately 8–10 mm long, running from the porous acusticus (the medial opening into the posterior cranial fossa) to the fundus (the lateral blind end within the petrous bone). Within the canal the four nerve bundles are arranged as described above, with a horizontal (falciform) crest and a vertical (Bill's bar) crest separating the compartments. The tumour typically originates on the superior or inferior vestibular nerve at or near the porous acusticus, then grows medially into the CPA cistern.
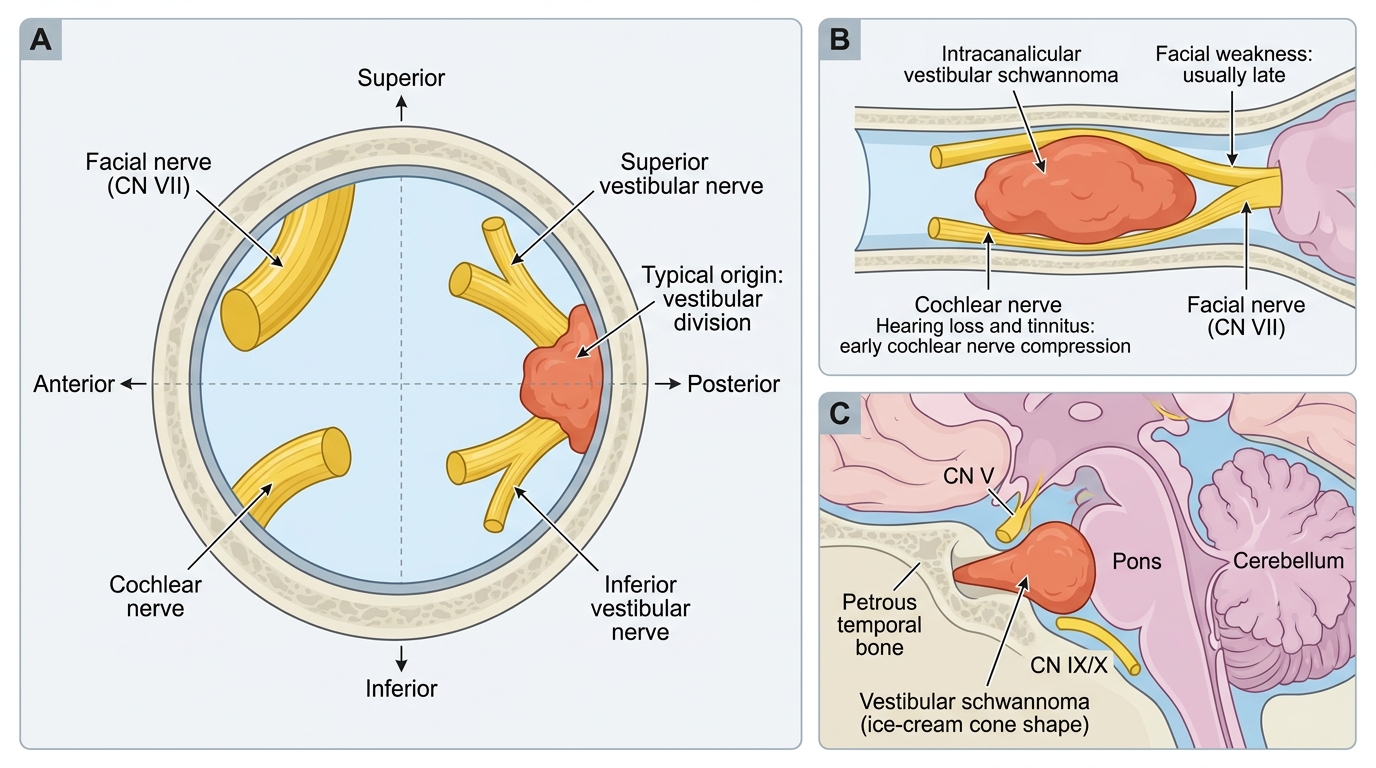
Internal Auditory Canal Nerve Positions and Acoustic Neuroma
As the tumour grows, it first fills the IAC, stretching the facial nerve (anterosuperior) and cochlear nerve against the bony walls of the canal — this explains why hearing loss and tinnitus are early symptoms (cochlear nerve compression) while facial weakness is relatively late (the facial nerve is more anteriorly situated and more mechanically resistant). When the tumour extends through the porous acusticus into the CPA cistern it adopts a characteristic 'ice-cream cone' shape — the intracanalicular component forms the cone and the CPA component forms the ball. The CPA cistern is surrounded by the pons medially, cerebellum posteriorly, and the petrous temporal bone anterolaterally; other cranial nerves (V superiorly, IX/X inferiorly) in this space explain the later neurological deficits.
Growth pattern: Most acoustic neuromas grow slowly — approximately 1–2 mm per year on average, though growth rates are highly variable and some tumours remain stable for decades. The slow growth allows central vestibular compensation, which is why balance disturbance is often subtle despite the tumour's vestibular origin. Approximately 40–50% of acoustic neuromas show no measurable growth over a 5-year observation period.
Bilateral acoustic neuromas are the defining feature of neurofibromatosis type 2 (NF2), an autosomal dominant disorder caused by mutations in the NF2 gene on chromosome 22q12, which encodes merlin (schwannomin), a tumour suppressor protein. NF2 typically presents in the second or third decade with bilateral hearing loss and should be suspected whenever acoustic neuroma occurs before age 30 or bilaterally.
SELF-CHECK
A 32-year-old woman presents with a 3-year history of gradually worsening unilateral tinnitus and hearing loss on the right side. Pure-tone audiometry shows right-sided high-frequency SNHL. Tuning-fork tests show Rinne positive on both sides, Weber lateralising to the left. The most appropriate next investigation is:
A. CT scan of the temporal bone with contrast
B. MRI brain with gadolinium, with attention to the IACs
C. Vestibular evoked myogenic potentials (VEMP)
D. Electrocochleography (ECoG)
Reveal Answer
Answer: B. MRI brain with gadolinium, with attention to the IACs
MRI brain with gadolinium (contrast-enhanced MRI with thin-section T1 sequences through the internal auditory canals) is the gold standard investigation for suspected acoustic neuroma. It detects tumours as small as 2–3 mm and characteristically shows an enhancing mass at the porous acusticus extending along the IAC into the CPA. CT of the temporal bone is useful for bony details and cochlear anatomy but is NOT the investigation of choice for detecting acoustic neuroma (soft tissue resolution is poor). VEMPs and ECoG are used in Meniere's disease and electrocochleography assessment, not for diagnosing acoustic neuroma.
Investigations
Investigating a suspected acoustic neuroma involves a structured stepwise approach: audiological assessment first, followed by imaging for confirmation. The sequence is important because audiological tests raise or lower the pre-test probability, and imaging — while definitive — is expensive and resource-intensive.
Provided image
Audiological investigations:
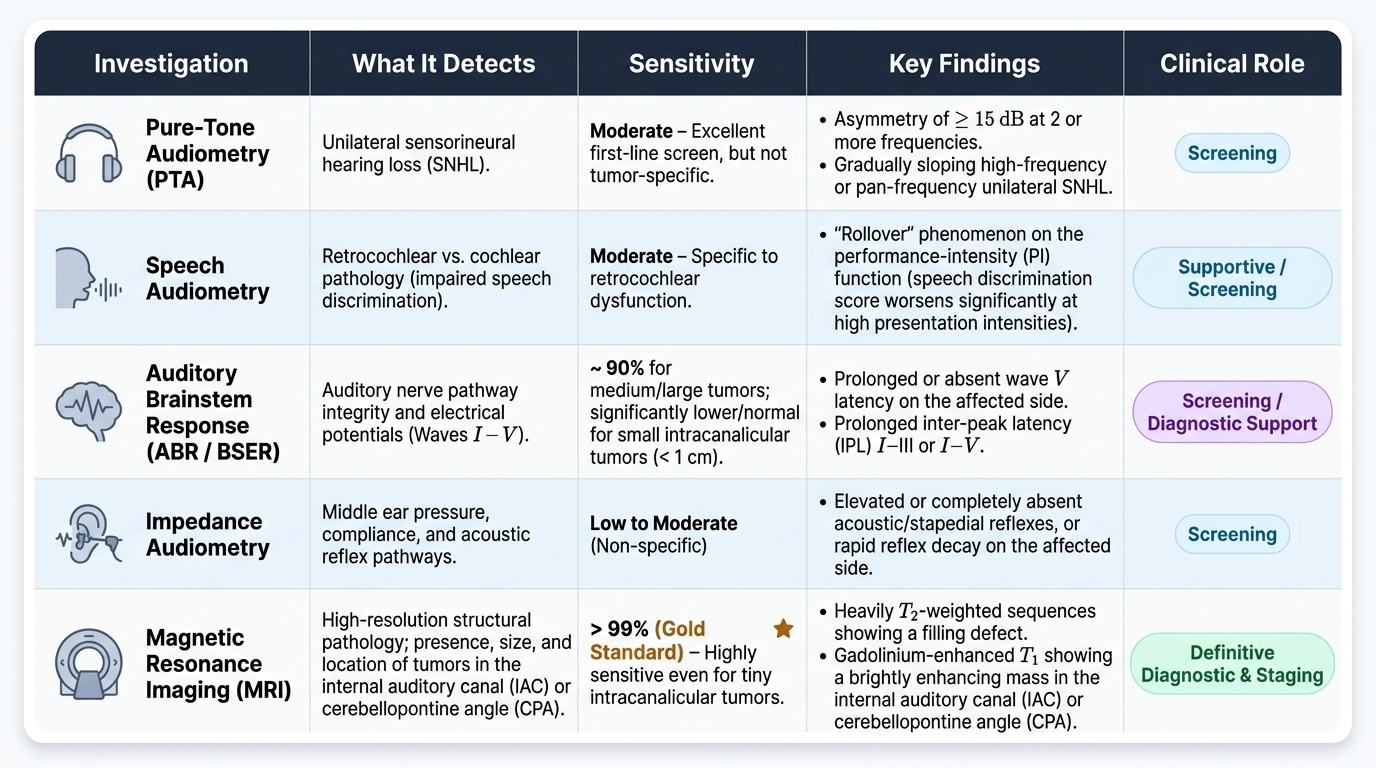
1. Pure-tone audiometry (PTA): The characteristic finding is a high-frequency or pan-frequency unilateral SNHL. An asymmetry of >15 dB between the two ears at two or more frequencies should always prompt further investigation. The pattern is typically a gradually sloping high-frequency loss.
2. Speech audiometry: A key discriminating feature of retrocochlear (vs cochlear) pathology is rollover on the performance-intensity (PI) function — speech discrimination score actually worsens at high presentation intensities. This is seen in acoustic neuroma and is not a feature of typical cochlear SNHL.
3. Auditory brainstem response (ABR / BSER): The ABR measures electrical potentials generated in the cochlea, VIII nerve, and auditory brainstem at five wave peaks (I–V). In acoustic neuroma, the characteristic finding is prolonged or absent wave V latency on the affected side, or a prolonged inter-peak latency (IPL) I–III or I–V. ABR has sensitivity ~90% for medium and large tumours but may be normal with small intracanalicular tumours.
4. Impedance audiometry: The stapedial reflex (acoustic reflex) tests the integrity of the reflex arc (VIII nerve → brainstem → VII nerve → stapedius). Acoustic neuroma classically produces an absent ipsilateral stapedial reflex or reflex decay at 500 Hz and 1000 Hz — a sensitive early indicator of retrocochlear pathology.
5. Caloric testing (ENG/VNG): Demonstrates canal paresis (reduced caloric response) on the affected side, confirming unilateral vestibular hypofunction. This is present in most cases.
Imaging — the gold standard:
MRI with gadolinium is the definitive investigation. Gadolinium-enhanced T1-weighted sequences with thin (1–2 mm) slices through the internal auditory canals demonstrate:
- An enhancing mass in the IAC and/or CPA
- The characteristic 'ice-cream cone' sign when there is both intracanalicular and CPA components
- Tumour size (critical for management planning)
- Relationship to brainstem and cerebellum
- Exclusion of other CPA tumours (meningioma, epidermoid)
MRI can detect tumours as small as 2–3 mm. It does not involve ionising radiation. The limitation is availability and cost in resource-limited settings.
CT of the temporal bone with contrast is used as an alternative or complement when MRI is contraindicated (cochlear implant, severe claustrophobia, pacemaker). High-resolution CT (HRCT) temporal bone shows bony erosion/expansion of the porous acusticus or IAC, and any intratumoral calcification (more typical of meningioma). It is less sensitive than MRI for small intracanalicular tumours.